Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Take Your Coding to the
Next Level—Clinical
Frankie Jackson, MSHA, RN, CCS
Director, Clinical Consulting, JA Thomas, Atlanta, GA
Michelle Custodio, BS, RHIA, CCDS, CDIP
System CDI Program Manager, Banner Health System, Chandler, AZ
Slide credit: Vickie Balistreri, BA, RHIA, CCS, CCDS,CCS-P, CPC,CPCH, AHIMA-Approved ICD-10-CM/PCS Trainer
Topics
• Operative reports:
– Complication: Liver laceration
– Common duct exploration
– Incision into cystic duct and/or milking of the Sphincter of
Oddi
– Gallbladder hydrops
– Perforated appendix with sepsis
– MAZE procedure
– Complication: Coronary dissection
• Clarification opportunities from a clinical perspective
– Radiology & pathology reports; cultures
• Clarification opportunities for other documentation of clinical
significance
– BMI; dietary; wound
Operative Reports
• Complication: Liver laceration
• Laparoscopic and/or open cholecystectomy:
– Common duct exploration
– Incision into cystic duct and/or milking of the
Sphincter of Oddi
• Gallbladder hydrops
• Perforated appendix with sepsis
Complication: Suture of Liver
Laceration = 50.61
Liver bed: Bleeding from the liver bed may be encountered
when the wrong plane is developed during dissection of
the gallbladder
Patients who have portal hypertension, cirrhosis, or
coagulation disorders are at particularly high risk
Op note examples:
• “I inadvertently nicked the liver requiring 3 sutures to
stop the bleeding”
• “During the removal of the gallbladder, friable liver bed
started to hemorrhage, requiring conversion to open
chole with cautery and suture hemostasis to control
bleed”
ACS Surgery: Principles and Practice-GASTROINTESTINAL TRACT AND ABDOMEN 21
CHOLECYSTECTOMY AND COMMON BILE DUCT EXPLORATION
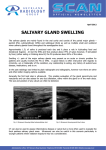
Gallbladder, Common Bile Duct,
Cystic Duct, Common Hepatic Duct
Operative Note: Gallstones, Stone Location
May Result in Additional Procedure(s)
Laparoscopic and/or open cholecystectomy:
• Exploration of common bile duct (51.51)
• Incision into common bile duct or milking of
Sphincter of Oddi (51.59)
Source: Wikipedia Creative Commons
http://en.wikipedia.org/wiki/File:Gallensteine_2006_03_28.JPG
Common Bile Duct
Source: Wikipedia Creative Commons
http://en.wikipedia.org/wiki/Common_bile_duct
Common Duct Exploration
• Preoperative magnetic
•
•
•
•
•
resonance
cholangiopancreatography
shows surgeon abnormal
anatomy and presence of stones
in the distal common bile duct
(CBD)
Acc = accessory duct entering
the common hepatic duct near
the neck of the gallbladder
CHD = common hepatic duct
Duo = duodenum
GB = gallbladder, containing
stones; LHD = left hepatic duct
PD = pancreatic duct; RHD =
right hepatic duct
Common Bile Duct Exploration
= 51.51
Large stones (> 1 cm), as well as most stones in the
common hepatic ducts, are not retrievable with the
techniques described above.
•Ductal clearance can be achieved via
choledochotomy if the duct is dilated. A small
longitudinal choledochotomy (a few millimeters longer
than the circumference of the largest stone) is made
with curved micro-scissors on the anterior aspect of
the duct while the stay sutures are elevated. A
choledochoscope is then inserted, and warm saline
irrigation is initiated. In most cases, baskets should
suffice for stone retrieval.
Incision Into Cystic Duct and/or
Milking of the Sphincter of Oddi = 51.59
Cystic duct stones: Stones in the cystic duct may be
visualized or felt during laparoscopic cholecystectomy.
If stones are in the cystic duct, they should be milked into
the gallbladder before applying clips.
Placing a clip across a stone may push a fragment of the
stone into the CBD and will increase the risk that the clip
will become displaced, leading to a bile leak.
If the stone cannot be milked into the gallbladder, a small
incision can be made in the cystic duct (as is done for
cholangiography), and the stone can often be expressed
and retrieved.
Correction, Incision of Cystic Duct
From Coding Clinic, 2Q 1997, p. 16
Correction, incision of cystic duct
• The appropriate code for incision of cystic duct
is 51.59, Incision of other bile duct
• Code 51.51, Exploration of the common duct, is
for the common duct only
Gallbladder Hydrops
HPI: 74-year-old female who presented with epigastric pain and
elevated liver enzymes. VS: T 37.7, HR 67, 135/89, O2 sats
97%.
