Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
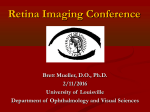
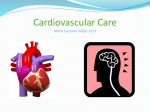
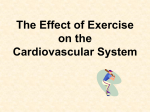
Grand Rounds Conference Brett Mueller, D.O., Ph.D. 6/17/2016 University of Louisville Department of Ophthalmology and Visual Sciences Patient Presentation CC: From Neurology attending: “My patient has blood in her eye.” HPI: 87 yo WF presented to the hospital with 2 hrs of L sided facial droop and L sided weakness. Received tissue plasminogen activator (tPA), and a repeat head CT demonstrated a 1.61 cm by 0.68 cm intraochemorrhage History POHx: Cataract surgery OU PMHx: Dementia, HTN, CAD, cerebral aneurysm s/p coiling, and an old stroke with residual L sided weakness FAMHx: none ROS: none MEDS: Lisinopril, statin, ASA, memantine ALLERGIES: none Head CT w/o Contrast Pre-tPA A Post-tPA B Hyperdense area in OD measuring 1.61 cm by 0.68 cm Exam VA Blink to light Blink to light EOM: Unable to obtain CVF: Unable to obtain 3--2 P 13 T 3--2 No APD 14 Exam OD OS LIDS/LASHES WNL WNL CONJ WNL WNL CORNEA WNL WNL IRIS WNL WNL LENS PCIOL PCIOL OD Fundus Photos OS Color fundus photos: OD: a large inferior suprachoroidal hemorrhage, subretinal hemorrhages and temporal hemorrhagic retinal detachment OS: nasal subretinal and suprachoroidal hemorrhage and multiple small intra-retinal hemorrhages, and a hemorrhagic retinal detachment Summary 87 y/o WF w/ bilateral suprachoroidal hemorrhages with hemorrhagic retinal detachments OD>OS, 2ndary to the administration of tPA for a nonhemorrhagic stroke PLAN: Observe Choroidal Effusion • Abnormal accumulation of fluid in the suprachoroidal space (between the sclera and choroid) • Common complications of glaucoma surgery, other intraocular surgeries, inflammatory and infectious diseases, trauma, neoplasms, and drug rxns, • Can be either serous (painless and can by asymptomatic) or hemorrhagic (painful and marked reduction in VA) Treatment of Choroidal Effusion • After glaucoma surgery choroidals are generally treated conservatively • If bleb is overfiltrating can taper steroids quickly to promote bleb scarring, and cycloplegic agents can be used to deepen the anterior chamber • Surgical drainage indications: flat anterior chamber, decreased vision, long-lasting choroidal effusions, appositional choroidals, and suprachoroidal hemorrhages Treatment of Choroidal Effusion • Surgical drainage is accomplished by performing a conj peritomy, a 2- to 3-mm radial incision is made in the sclera 3-4 mm posterior to the limbus • The incision is deepened until the suprachoroidal space is entered and fluid is released • The sclerotomy site is left open with closure of overlying conj Tissue Plasminogen Activator • Implicated in the treatment for blood clots: pulmonary embolism, MI, and stroke • Stroke: Guidelines recommend tx w/ tPA for all pts presenting with stroke like symptoms w/in a 3-4.5 hr window • PE: heparin commonly used, but if PE causes severe instability, then tPA is recommended • MI: tPA can be administered w/in 12 hrs of symptoms if pt cant get a cath tPA Causing Suprachoroidal Hemorrhages • Only reported in 5 case reports where patients were getting tPA for a MI • First reported case of a pt having a stroke who developed bilateral suprachoroidal hemorrhages after the administration of tPA • Neurologist need to be aware of this rare complication associated with tPA administration, as it may be more common than we think THANK YOU References 1) Chu TG, Green RL. Suprachoroidal hemorrhage. Surv Ophthalmol 1999; 43: 471-86 2) Barsam A, Heatley CJ, Herbert L. Spontaneous suprachoroidal hemorrhage secondary to thrombolysis for the treatment of myocardial infarction. Clin Experiment Ophthalmol. 