Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
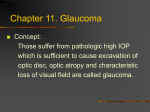
SURVEY OF OPHTHALMOLOGY VOLUME 58 NUMBER 1 JANUARY–FEBRUARY 2013 MAJOR REVIEW Glaucoma and Uveitis Sana S. Siddique, MD,1,2 Ana M. Suelves, MD,1,2 Ujwala Baheti, MD,1,2 and C. Stephen Foster, MD, FACS, FACR1,2 1 Massachusetts Eye Research and Surgery Institution; and 2Ocular Immunology and Uveitis Foundation, Cambridge, Massachusetts, USA Abstract. Despite its relative rarity, uveitis is the third leading cause of preventable blindness worldwide. Glaucoma associated with uveitis is one of the most serious complications of intraocular inflammation. We review in detail the epidemiology and pathogenesis of uveitic glaucoma and the safety and efficacy of the current medical and surgical treatment modalities. (Surv Ophthalmol 58:1--10, 2013. Ó 2013 Elsevier Inc. All rights reserved.) Key words. drainage implants glaucoma trabeculectomy I. Introduction trabectome uveitis developing glaucoma not only because of the uveitis, but also as a side effect of the use of corticosteroids, the mainstay of uveitis treatment. The association between uveitis and glaucoma was first reported by Joseph Beer in 1813 as arthritic iritis followed by glaucoma and blindness. In 1891 Priesley Smith proposed the first modern classification of uveitic glaucoma (UG). Specific types of UG were described by Fuchs in 1906 (heterochromic uveitis) and Posner and Schlossman in 1948 (glaucomatocyclitic crisis).B UG is one of the most serious complications of intraocular inflammation. Approximately 20% of uveitis patients in the United States develop glaucoma. There is no race, sex, or age predilection.B,56 Glaucoma is much more common in chronic uveitis, an incidence of 11% after 5 years, than acute uveitis, with 7.6% after 12 months.33,58 Some authors report no differences in the incidence of UG between anterior and posterior forms,58 but a study in 927 patients established anterior uveitis as the main cause, which is consistent with the overall distribution of uveitis.12 The occurrence of In the United States uveitis has an estimated prevalence of about 38 cases, and an incidence of 15 cases, per 100,000 population.27 One estimate is that uveitis afflicts 109,000 people in the United States and that 43,000 new cases a year are diagnosed.82 Over 2 million people worldwide are thought to have uveitis. Despite significant advances in therapeutics, the prevalence of blindness secondary to uveitis has not been reduced in the past 30 years. In the largest population-based study in the United States, the incidence of uveitis was approximately 3 times that of previous estimates and increased with the increasing age of patients. Women had a higher prevalence of uveitis than men, and the largest differences were in older age groups.30 Unless interventions improve, about 10% of patients with uveitis will be blinded by it. Epidemiological studies in the United States suggest that this underestimates the risk by as much as 4- to 5-fold. The sight-threatening complications of uveitis include damage to the retina and glaucoma. Patients with uveitis have an increased risk of 1 Ó 2013 by Elsevier Inc. All rights reserved. 0039-6257/$ - see front matter http://dx.doi.org/10.1016/j.survophthal.2012.04.006 2 Surv Ophthalmol 58 (1) January--February 2013 secondary glaucoma depends on the type of uveitis, being more common in Fuchs heterochromic uveitis, Posner-Schlossman syndrome, uveitis associated with herpes infection, and juvenile idiopathic arthritis (JIA)—ranging in frequency from 5--46% in patients with JIA.26,32,43,54,59,69 Additionally, glaucoma is more frequent in uveitic eyes of corticosteroid non-responders than in corticosteroid responders.68 II. Pathogenesis of Glaucoma Associated with Uveitis The mechanisms by which uveitis leads to elevated intraocular pressure (IOP) are incompletely understood. Imbalance between aqueous production and resistance to aqueous outflow from inflammation may result in a subsequent change in IOP. During episodes of intraocular inflammation, IOP is often reduced because of aqueous humor hyposecretion secondary to ciliary body inflammation, coupled with increased uveoscleral outflow. Over time, multiple mechanisms can conspire to increase the resistance to aqueous outflow during episodes of uveitis, thereby leading to elevated IOP. In some cases a rise of IOP in the presence of intraocular inflammation is a diagnostic challenge. The differential is between insufficient anti-inflammatory therapy with persistence of active inflammation, steroid response, and chronic structural damage secondary to inflammation. Glaucoma may be open or closed-angle. Openangle glaucoma represents the more common form of UG. Typically, increased resistance occurs as