Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
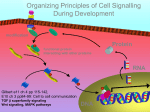
ISCs regulatory signalling and cancer pathways The pathways controlling the ISC are slowly being unravelled and, if these cells prove to be the origin of “tumour propagating cells”, should provide us with targets at which future cancer treatments can be aimed. The proper cell fate decisions of the ISC progeny as they migrate, proliferate and differentiate on route to assuming their appropriate positions within the villus are organised within the mircoanatomy of the crypt structure. These are tightly controlled processes with cells migrating at different rates. In the small intestine the upward migrating enteroendocrine cells migrate at the same rate as the surrounding cells turning over every approximately four days [30, 31], however in the large intestine they migrate independently over 23 days as opposed to the 4 days of the surrounding cells [73]. Indeed it is the short life span of these cells that negates the effects of any post differentiated mutations they may have acquired [74]. Any perturbation of the pathways regulating the ISCs and its daughter cells proliferation, differentiation or migration that allows accumulation and retention of cells within the intestinal epithelium would be prerequisite to neoplastic transformation. Further, although there is little evidence, account must also be taken of signals from the cells that surround the crypt such as the enteric neuron [75], as it is likely they also mediate different cell fates along the vertical crypt axis. Genetic experiments have shown that many regulatory signals are involved in the crypt-villus patterning, including the bone morphogenetic (BMP), Notch, PtdIns(3,4,5) kinase, Sonic Hedgehog (in the developing mouse[76]) and Wnt pathways [77, 78, 79, 80]. Wnt signalling Wnt signalling is critical for both the development of the intestine and the homeostasis of the adult tissue [81, 82, 83, 84]. However it is the deregulation of this pathway in CRC that has lead to its extensive study in the intestine [85, 83], [86]. As a mutation in the Apc gene (usually resulting in a protein truncation [87]), a single component of the canonical Wnt pathway, is associated with 85% of sporadic intestinal neoplasia and almost all inherited CRCs namely familial adenomatous polyposis (FAP). Inactivation of Apc is the earliest known genetic event in CRC [88]. The Wnt pathway (from Drosophila Wg (wingless) and Int gene [89]) starts with a large family of 19 secreted molecules called Wnts which bind to at least 10 members of its receptor families Frizzled (Fz) and low-density lipoprotein receptorrelated protein family LRP5/6. The binding of Wnts to the Fz receptor permits an interaction and phosphorylation of a cytoplasmic molecule called dishevelled (Dsh). Dsh then disrupts the so call “-catenin destruction complex”, -catenin is a signalling molecule which if allowed to accumulate in the cytoplasm will subsequently translocate to the nucleus where it activates members of the TCF/LEF family of transcription factors [90, 91, 92]. Intracellular levels of -catenin is regulated via formation of a multiprotein “destruction complex” encompassing glycogen synthase kinase β (GSK3β), casein kinase 1 (CK1), and the scaffolding proteins Apc, Axin1 and Axin2. This multiprotein complex of molecules phosphorylates specific serines and threonines within -catenin, triggering ubiquitination by TrCP and degradation in proteasomes. Consequently the presence of Wnt ligands or any disruption of the destruction complex allows β-catenin to accumulate and translocate to the nucleus. Once Wnt signalling has been activated there is alteration in the expression pattern of its TCF/LEF target genes (for a list of known Wnt target genes see www.stanford.edu/~rnusse/). A gradient of Wnt signalling along the crypt-villus axis controls expression of the EphB/ephrinB sorting receptors and ligands. This gradient of receptors allows the correct positioning of intestinal epithelial cells indeed EphB receptor activity suppresses CRC [93, 94]. It is these findings and the presence of nuclear β-catenin at the base of the crypt, adjacent to the presumptive stem cell niche, that has suggested a critical role for Wnt signalling in intestinal homeostasis and stem cell maintenance [95]. Deregulating the Wnt pathway by removing the Apc gene alters the stemness, proliferation and differentiation of the ISCs in the adult murine intestine. As Wnt activation immediately imposes disruption of the tissue architecture and the formation of benign growths, a phenotype mimicking tumourigenesis [95]. Further demonstrated by the evidence that this phenotype is entirely dependent on the Wnt target gene C-Myc [96]. Murine intestine cells that lose Apc undergo rapid entry into S-phase, enhanced apoptosis, failed migration and perturbed differentiation [95]. For these benign growths or adenomas to progress towards carcinoma other Wnt promoting factors are involved, such as oncogenic activation of the KRAS oncogene [97], autocrine Wnt feedback loops [98] and paracrine modulation of epithelial Wnt signalling by the myofibroblasts and other stromal cells [99]. The Wnts can also stimulate cellular responses through the so called “non-canonical” Wnt pathway. These are β-catenin independent and involve calcium trafficking or induce morphogenic changes via the planar cell polarity pathway. In summary the loss of Apc, activating the Wnt pathway, immediately confers virtually all of the phenotypes associated with the very early stages of intestinal neoplasia but deficiency of either C-Myc [100] or β-catenin [101] leads to loss of the mutant tumour propagating cells and replacement by wild type crypts in murine models. Targeting this pathway in CRC may give effective control of CRC and its metastases. For example mice which are heterozygous for a mutation in Apc develop multiple intestinal neoplasia (MIN) [102] (as