Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
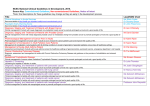
Frameworks foR undeRstaNDing ThE cancer population H McConnell, R White, J Maher. Macmillan Cancer Support Background We are particularly interested in the ‘intermediate survival’ group. We believe that hospital activity data2, along with clinical insight, suggests that this group more often experiences ongoing complex clinical care needs such as relapse or recurrence. It also suggests that they can face an especially uncertain future.1 This group may require a balance of acute intervention, self management and chronic illness management. This compares to the need for a focus on the impact of recovery and late effects for the longer-term survival cancers or a focus on early diagnosis and good treatment or palliative care for the ‘shorter-term survival’ cancers. Figure 1 Proportion of people in each of the three cancer groups, estimates for the UK New diagnoses in 2013 (% of incidence) People living with cancer up to 20 years post diagnosis in 2010 (% of prevalence) Deaths due to cancer in 2013 (% of mortality) Longerterm survival cancer types Intermediate survival cancer types Shorterterm survival cancer types 137,000 (39%) 1,172,000 (65%) 33,000 (20%) 73,000 (21%) 343,000 (19%) 28,000 (17%) 95,000 (27%) 165,000 (9%) 72,000 (45%) Note: Numbers do not add up to 100% as we have excluded leukaemia, head and neck cancer, ill-defined and some rarer cancers in the categories as the highly diverse cancer pathways makes them difficult to stratify. These excluded cancers made up 13% of incidence, 7% of prevalence and 18% of mortality. We next focus on everyone living with a specific cancer type. For the most commonly diagnosed cancers, we present the number of people in each phase of their cancer journey (figure 2).3 For example, we estimate that more than 30,000 men living with prostate cancer may need care for progressive disease as well an additional 11,000 men approaching end of life in the UK in 2010. People in each of the phases, and with different cancers, are likely to have distinct needs. This means different interventions may be required to support them. Acknowledgements Routes from Diagnosis was developed by Macmillan Cancer Support in partnership with Monitor Deloitte and the National Cancer Intelligence Network (NCIN) operated by Public Health England. We acknowledge the use of data for this analysis collected by cancer registries across the United Kingdom. References 1.McConnell H, White R, Maher J. Three cancer groups to explain the different complexity, intensity and longevity of broad clinical needs. NCRI conference poster session presented at NCRI Cancer Conference. 1–4 November 2015. Liverpool. 2.New unpublished Macmillan analysis from the Routes from Diagnosis research programme, undertaken by Monitor Deloitte for Macmillan Cancer Support. See also Macmillan Cancer Support. Routes from Diagnosis. The most detailed map of cancer survivorship yet. 2014. 3.Yip K, et al. Using routinely collected data to stratify prostate cancer patients into phases of care in the UK: implications for resource allocation and cancer survivorship. Br J Cancer. 2015. 112(9): 1594-602. 4.Macmillan Cancer Support. Routes from Diagnosis. The most detailed map of cancer survivorship yet. 2014. 5.Maddams J, et al. Projections of cancer prevalence in the United Kingdom, 2010–2040. Br J Cancer. 2012. 107(7): 1195–1202. For more information please contact [email protected] November 2015 End of life 16,000 (11,000 year1) End of life 11,000 (2,000 year1) End of life12,000 (2,000 year1) Progressive care 23,000 Progressive care 32,000 Progressive care 24,000 End of life 35,000 (29,000 year1) Ongoing monitoring (10+ years) 21,000 Progressive care (not estimated) Ongoing monitoring (10+ years) 73,000 Ongoing monitoring (5≥10 years) 51,000 Ongoing monitoring (5≥10 years) 6,000 Initial monitoring (2–5 years) 9,000 Recovery & readjustment (1–2 years) 13,000 Initial monitoring (2–5 years) 48,000 Ongoing monitoring (10+ years) 29,000 Ongoing monitoring (5≥10 years) 62,000 Ongoing monitoring (10+ years) 235,000 Ongoing monitoring (5≥10 years) 127,000 Initial monitoring (2–5 years) 63,000 Active surveillance (2+ years) 9,000 Active surveillance (0–2 years) 7,000 Initial monitoring (2–5 years) 103,000 Watch & wait (0–2 years) 18,000 Recovery & readjustment (1–2 years) 31,000 Recovery & readjustment (1–2 years) 27,000 Diagnosis & treatment (0–1 years) 50,000 Diagnosis & treatment (0–1 years) 43,000 Figure 1 shows the estimated sizes of the three cancer groups. The majority of people living with cancer have a cancer type in the ‘longer-term survival’ cancer group, but significant minorities of people have cancer types in the ‘shorterterm survival’ and the ‘intermediate survival’ groups (around 10% and 20% respectively). The different groups are helpful to present a broad focus for service design which should be considered in their management. Diagnosis & treatment (0–1 years) 42,000 We present different views of the cancer population. Firstly, in framing all cancers, we present three ‘cancer groups’ using survival rates for different cancer types. We use this alongside evidence about the likely complexity, intensity and longevity of needs for the majority of people in each group.1 Colorectal Results Lung Available data on prevalence, incidence, mortality and survival of the UK’s cancer population is reviewed alongside the wider evidence base on needs and experiences. These include patient experience surveys, pathways of care, key policy and strategies to inform the development of our cancer population frameworks. Prostate Methods Diagnosis & treatment (0–1 years) 29,000 We present different ways to frame the cancer population which can facilitate practical application of this knowledge for different purposes and audiences. Breast Cancer incidence, mortality, survival and, more recently, prevalence have been used as high-level proxies of the scale