a result of mechanical obstruction of the trabecular meshwork, which may be blocked by inflammatory cells, proteins, debris, or fibrin liberated from a disrupted blood-aqueous barrier, inflammatory precipitates on the meshwork, and swelling or dysfunction of the trabecular lamellae or endothelium, resulting in increased resistance to the aqueous outflow.56 Additionally, mediators such as Rho kinases may cause a constriction of trabecular endothelium, increasing the outflow resistance.66 Increased levels of protein in the aqueous are a result of increased permeability of the blood-aqueous barrier, which leads to an aqueous that more closely resembles serum. This elevated protein content may lead to IOP elevation. Cytokines released by inflammatory cells further exacerbate inflammation and may stimulate neovascularization in the angle. Some prostaglandins demonstrated in the aqueous humor of eyes with uveitis are also known to cause elevated IOP. In chronic cases of uveitis, obstruction of aqueous outflow may result from scarring and obliteration of trabecular SIDDIQUE ET AL meshwork beams or Schlemm’s canal or from overgrowth of a fibrovascular membrane in the angle. Additionally, the treatment of uveitis with corticosteroids results in elevated IOP in up to one-third of patients.9 Although corticosteroids have proven to be effective in reducing inflammation, prolonged administration can result in elevated IOP by decreasing aqueous outflow. Secondary ocular hypertension from corticosteroid administration is dependent on the dose, the chemical structure of the corticosteroid compound, the frequency and route of delivery, the duration of treatment, and the patient’s susceptibility to steroid response (‘‘steroid responders’’). Clinically, a corticosteroid response usually develops 2 to 6 weeks after initiating therapy, but may occur at any time. It is often difficult to distinguish between the side effects of the corticosteroids and the underlying inflammation. Only about 5% of the normal population demonstrates corticosteroid responsiveness,14 but with impaired conventional outflow seen during intraocular inflammation, the corticosteroid response rate rises significantly. The risk factors of being a steroid responder are primary open-angle glaucoma, familial history of glaucoma, rheumatoid arthritis, extremes of age (children and the elderly), and diabetes. Children are especially susceptible to an IOP increase secondary to steroids.5,80,90 Corticosteroids have been reported to cause biochemical and morphological changes in the trabecular meshwork, increasing resistance to aqueous outflow, and several theories have been proposed to explain this phenomenon, including accumulation of glycosaminoglycans in the trabecular meshwork, inhibition of phagocytosis by trabecular endothelial cells, and inhibition of synthesis of certain prostaglandins.B,C Ultrastructural analysis of trabeculectomy specimens in quiescent uveitic eyes with glaucoma show an increase of total extracellular material in the trabecular meshwork and a loss of inner wall endothelial cells, without an increased accumulation of inflammatory cells as compared to primary open-angle glaucoma specimens.76 Secondary angle-closure glaucoma can also result from a number of mechanisms in uveitic eyes. Angle closure with pupillary block occurs when anterior chamber inflammation results in 360 of posterior synechiae (Fig. 1), blocking the flow of aqueous from the posterior chamber into the anterior chamber, resulting in iris bombé. Peripheral anterior synechiae, another common complication of intraocular inflammation (Fig. 2), are typically broad-based and can result in total closure of the angle. Less commonly, nonpupillary block angleclosure glaucoma develops when inflammation and edema cause the ciliary body to rotate forward, 3 GLAUCOMA AND UVEITIS evaluating the angle.59 Retinal OCT requires a clear cornea, but anterior segment OCT does not. Objective evaluation of the optic nerve and nerve fiber layer may be done through OCT and Heidelberg retinal tomography. It is useful to obtain baseline photographs of the optic nerve. IV. Uveitic Disorders Associated with Glaucoma Many different types of uveitis have been associated with glaucoma, but certain disorders may have a relatively higher risk. Fig. 1. Posterior synechiae involving most of the pupillary margin. closing the angle,C a mechanism described in patients with Vogt-Koyanagi-Harada syndrome.47 III. Signs and Symptoms The patient may present with blurred vision, ocular pain, brow ache, redness, and other ocular disturbances. Some patients with markedly elevated IOP often have severe eye pain and nausea associated with corneal edema. Topical glycerol may decrease corneal edema so that the ophthalmologist may adequately