in human FAP patients) which is attenuated by loss of the methyl binding domain proteins Mbd2 and kaiso [103, 104]. Mice null for these genes show an associated reduction in expression of Wnt target genes upon Wnt activation. ISC therapeutics How we approach the development of ISC therapeutics depends where we intervene in an intestinal tumours’ development. In a sporadic occurrence if it is detected at a late stage (which could be avoided with adequate screening of susceptible patients) we may need to debulk the tumour (which current drugs are able to do) and target the tumour propagating cells to prevent its recurrence. To target the propagating cells in this situation we would need knowledge of the pathways the cells have utilised to drive their transformation. In hereditary predispositions such as FAP with 100% penetrance of tumours we could predict the pathway involved but it would be beneficial for treatments to prevent the initiation of the polyps that will lead to cancer. When approaching the problem there is an initial decision to be made whether we want the ISC therapeutic agent to prevent tumour initiation or to remove tumours that have developed. Either way it is likely the same signalling pathways, namely Wnt, in the ISCs will be targeted. Preventing tumour initiation The earliest known genetic event in CRC is the inactivation of Apc leading to aberrant expression of Wnt target genes FAP these tumours are benign but eventually lead to cancer later in life. The inactivation of the remaining Apc results in nuclear βcatenin aberrantly activating Wnt target genes to drive the ISC to over proliferate and form a polyp. A process crucial to this is the hypermethylation of gene promoters which results in their silencing. In mice it is known that inhibition of DNA methylation through reduction of DNA methyltransferase 1 (DNMT1) [129, 130] or perturbation of a protein that interprets the DNA methylation signal e.g. Mbd2, suppresses intestinal tumourigenesis in ApcMin mice [104]. We can assume hypomethylation and gene promoter hypermethyaltion are events that silence or over express gene essential for initial neoplastic transformation of a cell. Large scale alterations in DNA methylation, with global hypomethylation and promoter specific hypermethylation linked to aberrant patterns of histone modification are common in cancer cells [131, 132] with estimates suggesting that the average tumour will contain approximately 100–400 hypermethylated promoter regions. Demethylating and histone deacetylase (HDAC) inhibiting drugs (e.g. zebularine, RG108, trichostatin A, green tea extract EGCG, hydroxamic acids, benzamides & cyclic tetrapeptides) are showing promising results in cancer where specific hypermethylation is implicated in the etiology [133]. Some of these drugs are in phase I or II trials and are proving to be effective in certain cancers with newer molecules showing less toxicity. However which genes are initially epimutated as to allow neoplastic transformation in the ISC and which are secondary effects are unknown [134, 135]. One major concern about epigenetic drugs is their general lack of target specificity as global demethylation can potentially activate oncogenes [136, 137]. To maximize efficiency of epigenetic drugs, their mechanisms and targets must be more clearly defined. Results in mice with proteins such as Mbd2 which interpret the methylation signal but still reduce intestinal tumour burden may provide us with specific genes for therapeutic targeting. Which specific gene(s) are being derepressed via Mbd2 loss that prevent tumourigenesis has yet to be defined. These genes are of interest as the loss of Mbd2 combined with specific removal of Apc in the intestine doesn’t suppress Wnt signalling but does reduce its elevation. Another reason Mbd2 may be an attractive therapeutic target is the possibility that it may allow therapeutics with less cytotoxic effects. If as in mice humans can tolerate Mbd2 loss without harmful effects. The caveats to this are that the effects of such therapeutics are transient and the aberrant epigenetic patterns are likely to return once the treatment period terminates. However they are quite promising chemopreventive agents in cases when epimutations increase the risk of developing a disease in individuals who do not yet show signs of malignancy. The results of the long term exposure to such agent may be their undoing in a preventative measure but they may still be effective post tumour initiation in preventing recurrence after tumour removal. We are at the dawn of epigenetic medications but further progress is required, in particular, in the development of compounds with higher specificity and greater efficacy to see if they fulfil their potential. Preventing tumour recurrence As removal and debulking of CRC is already feasible it is the recurrence of these tumours which represent the main challenges for ISC therapeutics in sporadic patients. Assuming that within a metastasising tumour there are cells resistant to cytotoxic therapy with the potential to regenerate the tumour in situ and ex situ. As the pathways these cells have utilised to allow neoplastic transformation is likely to differ from tumour to tumour then initially we would assume all pathways have to be targeted. However as most other pathways all converge with Wnt signalling at some stage this would be the likely first target. There are many molecules identified which will down regulate Wnt signalling [138]. These molecules work at all levels of the canonical Wnt pathway. From the top of the pathway the natural inhibitors of Wnt such as the FRPs or Dickkopf gene family which is commonly down regulated in gastrointestinal tumours and can inhibit invasion in vitro [139, 140] and adult mice intestinal proliferation in vivo [81]. Through to genes involved in stabilising the βcatenin destruction complex, down regulating β-catenin, targeting the nuclear βcatenin with molecules