PMH: HTN, CAD s/p CABG, Hx of aortic stenosis. Hx of CA of
uterus, s/p resection.
DIAGNOSTICS: Last set of labs from transfer hospital showed:
WBC 12.3, creatinine 1.2, glucose 124, BUN 21, total bili 1.1,
alkaline phosphatase 206, GOT 545, GPT 269, anion gap 19,
amylase 64. 85% segs, troponin neg- 2 sets. 03/04 MRI of
abdomen: sludge in the gallbladder with a 13 mm calculus
located in the distal common bile duct with
associated intra and extrahepatic biliary dilatation.
MRCP: choledocholelithiasis with a 13 mm calculus
in the distal common bile duct with associated
intrahepatic and extrahepatic biliary dilatation.
Distended gallbladder with possible small stone in
the gallbladder neck.
Hydrops of Gallbladder and Adhesions
From Coding Clinic, 2Q 1989, p. 13
• Hydrops of the gallbladder (also known as mucocele),
575.3, refers to cystic duct obstruction with gallbladder
distention, usually due to gallstones. Since there are no
exclusion notes under code 575.3, hydrops can be
coded when it is mentioned in the diagnosis.
• Examples
– Codes 574.0 and 574.1, calculus of gallbladder, include calculus
of cystic duct and there is a fifth digit 1 for obstruction. Calculus
of gallbladder with cystic duct obstruction and hydrops of
gallbladder may be coded as 574.01 (or 574.11) and 575.3.
– Calculus of the cystic duct with hydrops of the gallbladder is
coded 574.21 and 575.3.
– Hydrops of the gallbladder due to adhesions is coded 575.3.
Perforated Appendix With
Sepsis
• Patient presents from ECF with severe
abdominal pain, N/V with reports of fever spike
of 103 day prior to admission
• Diagnostics:
– Labs: Lactic acid 2.5 –H, WBC -20.0 w/left
shift, seg 90%
– X-ray: Acute appendicitis suspicious for
perforation-extensive inflammatory changes in
the R lower abdomen and pelvis.
• ED: Acute appendicitis
• H&P: Acute appendicitis w/perforation
Perforated Appendix With
Sepsis
• Preoperative DX: Perforated appendicitis with
severe inflammatory changes and “large
pockets of purulent fluid within pelvis and right
abdomen necessitating partial cecectomy for
good viable tissue at staple line”
• Treated with partial cecectomy, IV Zosyn,
Vancomycin, and Flagyl
• Progress notes report atrial fib secondary to
infectious process and reports of persistent
leukocytosis
Perforated Appendix With
Sepsis
• Suggestions:
–ER – look at initial VS
–Look at nursing notes for first 12 hours:
• Spikes of BP or hypotension
• Meds given
• Lactic acid
• High white blood cell count
Perforated Appendix With
Sepsis
• Opportunity:
–PDX clarification for unspecified
septicemia POA
• Original DRG 331: FY 12 RW 1.6254
– Pdx: Acute appendicitis w/peritoneal abscess
– Px: Lap cecectomy
• Revised DRG 853: FY 12 RW 5.4668
– Pdx: Unspecified septicemia
– Px: Lap cecectomy
• RW difference: 3.8414
Operative Reports: Cardiac
• MAZE procedure
• Complication: Coronary dissection
Source: Wikipedia Creative Commons
http://en.wikipedia.org/wiki/File:Labyrint_barvaux.jpg#filelinks. Used with permission.
MAZE Procedure
Definition: MAZE heart surgery: Complex procedure to
treat atrial fibrillation. During the procedure, a number of
incisions are made on the left and right atrium to form scar
tissue, which does not conduct electricity and disrupts the
path of abnormal electrical impulses. The scar tissue also
prevents erratic electrical signals from recurring. After the
incisions are made, the atrium is sewn together to allow it
to hold blood and contract to push blood into the ventricle.
•MAZE is used because the result looks like a maze in
which there is only one path that the electrical impulse can
take from the SA node to the AV node. The atrium can no
longer fibrillate, and sinus rhythm (the normal rhythm of the
heart) is restored.
MAZE Procedure: How Is It
Performed and Why?
MAZE can be performed either through an open chest
procedure or a minimally invasive procedure.