assess the eye. Patients may also complain of photophobia and colored halos. Examination should include evaluation of the optic nerve and visual field to assess glaucomatous damage, along with gonioscopy to detect the presence of peripheral anterior synechiae and to assess the angle. If the cornea cannot be adequately cleared, ultrasound biomicroscopy and optical coherence tomography (OCT) are useful tools for Fig. 2. Anterior synechiae adjacent to the temporal limbus and Ahmed valve tube visible superiorly. A. FUCHS HETEROCHROMIC UVEITIS Fuchs heterochromic uveitis (FHU) was described by Ernst Fuchs in 1906 as a triad of anterior uveitis, heterochromia, and cataract. It is typically unilateral, affecting the hypochromic eye; in 13% of the cases it presents bilaterally. In some series FHU represents 2-5% of total uveitis cases and around 15% of anterior uveitis. It is believed to be underdiagnosed, especially in bilateral cases in which heterochromia is not well seen. The typical age of onset is 20--40 years of age, with men and women affected equally.46 FHU is a rare, idiopathic, chronic, low-grade iridocyclitis, without synechiae, with heterochromia, low-grade anterior chamber reaction with diffuse, small stellate keratic precipitates, posterior subcapsular cataract, and secondary open-angle glaucoma. An association between FHU and rubella virus has been described.10,64 The uveitis is typically poorly responsive to corticosteroid therapy, and in fact steroids may worsen the IOP elevation. Treatment of the glaucoma is initiated with medical therapy. The reported incidence of glaucoma in FHU varies from 13--59%, with higher figures seen on long-term follow-up. Glaucoma is believed to be the major long-term threat to vision in FHU patients. Typically, glaucoma more commonly develops in persons of African descent and in bilateral cases.1 Glaucoma generally persists after uveitis has subsided and does not respond to steroids. Controlling inflammation has little or no effect on IOP, and many physicians do not treat the associated inflammation. Medications, particularly aqueous suppressants, may be effective in controlling glaucoma initially, but characteristically FHU-associated glaucoma is relatively resistant to medical therapy, and surgery is often necessary.35,50 Treatment of the inflammation with corticosteroids may do little more than accelerate cataract formation and increase IOP further. Glaucoma is the major threat to vision in patients with FHU, and though frequently intermittent and well controlled initially, it may 4 Surv Ophthalmol 58 (1) January--February 2013 become chronic and difficult to treat. Unless glaucoma develops, FHU is a benign disorder and does not require therapy. B. POSNER-SCHLOSSMAN SYNDROME Posner-Schlossman syndrome, also known as glaucomatocyclitic crisis, was first described in 1948. It presents between 20 and 60 years of age, typically with unilateral recurrent episodes of mild cyclitis and heterochromia. Though inflammatory signs may be minimal, rise of intraocular pressure may be in the range of 40--70 mm Hg during an acute attack, but this usually resolves spontaneously. The levels of prostaglandins in the aqueous humor are correlated with the level of IOP.37 The prognosis for patients with Posner-Schlossman syndrome is benign, except when they develop glaucomatous damage, which occurs in about 25% of cases. Raitta and Vannas believed that there may be a relationship between this syndrome and the eventual development of primary open-angle glaucoma.65 Although the pathogenesis of PosnerSchlossman syndrome remains unknown, suggested possible associations include an immunogenetic factor involving HLA-Bw54,35 viral infections (Herpes simplex and cytomegalovirus),11,89 gastrointestinal disease, and various allergic conditions including angioneurotic edema, eczema, urticaria, contact dermatitis, asthma, rhinitis, food allergies, and intolerance to aspirin.48 A vascular cause has been postulated based on the demonstration of segmental iris ischemia on fluorescein angiography. Vasculature incompetence could be associated with a release of prostaglandins, inflammation, and a subsequent rise in intraocular pressure.52 Prostaglandin inhibitors, oral indomethacin, and subconjunctival polyphloretin (a prostaglandin antagonist) have been shown to lower intraocular pressures during attacks, further supporting this theory.37,52 The prognosis for control of IOP in patients with glaucomatocyclitic crisis is good.39 Chandler and Grant recommended corticosteroid therapy to control inflammation and topical hypotensive medications, including beta-blockers and carbonic anhydrase inhibitors, to control pressure during acute attacks.2 Currently, the favored initial treatment is a topical nonsteroidal anti-inflammatory