Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
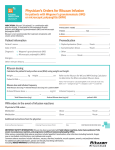
1. ALLERGIES/REACTIONS: 2. Height: 3. INDICATION AND DOSE: cm Weight: kg Relapse or refractory, low grade or follicular, CD20 positive, B-Cell NHL RITUXIMAB (RITUXAN) 375 mg/m2 or ( mg/ m2) times Frequency: Chronic Lymphocytic Leukemia RITUXIMAB (RITUXAN) 375 mg/m2 times THEN 500 mg/ m2 times Frequency: Every 28 days BSA = BSA = m2 BSA BSA = mg mg for Cycle 1, mg for Cycles 2-6 Refractory immune (idiopathic) thrombocytopenia purpura RITUXIMAB (RITUXAN) 375 mg/m2 or ( mg/ m2) times Frequency: BSA = mg Wegener’s Granulomatosis RITUXIMAB (RITUXAN) 375 mg/m2 or ( Frequency: Weekly times 4 doses mg/ m2) times BSA = mg Microscopic Polyangiitis RITUXIMAB (RITUXAN) 375 mg/m2 or ( Frequency: Weekly times 4 doses mg/ m2) times BSA = mg Rheumatoid Arthritis RITUXIMAB (RITUXAN) 1 g IV on days 1 and 15 4. PRE INFUSION LABS: CBC CMP LDH Uric Acid (URIC) Phosphate (PHOS) Hepatitis Panel (acute and chronic) 5. 6. 12 HOURS PRE RITUXIMAB (RITUXAN): Start Allopurinol 300 mg PO daily – consider when treating malignancies Hold blood pressure medications 12 hours prior to Rituximab Hydration IV: 30 MINUTES PRE RITUXIMAB (RITUXAN) GIVE: Acetaminophen (Tylenol) 650 mg PO. May repeat every 4 hours PRN chills or temperature greater than 38 C. Diphenhydramine (Benadryl) 50 mg PO. May repeat every 4 hours PRN chills or temperature greater than 38 C. Methylprednisolone (Solu-Medrol) 100 mg IV prior to dose on Days 1 and 15 for Rheumatoid Arthritis only Methylprednisolone (Solu-Medrol) 40 mg IV times 1 dose for Chronic Lymphocytic Leukemia (CLL) and lymphocytes greater than 25 K/mcL Methylprednisolone (Solu-Medrol) 40 mg IV times 1 dose Dexamethasone (Decadron) 10 mg IV times 1 dose. LIMIT THE TOTAL DOSE OF ALL ACETAMINOPHEN CONTAINING PRODUCTS TO 3,000 MG PER DAY Physician Initial: PATIENT INFORMATION Page 1 of 2 (05/09/12) 615 Revision I PHYSICIAN ORDERS RITUXIMAB (RITUXAN) INFUSION 7. RITUXIMAB (RITUXAN) ADMINISTRATION (CONCENTRATION = 1 MG/ML): DO NOT ADMINISTER AS AN INTRAVENOUS PUSH OR BOLUS First Infusion: (Required for initial dose OR patients with Chronic Lymphocytic Leukemia (CLL) and lymphocytes greater than 25 K/mcL only) Mix 100 mg of total dose in 0.9% sodium chloride (Normal Saline) 100 ml and infuse at initial rate Initial rate = 50 mg/hour (50 ml/hour) times 30 minutes. Then increase rate 50 mg/hour (50 ml/hour) every 30 minutes to a maximum of 400 mg/hour (400 ml/hour). If patient tolerates medication with no infusion reaction, call Pharmacy and request remainder of dose Subsequent Infusions: Initial rate = 100 mg/hour (100 ml/hour) times 30 minutes. Then may increase rate 100 mg/hour (100 ml/hour) every 30 minutes to a maximum of 400 mg/hour (400 ml/hour). DO NOT INFUSE OTHER MEDICATIONS INTO THE IV LINE WITH RITUXIMAB (RITUXAN) 8. VITAL SIGNS: Check pre-infusion, every 30 minutes during, and 30 minutes post infusion Call physician if: Systolic blood pressure less than mmHg, Pulse greater than Temperature greater than C 9. Nurse May Initiate CVAD Management Per Nursing Protocol #910.00 Nurse May Utilize Local Anesthetic For CVAD Access Per Nursing Procedure #788 Nurse May initiate IV Catheter Care, Outpatient Physician Order #858 For Infusion Reactions Initiate Drug Related Hypersensitivity Physician Order #774 If mild infusion reaction occurs the infusion may be resumed at one-half the previous rate upon improvement of patient symptoms 10. OUTPATIENTS: If stable 30 minutes post-infusion, discharge patient home on current reconciled home medications NOTE: These orders should be reviewed by the attending physician, appropriately modified for the individual patient, dated, timed and signed below. DATE TIME PHYSICIAN’S SIGNATURE Another brand of drug, identical in form and content, may be dispensed unless checked. PATIENT INFORMATION Page 2 of 2 (05/09/12) 615 Revision I PHYSICIAN ORDERS RITUXIMAB (RITUXAN) INFUSION