•90% of MAZE surgeries are concomitant (done in
conjunction) with other open chest surgery, such as
coronary artery bypass grafting, mitral valve repair, and/or
valve replacement
•Minimally invasive MAZE surgery (beating heart) is
performed through small keyhole incisions made between
the ribs, through which a tiny camera and video-guided
instruments are inserted. When appropriate, robotics are
used to assist the surgeon during the procedure.
Reason performed: The Cox MAZE III Procedure is now
considered to be the "gold standard" for effective surgical
cure of AF.
MAZE Procedure
Risk of mortality: The overall operative mortality for
patients undergoing the MAZE procedure is 3%. The
mortality rate increases among patients over age 65. Atrial
fibrillation is not immediately life-threatening, but it can
lead to other heart rhythm problems. Follow-up data from
the Framingham Heart Study and the Anti-Arrhythmia
Versus Implantable Defibrillators Trial have shown that
atrial fibrillation is a predictor of increased mortality.
•According to a 2002 study published in the New England
Journal of Medicine, controlling a patient's heart rate is as
important as controlling the patient's heart rhythm to
prevent death and complications from cardiovascular
causes.
MAZE Procedure
From Coding Clinic, 4Q 2003, pp. 93–95
• Effective October 1, 2003, changes have been made to
distinguish between MAZE procedures performed via
an open chest approach (37.33) and an endovascular
approach (37.34)
Complication:
Coronary Dissection
• Scrutinize the operative/procedure note to see if
a coronary dissection was documented and the
degree or type of dissection
• Query or clarify with the physician if the
coronary dissection is a complication or an
expected outcome due to tortuous vessels, etc.
Complication:
Coronary Dissection
• Type A dissections represent minor radiolucent areas within the
•
•
•
•
•
coronary lumen during contrast injection with little or no persistence
of contrast after the dye has cleared.
Type B dissections are parallel tracts or a double lumen separated
by a radiolucent area during contrast injection, with minimal or no
persistence after dye clearance.
Type C dissections appear as contrast outside the coronary lumen
("extraluminal cap") with persistence of contrast after dye has
cleared from the lumen.
Type D dissections represent spiral ("barbershop pole") luminal
filling defects, frequently with excessive contrast staining of the
dissected false lumen.
Type E dissections appear as new, persistent filling defects within
the coronary lumen.
Type F dissections represent those that lead to total occlusion of the
coronary lumen without distal antegrade flow. In rare cases, a
coronary artery dissection may propagate retrograde and involve
the ascending aorta.[8]
Complication:
Coronary Dissection
• Numerous studies performed prior to the
common use of stents found that, in general,
type A and B dissections are clinically benign
and do not adversely affect procedural outcome.
However, types C through F are considered
major dissections and carry a significant
increase in morbidity and mortality.
– Jason H. Rogers, MD* and John M. Lasala, MD, PhD§Divisions of Cardiovascular Medicine: *University of California, Davis Medical Center,
Sacramento, California and §Washington University School of Medicine, Saint Louis, Missouri
Dissection of Artery Occurring During
Coronary Angioplasty
From Coding Clinic, 1Q 2011, pp. 3–4
Question: “… A patient underwent coronary angioplasty with stent
deployment. During the procedure, the patient developed chest pain
and ST-segment changes. Angiogram revealed a dissection throughout
the proximal mid-portion of the vessel … Additional arteriogram
revealed control of the dissection and a widely patent vessel. When
queried, the provider indicated that the dissection was a complication
of the procedure. … What is the correct diagnosis code
assignment for a clinically significant dissection occurring
during PTCA?”
Answer:
• Assign code 997.1, Cardiac complications, since the provider
has documented that the dissection was a complication of
percutaneous coronary intervention (PCI).
• Assign code 414.12, Dissection of coronary artery, to further
describe the complication …
Dissection of Artery Occurring During
Percutaneous Coronary Intervention
From Coding Clinic, 1Q 2011, p. 4
Question: This patient with known coronary artery
disease (CAD) is admitted for percutaneous
coronary intervention. The operative report states,
“a kissing balloon angioplasty was also carried out
due to plaque migration. This was associated with a
small dissection in the native right coronary artery
just distal to the stent. Because of this a 12/2.5
millimeter drug eluting stent was placed in the distal
right coronary artery extending to the left ventricular
branch and jailing the posterior descending
coronary artery.” What is the appropriate code for
the dissection?