drug (NSAID) to control the inflammation (diclofenac 0.1% 1 gutta three or four times daily).39 Topical steroids (prednisolone acetate 1% 1 gutta three times daily, followed by taper), oral NSAIDs (indomethacin 75--150 mg/day), or carbonic anhydrase inhibitors (acetazolamide 250 mg by mouth three times daily) may also be used. Antiprostaglandin therapy may play a role in the future. SIDDIQUE ET AL C. JUVENILE IDIOPATHIC ARTHRITIS The prevalence of glaucoma in JIA-associated uveitis has been reported in the range of 14--27%43,45,86 our group,26 however, found a higher prevalence: 42% of patients with JIA-uveitis had associated glaucoma or ocular hypertension. Patients who experience persistent low-grade intraocular inflammation are at greatest risk for developing glaucoma, and an earlier referral to a glaucoma specialist and an aggressive approach to treatment of UG may reduce the risk of blindness in this population. The glaucoma associated with JIA commonly occurs with open angles, but may be of the pupillary block, secondary angle-closure type, as a result of the formation of posterior synechiae. We acknowledge the difficulty of treating glaucoma associated with JIA-uveitis and have outlined our approach.26 We treat our patients with a stepladder algorithm beginning with topical steroids and cycloplegics, possibly followed by regional injection steroid therapy and brief systemic steroid therapy. If inflammation recurs with steroid withdrawal, an oral NSAID is used. Immunomodulatory therapy, usually methotrexate, is the final step in our algorithm, with resulting high efficacy and low toxicity. Biologic response modifier therapy has been reserved for treatment failures. Medical treatment of glaucoma is initiated with a step-by-step approach starting with topical beta blocker and sympathomimetics, adding topical carbonic anhydrase inhibitors (oral if necessary) and latanoprost if required. We believe that it is beneficial to consider filtering surgery (mitomycin C [MMC] trabeculectomy with or without fluorouracil [5-FU] and draining devices) early on if pressures remain uncontrolled. Some consider goniotomy as the first-line surgical intervention for childhood glaucoma.28,36 Freedman and associates28 conducted a retrospective review of patients with refractory glaucoma associated with chronic childhood uveitis to evaluate the safety and efficacy of goniotomy in these patients. They evaluated 12 patients with childhood UG and found a high overall success rate of 75% with a mean follow-up of 32.4 months. Similarly, Ho and colleagues36 conducted a study of the long-term results of standard goniotomy in childhood glaucoma and reported success in 72% of eyes (55% without medications) with a mean follow-up of more than 8 years. Compared with other surgical options, goniotomy offers comparable or even higher rates of success, but with fewer risks of complications such as infection, exacerbation of uveitis, iatrogenic damage to intraocular structures, or hypotony. Thus, goniosurgery is considered an effective, low-risk surgical intervention that can be utilized in the face of failure with maximal medical therapy. 5 GLAUCOMA AND UVEITIS D. HERPETIC UVEITIS The association between virus infections of the anterior uvea and glaucoma was described more than 40 years ago.75 Secondary glaucoma is the most common complication in patients with herpetic uveitis.55 An estimated 28--45% of patients with Herpes simplex virus (HSV) keratouveitis (Figs. 3, 4) develop transient elevated IOP,44 and 10%44 to 54%55 may present with secondary glaucoma.55 An acute increase in IOP in the presence of active iridocyclitis is the hallmark of a herpetic etiology, associated most commonly with either HSV or varicella zoster virus (VZV).55 These hypertensive episodes are attributed to inflammation of the trabecular meshwork,22 similar to PosnerSchlossman crises. This is supported by the normalization of IOP in response to topical corticosteroids. Additionally, the increase of IOP can be secondary to swelling and obstruction of trabecular meshwork by inflammatory cells and debris. Typically, herpetic iridocyclitis episodes are unilateral, synechiaeforming, and explosive in nature; with hypopyon, hyphema, or fibrin deposition noted at exam in severe cases.31,49 Diffuse or sectorial iris atrophy demonstrated by retroillumination at the slit lamp is no longer considered pathognomonic of VZV, but it is a characteristic of herpetic iritis, including HSV, VZV, or cytomegalovirus iridocyclitis. Management of secondary glaucoma in patients with herpetic uveitis may be difficult. In severe cases long-term anti-glaucoma therapy and surgical approach may be warranted even after the active inflammation has subsided. Along with management of glaucoma, long-term