Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
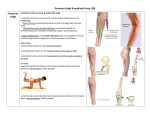
Lower Extremity blocks Lumbar Plexus • The lumbar plexus consists of five nerves on each side, the first of which emerges between the first and second lumbar vertebra and the last one between the last lumbar vertebra and the base of the sacrum. • The major branches of the lumbar plexus are the genitofemoral, lateral femoral cutaneous, femoral, and obturator nerves. • The femoral nerve is formed by the posterior divisions of L2-4 and descends from the plexus lateral to the psoas muscle. Genitofemoral nerve block • The genitofemoral nerve is mainly a sensory nerve, and it is formed from the first and second lumbar nerves • The nerve descends on the surface of the psoas major muscle behind the ureter, and divides into the genital and femoral branches at a variable distance above the inguinal ligament. • The genital branch enters the inguinal canal through the deep inguinal ring and passes through the inguinal canal (man) or round ligament of the uterus (woman). • The femoral branch accompanies the external iliac artery and below the inguinal ligament remains enveloped by the femoral vascular sheath lateral to the femoral artery. 1. Pubic Tubercle 2. Inguinal Ligament 3. Anterior Superior Iliac Spine 4. Obturator Nerve 5. Accessory Obturator Nerve 6. Superior Ramus of the Pubic Bone 7. Genitofemoral Nerve 8. Femoral Nerve 9. Sciatic Nerve Technique • Patient in supine position. • The main anatomical landmarks are identified: the pubic tubercle, inguinal ligament, inguinal crease and femoral artery. • The femoral branch of the genitofemoral nerve is blocked by inserting the 25G/5-cm needle at the lateral border of the femoral artery at the inguinal crease. • A fanlike infiltration of the subcutaneous tissue is made in a medial, caudal and cephalad direction with 10-15 ml of local anesthetic solution. • The genital branch of the genitofemoral nerve is blocked by infiltration of 10 ml of local anesthetic just lateral to the pubic tubercle, below the inguinal ligament. Anatomic landmarks Landmarks for the posterior approach to sciatic blockade are easily identified in most patients. Proper palpation technique is of utmost importance because the adipose tissue over the gluteal area may obscure these bony prominences. The landmarks are outlined by a marking pen: • Greater trochanter • Posterior-superior iliac spine • Needle insertion point 4-cm distal to the midpoint between landmarks 1 and 2 Popliteal Block • Indications: Ankle and foot surgery • Landmarks: Popliteal fossa crease, tendons of the semitendinosus and semimembranosus muscles Popliteal Block Popliteal Block Popliteal Block Popliteal Block Popliteal Block Popliteal Block Popliteal Block Popliteal Block Popliteal Block Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Popliteal Block: Lateral Approach Saphenous Nerve Block Saphenous Nerve Block Saphenous Nerve Block Ankle Block • Indications: Surgery on foot and toes • Nerves: • Two deep nerves: Posterior tibial, deep peroneal • Three superficial nerves: superficial peroneal, sural, saphenous Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block Ankle Block