Dissection of Artery Occurring During
Percutaneous Coronary Intervention
From Coding Clinic, 1Q 2011, p. 4
• Answer: Query the provider regarding the
clinical significance of the dissection. The
insertion of a stent as a result of the dissection
does not automatically mean that the dissection
is clinically significant. If the provider confirms
that the dissection is a complication of the
procedure, assign code 997.1, Cardiac
complications, with code 414.12, Dissection of
coronary artery, to further describe the
complication. If the provider indicates that the
dissection is not clinically significant, do not
assign a code.
Arterial Dissection
From Coding Clinic, 4Q 2002, pp. 54
• Arterial dissection: New codes have been created to allow
data capture of dissection of the carotid, coronary, iliac, renal,
vertebral and other arteries.
• Arterial dissection is defined as blood coursing within the
layers of the arterial wall. The term dissecting aneurysm is a
misnomer. A dissection is not an aneurysm. True aneurysms
involve dilatation of all three arterial wall layers. Arterial
dissections are common complications of interventional
procedures, but they may also occur spontaneously.
Dissection of carotid artery 443.21
Dissection of coronary artery 414.12
Dissection of iliac artery 443.22
Dissection of renal artery 443.23
Dissection of vertebral artery 443.24
Dissection of other artery 443.29
Clarification Opportunities
From a Clinical Perspective
• Radiology reports
–Acute interstitial pneumonia/pneumonitis
–Cerebral edema
• Pathology reports
–Transbronchial biopsy of lung
• Cultures
–A/H1N1 influenza
–Organism on sputum
Radiology Reports: Acute
Interstitial Pneumonia/Pneumonitis
HPI: 91-year-old male who presents w/wheezing and coughing w/green
sputum.
VS: 133/67, T 36.8, HR 98 slightly irregular, RR 18, sats 94% on ra.
PMH: Recurrent PNA. Lymphoma in groin for which he received chemo
last summer, nothing since. Hx of multi tropical infections while he was
in the service including dengue fever, malaria, yellow fever, and jungle
rot. Hx of irrregular heartbeat. Hx of TIA and amaurosis fugax. Hx of
esophageal stricture and hiatal hernia.
DIAGNOSTICS: WBC 6.2, hgb 12.3, 16% monos, Na 133, creatinine 1.49,
albumin 3.8.
03/24: "bilateral reticular opacities with ground glass opacity of
the right posterior costophrenic sulcus. Findings could
represent either aspiration, pneumonia, vs acute infection on
chronic fibrosis.” 03/25: CT of thorax: 13 mm bleb in right middle
lobe. Mild subsegmental atelectasis vs. early infiltrate at the bilateral
lower lobes. Mediastinal lymph nodes measuring up to 11 mm...may be
reactive.”
Radiology Reports: Interstitial
Pneumonia
ED: Wheezing, pneumonia.
H/P: Bibasilar infiltrates consistent with pneumonia with bronchial
hyperreactivity. 2 cm opacity on chest x-ray. HTN. Hx of recurrent
aspiration due to esophageal stricture. Hx of lymphoma, in remission.
Coumadin therapy. Hx of arrhythmia. CT of chest as appearance of
the pneumonia is atypical and there is also a small opacity.
Could correspond to an old lymphoma nodule or hx of valley fever. Also
a possibility of pulmonary fibrosis.
PROGRESS NOTES: 03/25-URI with RAD, cocci pending. Neutropenia.
CONSULTS: 03/25-Suspect upper respiratory infection with
bronchospasm. Reactive airway disease. Cough. Wheezing. Hx of
lymphoma. d/c solumedrol, start prednisone.
Treatment: IV solumedrol, IV azithromycin, IV Rocephin
Swallow study: Passed swallow study. Able to swallow thin liquids.
Acute Respiratory Failure Due to
Mycoplasma Pneumonia
From Coding Clinic, Nov-Dec 1987, pp. 5–6
Question:
The physician's diagnosis is "Acute respiratory failure
due to acute bilateral interstitial pneumonia due to
Mycoplasma organism?" The discharge summary
states: "Since we could not culture anything and since
Legionella antibodies were negative, it was presumed
that his pneumonia was due to Eaton's agent and he
was given erythromycin as part of his antibiotic program
with final improvement in the pneumonia and hypoxia." It
was felt that the use of two codes was indicated, 136.3
for acute interstitial pneumonia and 483 for Mycoplasma
pneumonia, to show the type of pneumonia as well as
the organism. Is this correct coding?