antiviral prophylaxis such as oral acyclovir, valacyclovir, or famciclovir is usually required to prevent recurrences.77,81 We normally prescribe acyclovir 800 mg twice a day or valacyclovir Fig. 4. Large patches of iris atrophy in a patient with HSV-related uveitis. Note the transillumination defects and the visualization of the haptic inferiorly. prophylactically for patients with herpes simplex disease and double the dose for varicella zoster disease. Topical antiviral therapy is indicated in patients with keratouveitis to prevent viral replication during the use of topical steroid treatment, but it is considered ineffective in herpetic uveitis. V. Management Treatment of glaucoma in uveitis depends on the underlying disease. One should treat any underlying systemic disease, the ocular inflammation, and the glaucoma. The ocular inflammation and glaucoma usually can be controlled with anti-glaucoma and anti-inflammatory agents. Often, treatment of the inflammation will control the IOP. Patients treated aggressively with anti-inflammatory therapy have a better clinical course of uveitic glaucoma. We use potent topical corticosteroids such as difluprednate or betamethasone.25 Invasive options are considered if glaucoma medical management does not suffice, which occurs in 25--30% of cases. A. MEDICAL Fig. 3. Slit-lamp photograph of a 23-year-old man with HSV-related transillumination defects and iris atrophy spreading from 9 o’clock to 5 o’clock. Traditionally, the first-line agents used to treat increased IOP associated with uveitis were topical beta-blockers and carbonic-anhydrase inhibitors. Absorption of topical medication may be decreased in the face of inflammation, and systemic carbonic anhydrase inhibitors should be considered if topical medications fail to have the desired effect. Oral or intravenous hyperosmotic agents may also be used. Prostaglandin analogs are now the first-line drugs, and, although they have been reported to reinduce or cause exacerbations of inflammation,23,70,71,84,85 they may be used in patients in whom the uveitis is 6 Surv Ophthalmol 58 (1) January--February 2013 quiescent. Our group followed 42 patients (59 eyes) with anterior, intermediate, or posterior uveitis treated with the prostaglandin bimatoprost and concluded that bimatoprost is an effective and safe agent in lowering IOP in patients with uveitic glaucoma where the uveitis is controlled on immunomodulatory therapy. Other studies support the efficacy and safety of other prostaglandin analogs as IOP-lowering agents in UG, even in herpetic keratouveitis.51,68 Additionally, prostamides do not increase the flares of uveitis,24 nor do they result in clinically significant cystoid macular edema.17 Typically we start with a topical prostaglandin such as bimatoprost, latanoprost, or travoprost once a day. If this alone fails to control the IOP, we add another topical agent such as a beta-blocker (timolol) up to twice a day, carbonic anhydrase inhibitor (dorzolamide or brinzolamide) up to two to three times per day, or an alpha agonist such as brimonidine up to twice a day. If maximal topical therapy fails to control the IOP, we add an oral carbonic anhydrase inhibitor such as acetazolamide 250--1,000 mg per day. If all medical efforts fail, we move along to other options such as selective laser trabeculoplasty (SLT) which, in our experience,63,A works well in patients with UG. If further intervention is needed, we use the Ahmed valve or MMC trabeculectomy. SIDDIQUE ET AL in the range of 14--40%.18,19,40 In a recent review on SLT in patients with non-uveitic glaucoma, it was concluded, based on five prospective and two retrospective studies comparing SLT with ALT, that the IOP lowering efficacy of SLT is similar to ALT with statistically equivalent mean IOP reductions.67 SLT, in comparison to ALT, induces less inflammation and does not alter the structural integrity of the trabecular meshwork (TM), an important consideration in UG, where permanent structural alterations can contribute to glaucoma.8,56 SLT has been effective in controlling IOP in patients with UG and we use it as the next step after maximal medical therapy fails. We recently conducted a retrospective analysis of 84 eyes of 84 patients with UG who underwent selective laser trabeculoplasty. The patients were divided based on the presence or absence of prior glaucoma surgery (trabeculoplasty/ valve), and outcomes were analyzed at 1, 3, 6, and 12 months. SLT was successful in reducing mean IOP percentage in naı̈ve eyes from baseline at 1, 3, 6, and 12 months by 15.2%, 16.8%, 23.3%, and 19.8%, respectively (all statistically significant levels). SLT was less effective in eyes with previous glaucoma surgery, though 50% of the eyes at all follow-up visits had a pressure decrease of $ 1 mm Hg. There was no statistically significant difference between numbers of flare-ups prior to SLT compared with flareups during follow-up.63,A B. SURGICAL If medical management fails to get the IOP under control, the next step is to use surgical options, including laser therapy, trabeculectomy, drainage implants, and cycloablation. The severity of uveitis may increase after surgical intervention. 