of need to support the development and monitoring of cancer services. This data is limited in its ability to reflect the complexity in disease pathways. Recovery & readjustment (1–2 years) 47,000 Figure 2 Cancer care pathway – estimating the number of people in the United Kingdom by cancer type 2010 For example, the recovery package should be implemented as outlined in the Cancer Strategy. This should happen from diagnosis and treatment so as to plan ongoing care and facilitate recovery and readjustment as appropriate. For many women with breast cancer in the post-treatment monitoring phase, a tailored focus on early identification of potential consequences of cancer and its treatment and management of cancer, alongside other conditions is key. This is rather than the current outpatient follow-up models. Early identification of tumours and wellmanaged palliative and end of life care is particularly key for the majority of people with lung cancer. complications or other inpatient morbidities, also build up some of the highest costs (groups 2, 3 and 6). The pathways also present key ‘transition’ points between phases of care and the number of people who may experience these in a year. Critically, these transitions – for example from treatment to recovery – need to be well managed between sectors of care and health professionals. That way, we can ensure patient care and experience is not compromised. The insight offered by Routes from Diagnosis is already being used to improve cancer services in the UK, for example in South Yorkshire, Bassetlaw and North Derbyshire Clinical Commissioning Groups. In these places, the framework has been used to more deeply understand the ‘footprint’ of care in the local area and inform the redesign of the colorectal cancer care pathway. Finally, we present an example of detailed survivorship outcomes, or ‘Routes from Diagnosis’, mapping the cancer journey from diagnosis to death or continued survival for a cohort of people diagnosed with a specific cancer. We use survival, recurrence, metastases, second cancers, and inpatient morbidities and care to categorise people into different clinically relevant outcomes groups.4 Conclusions Figure 3 presents one example from the work for prostate cancer and demonstrates the wide range of outcomes within cancer types, even within survival groups. Only a quarter of people survive long term (seven plus years survival) with no metastases and no other inpatient morbidities with relatively low cost (group 8). Approximately 11% survive long term and develop metastases or have cancer complications incurring much higher costs per patient (group 6). Routes from Diagnosis provides the cancer community with a scientific, evidencebased framework. This can be applied to cancer care commissioning, service and system design, and policy formulation, and to inform the direction of academic research. Clinical teams and commissioners, who understand the variations in clinical journeys, can target improvements to ensure people living with cancer receive the right tailored care, at the right time, in the right place. We know that the number of people living with cancer will increase to four million by 2030.5 It is critical that key decision-makers in health, social care and government – and cancer care teams – understand the range of needs of the cancer population. This will ensure that they are able to develop services and support for the whole of people’s cancer journeys. We have used these different frameworks in a variety of ways. We have used them to quantify some of the needs, support the Cancer Strategy and the National Cancer Survivorship Initiative, and to inform the redesign of patient care pathways. We have found that different ways of presenting the cancer population are needed in line with the end use of the framework. Further work in this area continues, for example quantifying more precisely the time at which patients start and finish all treatments. We are also looking to more accurately calculate the number of people requiring support for specific long-term effects, recurrent cancer or metastatic disease. The highest inpatient costs are associated with moderate survival (group 2) as opposed to longer-term survival groups. Groups who experience cancer Figure 3 Detailed Routes from Diagnosis survivorship outcome framework and average post-diagnosis inpatient costs for prostate cancer, men diagnosed in 2004 in England Survival time 0–12 months Survivorship outcome Metastases No Metastases Metastases presented 1–7 years survival Metastases developed Percentage of prostate cancer patients High inpatient care 2% Low inpatient care 2% High inpatient care 2.2% Cancer complications Single other inpatient morbidity Multiple other inpatient morbidities Group 2 £12,000 Group 3 £2,700 Group 4 £11,500 Group 6 £7,500 Group 7 £3,000 Group 8 1.2% 3.1% 0.7% 6.7% Single other inpatient morbidity 1.2% Multiple other inpatient morbidities 4.7% Metastases 6.3% 1.4% 9.5% Cancer complications 3.3% Circulatory only 1% MSK only 1.8% Genitourinary only Single other inpatient morbidity 1.8% 2 other inpatient morbidities 2+ other inpatient morbidities No other inpatient morbidities Notes: Cancer complications = recurrence or additional primary cancer; High inpatient care = patient spent more than 25% of survival length in hospital; Low inpatient care = patient spent less than 25% of survival length in hospital. Macmillan Cancer Support, registered charity in England and Wales (261017), Scotland (SC039907) and the Isle of Man (604). MAC15794_FRAMEWORKS £14,200 6.9% No other inpatient morbidities No Metastases Group 1 1.7% Cancer complications 7+ years survival £6,700 6.2% Low inpatient care No other inpatient morbidities No Metastases Average cost per patient (£) 6.1% 4.8% 25.3% MSK: musculoskeletal. Average post-diagnosis inpatient costs exclude patients with no inpatient records. Group 5 is not applicable to the prostate cancer simplified survivorship outcomes framework.