Acute Respiratory Failure Due to
Mycoplasma Pneumonia
From Coding Clinic, Nov-Dec 1987, pp. 5–6
Answer:
No. The correct code assignments are:
• 518.81 Respiratory failure
• 483 Pneumonia due to other specified organism
(Mycoplasma)
• Code also any ventilation therapy and any temporary
tracheostomy performed
The medical record indicated that the reason for admission
was the acute respiratory failure, and for this reason it is the
principal diagnosis. The "interstitial" stated in the diagnosis
may refer to the Mycoplasma infiltrates noted on the chest xrays. Code 136.3 is assigned to Pneumocystis carinii
pneumonia, which is a parasitic infection occurring in
debilitated or immunodeficient patients. It would not be
assigned in this particular case where the presumed cause of
the pneumonia is due to an Eaton's agent, an endemic type
of infection, 483. You may wish to ask the physician for
further clarification of "interstitial" relating to his diagnosis of
pneumonia.
Cerebral Edema:
Radiology Report
HPI: 79-year-old female seen in office with increasing speech difficulty and
right-sided weakness.
VS: 36.7, HR 94, RR 19, O2 sats 95%, 185/85
PMH: Sentinel node CA in breast resulting in mastectomies in October of
2009, right gamma scanning.
HOME MEDS: Decadron 4 mg 4 times daily. Bumex, Tarka, Toprol XL,
clonidine, Nexium, Compazine, Xanax, allegra. Combivent inhaler,
DuoNeb SVN txs at home, ASA, Plavix.
DIAGNOSTICS: Hemoglobin 13.4, WBC 9.4, platelets 214,000, Na 138
with K 4.1, BS 148, creatinine 0.57. MRI 04/20-Lg cystic
enhancing L frontal mass w/lg amount of surrounding edema
& mass effect. Sub falcine herniation is seen on the order of
1.4. 04/20-MRI without contrast: Impression: Left frontal lobe
intra-axial/parenchymal mass. Mass somewhat poorly
defined without IV contrast. Sub falcine herniation is seen
with extensive white matter edema.
Cerebral Edema:
Progress Note
ED: Left frontal brain mass. H/P: Brain tumor, large left frontal as described,
possible surgical intervention later. CVA-post stroke hemiplegia affecting
right side. Breast CA, s/p right lumpectomy May 2009. HTN.
Hypothyroidism. Hyperparathyroidism. Renal insufficiency. OA. GERD.
Urinary incontinence. Morbid obesity. Asthma.
PROGRESS NOTES: 04/20: brain tumor, left frontal enhancing mass. 04/22:
Solitary brain met. likely breast CA recurr. 04/22-post op MRI shows
excellent decompression of cystic lesion, some mild enhancement around
resection cavity and blood products in cavity, questionable residua, some
mild residual midline shift and effacement of ventricle.
CONSULTS: 04/20: Left frontal cystic brain tumor this am after post-gad
stealth MRI completed. Guarded prognosis. 04/20: Marked peri-
lesional vasogenic edema throughout left frontal lobe.
Marked cingulate herniation with left-to-right shift. Mass
displaces the corpus callosum inferiorly. Edema extends
back to the posterior frontal lobe. Right hemiparesis, dysphasia
secondary to left frontal brain tumor, likely breast metastasis, less likely
glioblastoma multiforme. 04/20-Most likely brain metastases from original
tumor although primary glioma cannot be excluded.
Cerebral Edema:
Operative Report
Treatment
• IV Decadron started prior to admission on 04/14 –
continued during stay.
• Craniotomy with excision/destruction of lesion/tissue
brain on 04/20/2011. Postop dx: Left frontal cystic brain
tumor. Body of op note: "MRI showed a large cystic
anterior left frontal lesion with diffuse left hemispheric
vasogenic edema and marked mass effect with
cingulate herniation. Lesion over 4.5 cm x 3 cm x 3 cm
with over 1/2 of cystic lesion comprised of enhancing
cellular mass. Moderate amount of cystic fluid, think
xanthochromic looking-Floseal and Surgicel were used
for hemostasis in the tumor bed and reapplied. Duragen
placed over craniotomy defect as onlay graft.”
Intracerebral Hemorrhage With
Vasogenic Edema
From Coding Clinic, 1Q 2010, p. 8
Question: A patient is admitted and diagnosed
with intracerebral hemorrhage (ICH). The
provider also documented "vasogenic edema."
Is it appropriate to code the vasogenic edema?