1. Laser Iridotomy Pupillary-block glaucoma may occur from posterior synechiae formation or a fibrin membrane. A laser iridotomy with an argon and/or Nd:YAG laser may relieve the block. Sometimes more than one iridotomy may be required. In some cases, a surgical iridectomy may be required if the laser iridotomy seals secondary to intense inflammation.13,70 This is especially likely in patients with brown irides. Argon laser trabeculoplasty (ALT) usually fails to control the IOP in uveitic eyes because of angle alterations, and we do not advocate ALT in patients with UG. SLT is done with a 532-nm Q-switched Nd:YAG laser that specifically targets pigmented cells in the trabecular meshwork, using low power and ultra-short durations, and spares the adjacent cells from collateral thermal damage and preserves structural integrity. Various studies have reported a mean reduction of IOP at various follow-up times 2. Trabeculectomy Trabeculectomy is indicated for eyes with closedangle, open-angle, or combined mechanism glaucoma when IOP is believed to be too high despite maximum tolerated medical and laser therapy. The results of unaugmented trabeculectomy are variable and are particularly poor in young patients with UG,73 as a result of an accelerated wound-healing response. Anterior idiopathic uveitis, Fuchs cyclitis, and aphakia have traditionally been associated with a higher risk of surgical failure. Combined surgery with phacoemulsification has a high risk of surgical failure in patients with intermediate uveitis.15 Hoskins and associates38 reported successful control of IOP (! 21 mm Hg) in six of their nine patients with uveitis who underwent trabeculectomy. Stavrou and colleagues74 achieved an overall 1- and - year success rates of 92% and 83%, respectively, in 33 eyes treated with trabeculectomy for UG. Hill and associates34 reported successful trabeculectomy in 13 (81%) of 16 patients with uveitic glaucoma after 1 year and in 11 (73%) patients after 2 years. They also reported that in five of seven patients with significant postoperative inflammation, the filtering surgery failed. 7 GLAUCOMA AND UVEITIS Trabeculectomy with wound healing modulators, such as 5-FU and MMC, has been used in an effort to minimize scarring of the filtration bleb in patients with UG and to improve the success rate in patients with a high risk of failure.5,62,87,88 MMC can be applied to the eye for a variable duration prior to or after dissection of the scleral flap; irrigation of the subconjunctival tissues should be carried out to prevent intraocular exposure, however. Towler and associates79 reported on 28 uveitic eyes undergoing trabeculectomy with and without 5-FU. In 17 eyes trabeculectomy was followed by subconjunctival 5-FU beginning on the day after surgery. Ten 200-ml injections of 5 mg 5-FU in sterile saline were given into the lower fornix daily for 7 days, then on alternate days for the next 7 days. Eleven eyes underwent unaugmented trabeculectomy. During the first 2 years more than 90% of the 5-FU group achieved control of the IOP compared with 80% of the non 5-FU patients. Complete surgical success was defined as IOP # 20 mm Hg without topical anti-glaucoma drops and partial success was defined as IOP # 20 mm Hg with topical anti-glaucoma therapy. The success of IOP control was analyzed by combining the two groups. The median survival of primary trabeculectomy in the 5-FU--treated eyes was 60 months, compared with 42 months for untreated eyes. After 5 years only 50% of the eyes that underwent trabeculectomy with 5-FU were controlled and only 30% of the eyes that did not receive 5-FU were controlled. This same group reported a larger series with a success rate of 67% after 5 years in eyes with UG treated with trabeculectomy plus intraoperative 5-FU.78 Similarly, Patitsas and colleagues61 reported a 71% success rate in eyes undergoing trabeculectomy with 5-FU after a mean follow-up of 34 months. Ceballos and colleagues16 reported a cumulative probability of success of 78% and 62% with trabeculectomy with 5-FU or MMC at 1 and 2 years, respectively. They also reported male sex as the only statistically significant risk factor for trabeculectomy failure. A more recent study by Kaburaki41 demonstrated no differences in rate of IOP control after 5 years in 53 eyes with inactive uveitis and secondary glaucoma compared with 80 eyes with primary