such as ICAT and TBLR1[141] which inhibit the βcatenin/TCF4 interaction and finally targeting the Wnt target genes themselves such as C-myc. Many of these targets have been attacked by different mechanism in vitro and in vivo. By repairing the defective components of the β-catenin destruction complex through introducing wild type versions [142, 143], over-expressing βcatenin/TCF inhibitors [144], antisense degradation of β-catenin [145], introduction of β-catenin binding proteins that target for degradation [146, 147, 148] and screens highlighting molecules to disrupt the β-catenin/TCF4 interaction [149, 150] have all been show to inhibit tumour growth and survival. Therapeutic specificity for the cancer ISC For any ISC therapy it is critical that the normal somatic stem population is not catastrophically impaired. The therapeutic agent ideally shall be tumour specific to avoid side effects as for example the Wnt pathway is also is also a therapeutic target for neurodegenerative, bone and cardiovascular disease [151]. Targeting of single pathways will probably not be sufficient due to systemic toxicity limitations. Therapeutic targeting of signalling synergy between Wnt and other important pathways in the cancer stem cell may provide the angle for controlling CRC. In vitro studies using tyrosine kinase inhibitors, and combinations of agents against the EGF and Wnt pathways all show potential for inhibiting CRCs [152, 153]. Targeting the cross talk between the regulatory pathways and mesenchyme in the ISC niche may also provide the therapeutics to specifically target the cancer cells rather than normal cells. BMP targeting may be attractive due to findings that BMP signalling in the stroma results in Wnt suppression. Aside from the previously described pathways there are other potential targets for drugs against colorectal cancer. The paracrine hormone hypothesis of colorectal cancer (described by [154]) implicates the dysregulation of the guanyl cyclase C (GCC) and its paracrine ligands. Deletion of GCC causes an increase in the mutation rate and, presumably from the ISC, defective lineage specific differentiation, increases the size of the proliferating cell compartment, the number of proliferating cells in that compartment and their cell cycle kinetics [155, 156]. This loss of the paracrine hormones is associated with overexpression of the receptors in tumours as compared to normal cells in human intestine [157] however it is unknown if they mark the stem cells so its use in preventing recurrence is unknown until the cancer stem cell is identified. The requirement for tumour cell specific therapeutics is due to the concern over destruction of the normal ISC population. This may be less of a concern once we have characterised the ISC and is proposed quiescent versions. These are the stem cell described earlier which allow repopulation of the crypt-villus following destruction of the active ISC. If it exists it is the quiescent stem cell in whatever shape or form it comes which may allow therapies targeting all active ISC to be successful. The location of this quiescent stem cell is of great interest, as potentially in a process called transdifferentiation a cell can extricate it self from foreign tissues, transform and migrate to contribute to adult stem cells within other tissues. This process is of great interest, indeed adult bone marrow cells can contribute to adult cell lineages in several non-haematopoietic tissues, including the gastro-intestinal tract. Further evidence is needed to show if potentially bone marrow cells can form ISCs [158, 159], or even a mesenchymal stem cell in the lamina propria which could then rise to an ISC. If possible all ISC could be eliminated therapeutically safe in the knowledge that the organ will be replenished from the protected undamaged quiescent stem cells. Summary To summarise for the past half century, oncologists have had systemic drugs available that are able to induce tumour responses in patients with colorectal cancer. However, in cases of advanced colorectal cancer, these regimens are almost never curative. The recently introduced concept that cancer stem cells drive tumour growth suggests a reason for these therapeutic failures. Current chemotherapeutics target rapidly dividing cells not their controlling pathways missing the slow dividing cytotoxic resistant cancer SCs. The failure also suggests a solution the development of therapeutics that target cancer SCs. If we can identify the ISC and characterise the differences in its tumour propagating counterpart we can exploit their differences. We will then be able to treat sporadic tumours with current drugs, essential to debulk the tumours and with the tumour propagating cell agent to prevent their recurrence. In the last 20 years extensive information about the mechanisms by which SC populations are maintained has been obtained without actually identifying the ISC. Although we have still to identify the ISC we may have identified how they are controlled as has been described earlier there are many pathways and molecules which are capable of altering the homeostasis of the intestine. Much of the work described here has yielded markers for cells showing characteristics of being the ISC. We are getting nearer the goal of identifying the active, quiescent and potential ISCs which lead to CSCs. The current proposed markers have yet to be categorically proven but until definitive identification of the ISC they are being used to study the effects of DNA damaging agents and chemotherapeutic agents in vivo on these potential ISC. The value for CRC therapeutics using the targets proposed by the ISC regulatory pathways and the various methods of attacking them (e.g. anti-sense, RNA interference and protein knockdown strategies [160]) can only be assessed when the proposed CSC have been identified. At that juncture we will finally be able to assess the roles of the ISC in drug discovery.