Answer: Assign code 431, Intracerebral
hemorrhage, as the principal diagnosis. Assign
code 348.5, Cerebral edema, as an additional
diagnosis. It is appropriate to code the cerebral
edema separately since it is not inherent in
cerebral hemorrhage.
Glioblastoma With Vasogenic Edema
From Coding Clinic, 3Q 2009, p. 8
Question: The patient is a 48-year-old male with glioblastoma
multiforme status post two surgeries. The tumor has recurred with
massive growth since debulking one month ago. The provider
indicated that there was a significant amount of surrounding vasogenic
edema and mass effect. Is it appropriate to assign a code for cerebral
edema when it is due to a primary intracranial process such as a brain
tumor and the provider has indicated that it is clinically significant?
•Answer: Assign code 348.5, Cerebral edema, as an additional
diagnosis, since the provider has evaluated and documented the
clinical significance of the vasogenic edema.
•Patients with glioblastoma commonly develop vasogenic edema.
Vasogenic edema is an accumulation of fluid in the brain (due to the
tumor’s disruption of the blood-brain barrier). The surrounding edema
can increase the mass effect of the tumor and is considered an
irreversible process. Tumor-related vasogenic edema may disrupt
synaptic transmission and alter neuronal excitability, leading to
headaches, seizures, focal neurological deficits, and encephalopathy.
The condition can contribute to morbidity, resulting in fatal brain
herniation.
Transbronchial Lung Biopsy
Transbronchial Biopsy
Pathology Reports:
Transbronchial Lung Biopsy
IV fluids, IV Protonix. IV Rocephin. IV cardizem. Serial
cardiac enzymes, hold nortriptyline due to
anticholinergic side effect. Poor candidate for AAA.
Two bronchoscopies were done. First one had too much
bleeding then subsequent transbronchial biopsy on
04/26 documented in operative note as "bleeding is from
the left upper lobe and the left lingula and from right
upper lobe. Transbronchial biopsy obtained of the right
upper lobe along with microbiological brushing and
cytological brushing."
Also noted on path report 04/26: Lung, right upper lobe
transbronchial biopsy. Benign bronchial and lung tissue
with minimal chronic inflammation."
Transbronchial Biopsy of Lung
From Coding Clinic, 1Q 2011, p. 18
Question: The procedure is listed as bronchoscopy due to
nodular infiltrates and atelectasis and airway
examination. Washings, brushing and biopsy were taken
from the left lower lobe and washings from the right
lower lobe. Additionally, the provider has clarified that a
transbronchial biopsy of the left lower lobe was
performed. However, lung tissue was not identified on
the pathology report. Should a transbronchial biopsy of
the lung be reported?
Answer: Based on the provider’s documentation, assign
code 33.27, Closed endoscopic biopsy of lung, for the
transbronchial biopsy. The absence of lung tissue in the
pathology report does not preclude the assignment of
the code when the procedure is performed by the
provider. Tissue samples may be inadequate or
inconclusive.
Transbronchial Lung Biopsy vs.
Endoscopic Bronchus Biopsy Clarification
From Coding Clinic, 2Q 2009, pp. 16–17
Question: In Coding Clinic, Third Quarter 2004, p.
9, there was a question on how to code
transbronchial biopsy and also how to code
fiberoptic bronchoscopy and brushings and
biopsies when the pathology report describes
tissue from the bronchus as well as lung tissue.
The answer advised code 33.24, Closed
[endoscopic] biopsy of bronchus, for biopsy of
the bronchus and code 33.27, Closed
endoscopic biopsy of lung, for biopsy of the
lung. Was code 33.27 assigned based on the
pathology report or was it assigned to assist in
coding "transbronchial" biopsy?
Transbronchial Lung Biopsy vs.
Endoscopic Bronchus Biopsy Clarification
From Coding Clinic, 2Q 2009, pp. 16–17
Answer: Most bronchoscopic biopsies should be coded 33.24, as that
encompasses flexible fiberoptic as well as rigid bronchoscopy. It also
includes washings (for obtaining cells for diagnostic cytopathology),
brushings, and forceps biopsies.
•Transbronchoscopic fine needle aspiration/biopsy (Wang needle
aspiration biopsy) is also captured with code 33.24. Small bits of lung
tissue are seen from time to time on these biopsies, and they should
not be coded as transbronchoscopic lung biopsies, unless that was the
intent of the procedure.