open-angle glaucoma that underwent a trabeculectomy plus MMC. This study showed similar incidence of postoperative complications, but hypotonic maculopathy was more frequent in UG. Even though subconjunctival bevacizumab has been used successfully in controlling wound healing after glaucoma filtration surgery, there is no published data evaluating the safety and efficacy of intraoperative use of bevacizumab as adjunct to trabeculectomy in UG. 3. Non-penetrating Glaucoma Surgery Non-penetrating glaucoma surgery (NPGS) is a large trabeculectomy with the final thin layer of Descemet’s membrane left intact. The aqueous fluid percolates through the membrane into a ‘‘lake’’ in a pocket of the sclera. The fluid is absorbed into blood vessels, rather than getting to the subconjunctival space to be absorbed there. There are two variations of NPGS: viscocanalostomy and nonpenetrating deep sclerectomy (NPDS). Both involve removal of a deep scleral flap, the external wall of Schlemm’s canal and corneal stroma behind the anterior trabeculum and Descemet’s membrane, thus creating an intrascleral space. The aqueous humor leaves the anterior chamber through the intact trabeculo-Descemet’s membrane into the scleral space, hence it will egress into different pathways. The risk of IOP being too low is lessened because there is no complete hole through the wall of the eye. The best patients for NPGS are those in whom an IOP of 17--18 mm Hg would be adequate. An implant is normally used in deep sclerectomy, but no routine antiproliferative agents are used, and the IOPs are not as low as those seen with trabeculectomy. Several small, prospective, randomized trials have been conducted to compare the efficacy and sideeffect profile of NPDS with that of trabeculectomy.4 Although these had limited follow-up, they did generally demonstrate that postoperative IOP reduction was equivalent or slightly lower compared with that of trabeculectomy, but with a lower frequency of complications. Some retrospective reviews of NPGS found NPDS to be significantly safer than trabeculectomy while retaining good IOP control.21,53 NPDS with implant, and intraoperative MMC, has also been used in UG with a high success rate,3,7,72 but the series are small, retrospective, and non-comparative. So far, no cases of endophthalmitis have been reported following NPDS, even when augmented with intraoperative antimetabolites, and this is likely to be related to the barrier provided by the trabeculo-Descemet’s membrane. There is currently no evidence in the form of adequately powered randomized trials with sufficiently long follow-up periods to conclusively demonstrate that NPGS has a significantly lower risk of endophthalmitis and infection when compared to trabeculectomy and glaucoma drainage device implantation, however. Regardless of the surgical procedure, it is of utmost importance to educate the patient about the symptoms of bleb-related infection to allow early intervention.4 NPGS has been used in patients with UG, but no long-term data have yet been published on its safety and efficacy. 8 Surv Ophthalmol 58 (1) January--February 2013 4. Glaucoma Drainage Device Implantation Drainage implants are designed to route aqueous from the anterior chamber to a posterior reservoir. They are particularly useful in cases with significant conjunctival scarring due to previous surgery. Drainage valves, such as the Ahmed valve (Fig. 2), may be safer than trabeculectomy with less risk of hypotony. They have been used with increasing frequency in the management of UG, either as the initial glaucoma surgery or when trabeculectomy has failed, and have proved to be an effective tool. We have found a cumulative probability of success of up to 94% at one year, following (between 1995 and 1998) 19 patients (21 eyes) with chronic uveitis who underwent Ahmed glaucoma valve implantation for uncontrolled glaucoma.20 Gil-Carrasco and associates29 reported successful glaucoma management after Ahmed glaucoma valve implantation in 8 of 14 uveitic eyes (57%) after an average follow-up of 14 months. Hill and colleagues34 included 11 patients with uveitic glaucoma with failed trabeculectomy filtering blebs who subsequently received Molteno drainage implants. Safety and efficacy of the Ahmed valve has also been demonstrated in children.42,57 We recently published the long-term results of Ahmed glaucoma valve implantation in uveitic glaucoma, with success rates of 77% and 50% at 1 and 4 years, respectively.60 Ceballos and colleagues,16 using the Baerveldt glaucoma drainage implant in 24 eyes, had a success rate of 92% at 1 year, with most patients requiring no adjunctive medical therapy. A retrospective comparative study in refractory UG eyes versus primary open-angle glaucoma disclosed no significant differences in IOP control or long-term complications, except for an increased need of removing the tube observed in uveitic eyes.60 5. Stents No data on the use of stents in UG have been published. 