2006;34:177e179 3) Khawly JA, Ferrone PJ, Holck DE. Choroidal hemorrhage associated with systemic tissue plasminogen activator. Am J Ophthalmol. 1996;121:577e578 4) Trikha S, Lockwood A, Puvanachandra N, Kirwan J. Acute suprachoroidal haemorrhage post-tenecteplase thrombolysis for myocardial infarction: management considerations. BMJ Case Rep. 2010 May 13;2010. pii: bcr1120092460. Doi: 10.1136/bcr.11.2009.2460. PubMed PMID: 22753301; PubMed Central PMCID:PMC3047514. 5) Asensio Sánchez VM, Pérez Flández FJ, Carlos Bejarano J, Merino Núñez F.Suprachoroidal haemorrhage and acute glaucoma associated with systemic fibrinolysis. Arch Soc Esp Oftalmol. 2002 Aug;77(8):459-61. Spanish. PubMed PMID: 12185623. 6) Chorich LJ, Derick RJ, Chambers RB, Cahill KV, Quartetti EJ, Fry JA, Bush CA. Hemorrhagic ocular complications associated with the use of systemic thrombolytic agents. Ophthalmology. 1998 Mar;105(3):428-31. PubMed PMID: 9499772. 7) Lopez AD, Mathers CD, Ezatti M, Jamieson DT, Murray DJL. Global burden of disease and risk factors. New York/Washington: Oxford University Press and the World Bank; 2006 8) Mackay J, Mensah G. The atlas of heart disease and stroke. Geneva: WHO; 2004 9) Saver J, Fonarow G, Smith E, Reeves M, Grau-Sepulveda M, Pan W, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309(23):2480–8 10) Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–29The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995; 333:1581–1587. 11) Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359:1317–1329.Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke. The NINDS t-PA Stroke Study Group. Stroke. 1997 Nov;28(11):2109-18. PubMed PMID: 9368550. 12) Chu TG, Green RL. Suprachoroidal hemorrhage. Surv Ophthalmol. 1999;43:471–486. 13) Chak M, Williamson TH. Spontaneous suprachoroidal haemorrhage associated with high myopia and aspirin. Eye.2003;17:525–527. References 14. Kim MH, Koo TH, Sah WJ, Chung SM. Treatment of total hyphema with relatively low-dose tissue plasminogen activator. Ophthalmic Surg Lasers1998; 29: 762–766. | PubMed | ISI | ChemPort | 1.Lundy DC, Sidoti P, Winarko T, Minckler D, Heuer DK. Intracameral tissue plasminogen activator after glaucoma surgery. Indications, effectiveness, and complications. Ophthalmology1996; 103: 274–282. | PubMed | ISI | ChemPort | 15. Jaffe GJ, Lewis H, Han DP, Williams GA, Abrams GW. Treatment of postvitrectomy fibrin pupillary block with tissue plasminogen activator. Am J Ophthalmol 1989; 108: 170–175. | PubMed | ISI | ChemPort | 16. Williams GA, Lambrou FH, Jaffe GA, Snyder RW, Green GD, Devenyi RG et al. Treatment of postvitrectomy fibrin formation with intraocular tissue plasminogen activator. Arch Ophthalmol1988; 106: 1055–1058. | PubMed | ISI | ChemPort | 17. Jaffe GJ, Abrams GW, Williams GA, Han DP. Tissue plasminogen activator for postvitrectomy fibrin formation. Ophthalmology 1990; 97: 184–189. | PubMed | ISI | ChemPort | 18. Heiligenhaus A, Steinmetz B, Lapuente R, Krallmann P, Althaus C, Steinkamp WK et al. Recombinant tissue plasminogen activator in cases with fibrin formation after cataract surgery: a prospective randomised multicentre study. Br J Ophthalmol 1998; 82: 810–815. | Article | PubMed | ISI | ChemPort | 19. Siatiri H, Beheshtnezhad AH, Asghari H, Siatiri N, Moghimi S, Piri N. Intracameral tissue plasminogen activator to prevent severe fibrinous effusion after congenital cataract surgery. Br J Ophthalmol 2005; 89: 1458– 1461. | Article | PubMed | ISI | ChemPort |