•Code 33.27 (closed endoscopic biopsy of lung) is specific for
transbronchoscopic lung biopsy, and the inclusion terms mention the
use of fluoroscopic guidance or control and that would reflect the
increased resources needed for the procedure. From an historical
point of view, the intent of this code was to differentiate flexible
fiberoptic bronchoscopic lung biopsy from that done with the rigid
bronchoscope. Actual lung specimens obtained either way are
sometimes insufficient for diagnosis, and with the advancements in
VATS lung biopsy and the accompanying ability to get more adequate
tissue samples in a safe manner, bronchoscopic lung biopsy to
diagnose diffuse lung disease is done less often than in the past.
Cultures:
A/H1N1 Influenza
HPI: 81-year-old male who comes in complaining of 4–5 days of
coughing with white sputum, some shortness of breath, very
tired with diarrhea, now tachycardic. VS: T 37.0, HR 123, BP
107/43, RR 18, O2 sats 2L nasal cannula. PMH: DM, HTN.
DIAGNOSTICS: WBC 4.1, hemoglobin 15.4, creatinine 1.56
down to 1.07 on discharge, glucose of 311, Na 135, K 4.4,
CO2 of 20, lactic acid 2.0. CXR: no active cardiopulm process
disease. EKG: tachycardia. 2nd CXR: negative for PNA.
03/03 positive for H1N1 influenza A virus novel
H1N1 by direct fluorescent antibody stain.
H/P: Acute renal failure. Tachycardia likely due to dehydration.
Viral illness – possible influenza. May have touch of PNA.
DM. HTN.
PROGRESS NOTES: 03/02: tachycardia improving. Acute
kidney injury. Acute bronchitis likely viral syndrome. Hx of
DM.
Cultures:
Organism on Sputum
• Positive sputum culture for MRSA
• Positive sputum culture for Pseudomonas
– Possible clarification opportunity – is physician
treating pneumonia caused by organism
(MRSA) or due to (MRSA), or is the culture a
contaminant, or does patient have
colonization?
Clarification Opportunities for Other
Documentation of Clinical Significance
• BMI clinical significance
• Dietary consults
– Malnutrition (degree and treatment)
• Wound consults
– Stage of pressure ulcer
– Apligraf®
Nursing Documentation:
BMI Clinical Significance
• Patient is 68-year-old female with pneumonia
who is significantly overweight with BMI of 52
requiring “big boy” bed, minimum of two person
assist to move as well as extra-large wheelchair.
Increased difficulty breathing due to morbid
obesity.
Body Mass Index Reporting Clarification
From Coding Clinic, 2Q 2010, p. 15
Question: There has been some confusion as to whether nursing staff
documentation is acceptable for assigning the body mass index (BMI).
Since hospitals are allowed to code the BMI based on the dietitian’s
documentation, it would seem reasonable to assign the BMI based on
the nurse’s documentation as well. Can coders use nursing
documentation to assign the BMI?
Answer: Yes, the BMI may be assigned based on medical
record documentation from clinicians, including nurses and
dietitians who are not the patient’s provider. As stated in the
Official Guidelines for Coding and Reporting, BMI code assignment
may be based on medical record documentation from clinicians who
are not the patient’s provider, since this information is typically
documented by other clinicians involved in the care of the patient.
Dietitians were only mentioned as an example of a clinician that might
document BMI information.
• However, the associated diagnosis (such as overweight, obesity, or
underweight) must be documented by the provider. Refer to the Official
Guidelines for Coding and Reporting for additional discussion.
Malnutrition – Guidelines
From Coding Clinic, 4Q 1992, pp. 24–25
Malnutrition Codes
• Malnutrition is generally thought of as a problem associated with
children. Increasingly, it is becoming a problem for the elderly of this
country who are unable to properly care for themselves, and who do
not have the resources to obtain daily care.
• Category 262, other severe protein-calorie malnutrition, and category
263, other and unspecified protein-calorie malnutrition, contain
inclusion statements that define malnutrition in terms of weight for age,
which is a standard method for classifying childhood malnutrition.
• Effective October 1, 1992, all the inclusion statements from the
malnutrition codes have been deleted. With this change, it is hoped
that coders will no longer feel restricted in the use of these codes and
use these codes for all age groups, not just children, as the original
inclusion statement implied.
• In order to improve the reporting of malnutrition among the elderly, it is
important for physicians to document the condition in the medical
record and for coders to be aware of malnutrition as a potential
diagnosis.
Dietary Consults:
Malnutrition
• Degree & treatment
• Where to look:
– Dietary consults
– Labs: Albumin and prealbumin levels
presented
– Provider clinical picture documentation and/or
orders
Early Recognition of Protein
Malnutrition
Early recognition of protein malnutrition and initiation of
nutritional therapy can shorten the length of hospital stays and
improve patient outcomes.
•Prealbumin is the earliest laboratory indicator of nutritional
status and has emerged as the preferred marker for malnutrition
because it correlates with patient outcomes in a wide variety of
clinical conditions.
•One study noted that as many as 50% of hospitalized patients
were at risk for protein calorie malnutrition. Patient care was
improved by incorporating the prealbumin level into the
nutritional assessment, which enabled caregivers to begin
supplementation before the patient's condition deteriorated.
– Mears E. Outcomes of continuous process improvement of a nutritional care program incorporating
serum prealbumin measurements. Nutrition. 1996;12:479–84.
Prealbumin Levels – Risk of
Malnutrition
• Determining the level of prealbumin, a hepatic protein, is
a sensitive and cost-effective method of assessing the
severity of illness resulting from malnutrition in patients
who are critically ill or have a chronic disease.
• Prealbumin levels have been shown to correlate with
patient outcomes and are an accurate predictor of
patient recovery.
• In high-risk patients, prealbumin levels determined twice
weekly during hospitalization can alert the physician to
declining nutritional status, improve patient outcome,
and shorten hospitalization in an increasingly costconscious economy.
Prealbumin – Most Accurate
Predictor
Levels and risk of malnutrition
Prealbumin risk level
Prognosis
• <5.0 mg per dL (< 50 mg per L) Poor prognosis
• 5.0 to 10.9 mg per dL
Significant risk;
• (50 to 109 per L)
aggressive nutritional
support indicated
• 11.0 to 15.0 mg per dL Increased risk;
monitor status
biweekly
• 15.0 to 35.0 mg per dL Normal
Protein Calorie Malnutrition
Table
Measurement
Normal
Mild
undernutrition
Moderate
undernutrition
Severe
malnutrition
Normal weight
90–110
85–90
75–85
<75
Body mass index
19–24
18–18.9
16–17.9
<16
Serum albumin
3.5–5.0
3.1–3.4
2.4–3.0
<2.4
Serum transferrin 220–400
201–219
150–200
<150
Total lymph count 2000–3500
1501–1999
800–1500
<800
Delayed
hypersensitivity
2
1
0
2
Wound Consults:
Look for Apligraf®
Possible missed opportunity = 86.67
• Look in wound consult note for application of
Apligraf
– Used for diabetic non-healing wounds/ulcers,
venous stasis ulcers, and burns
• Application methods:
– Suturing
– Gluing
– Steri-Strips
– Followed by compression dressings
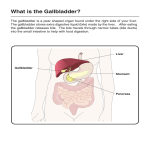
What Is Apligraf?
Apligraf is applied as a bi-layered living skin substitute.
• FDA has approved Apligraf (Graftskin) for use with diabetic
foot ulcer care in the treatment of diabetic foot ulcers of
greater than 3 weeks' duration. This expands the use of
Apligraf, which received marketing clearance in 1998 for use
in the treatment of venous leg ulcers of greater than 1
month's duration that have not adequately responded to
conventional therapy alone.
• In a large-scale clinical trial Apligraf was shown to heal more
diabetic foot ulcers faster than conventional therapy alone. By
12 weeks of treatment, 63 (56%) of 112 patients with diabetic
foot ulcers treated with Apligraf were 100% closed, compared
with 36 (39%) of 96 patients with ulcers treated with
conventional therapy alone (debridement, saline dressing,
and total off-loading).
Apligraf® Wound Repair System
From Coding Clinic, 3Q 2010, p. 7
Question: The patient has a nonhealing ulcer of the medial left
calf. She is currently on a wound VAC but has history of
fasciotomy and arterial thrombectomy of the area. Apligraf®
was placed at bedside. What is the code assignment for the
procedure?
Answer:
• Assign code 86.67, Dermal regenerative graft, for placement
of the Apligraf® wound repair system.
• Apligraf® is a biological skin therapy used in the treatment of
persistent nonhealing sores. It delivers living cells, rebuilding
proteins and growth factors similar to the human skin, on an
ongoing basis when there is the potential to form a sore due
to disrupted healing in patients with diabetes and poor
circulation. It is placed directly on the wound, which is then
covered with a nonadhesive dressing.
Questions?
In order to receive your continuing education certificate for
this program, you must complete the online evaluation which
can be found in the continuing education section at the front
of the workbook.