6. Cycloablation As a last resort, cycloablative techniques can be used to decrease aqueous production by destruction of the ciliary body using transcleral or intraocular diode Nd:YAG laser cyclophotocoagulation. An 810nm infrared diode laser may also be used. Unfortunately, cycloablative procedures often exacerbate inflammation and lead to postoperative hypotony and phthisis bulbi. Therefore, cycloablation is only used as a last resort for refractory glaucoma in eyes with poor visual potential in which conventional drainage surgery has failed.6,83 SIDDIQUE ET AL VI. Conclusion Uveitic glaucoma is potentially blinding and should be managed aggressively. In the minority of patients who fail medical management, trabeculectomy with antifibrotic agents or drainage implants must be used. Maximum control of the inflammation by topical, regional, and/or oral steroids or other immunomodulatory therapy is critical for a favorable long-term visual outcome. VII. Method of Literature Search Literature selection for this review was based on a Medline database search from the period 1955 to 2011, using the following key words and various combinations: uveitis and glaucoma. VIII. Disclosure The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. References 1. Allingham RR, Damji K, Freedman S, et al. Steroid induced glaucoma, in Allingham RR, Damji K, Freedman S, et al (eds). Shields Textbook of Glaucoma. Baltimore, MD, Lippincott Williams and Wilkins; ed 5, 2005, pp 387--92 2. Allingham RR. Glaucoma due to intraocular inflammation, in Epstein DL, Schuman JS (eds). Chandler and Grant’s glaucoma. Baltimore, MD, Williams and Willkins; ed 4. 1997, pp 376--94 3. Anand N. Deep sclerectomy with mitomycin C for glaucoma secondary to uveitis. Eur J Ophthalmol. 2011;21:708--14 4. Ang GS, Varga Z, Shaarawy T. Postoperative infection in penetrating versus non-penetrating glaucoma surgery. Br J Ophthalmol. 2010;94:1571--6 5. Ang M, Ho CL, Tan D, et al. Severe vernal keratoconjunctivitis requiring trabeculectomy with mitomycin C for corticosteroid-induced glaucoma. Clin Experiment Ophthalmol. 2011 May 17;. (Epub ahead of print). 6. Ataullah S, Biswas S, Artes PH, et al. Long term results of diode laser cycloablation in complex glaucoma using the Zeiss Visulas II system. Br J Ophthalmol. 2002;86:39--42 7. Auer C, Mermoud A, Herbort CP. Deep sclerectomy for the management of uncontrolled uveitic glaucoma: preliminary data. Klin Monbl Augenheilkd. 2004;221:339--42 8. Ayala M, Landau Högbeck I, Chen E. Inflammation assessment after selective laser trabeculoplasty (SLT) treatment. Acta Ophthalmol. 2011;89:306--9 9. Becker B. Intraocular pressure response to topical corticosteroids. Invest Ophthalmol. 1965;4:198--205 10. Birnbaum AD, Tessler HH, Schultz KL, et al. Epidemiologic relationship between fuchs heterochromic iridocyclitis and the United States rubella vaccination program. Am J Ophthalmol. 2007;144:424--8 11. Bloch-Michel E, Dussaix E, Sibillat M, et al. [PosnerSchlossmann syndrome. A cytomegalovirus infection?]. Bull Soc Ophtalmol Fr. 1988;88:75--6 12. Bodaghi B, Cassoux N, Wechsler B, et al. Chronic severe uveitis: etiology and visual outcome in 927 patients from a single center. Medicine (Baltimore). 2001;80:263--70 GLAUCOMA AND UVEITIS 13. Boyle JW, Netland PA, Salim S, et al. Uveitic glaucoma: pathophysiology and management. EyeNet. 2008;12:39--41 14. Busquets M, Zdrale N, Nairn J, et al. Intraocular pressure changes after removal of sub-tenon’s triamcinolone acetonide depot. Retinal Physician. 2010;7:45--8 15. Carreño E, Villarón S, Portero A, et al. Surgical outcomes of uveitic glaucoma. J Ophthalmic Inflamm Infect. 2011;1:43--53 16. Ceballos EM, Beck AD, Lynn MJ. Trabeculectomy with antiproliferative agents in uveitic glaucoma. J Glaucoma. 2002;11:189--96 17. Chang JH, McCluskey P, Missotten T, et al. Use of ocular hypotensive prostaglandin analogues in patients with uveitis: does their use increase anterior uveitis and cystoid macular oedema? Br J Ophthalmol. 2008;92:916--21 18. Cvenkel B. One-year follow up of selective laser trabeculoplasty in open-angle glaucoma. Ophthalmologica. 2004;218: 20--5 19. Damji KF, Shah KC, Rock WJ, et al. Selective laser trabeculoplasty v argon laser trabeculoplasty: a prospective randomised clinical trial. Br J Ophthalmol. 1999;83:718--22 20. Da Mata A, Burk SE, Netland PA, et al. Management of uveitic glaucoma with Ahmed glaucoma valve implantation. Ophthalmology. 1999;106:2168--72 21. Dupas B, Fardeau C, Cassoux N, et al. Deep sclerectomy and trabeculectomy in uveitic glaucoma. Eye (Lond). 2010;24: 310--4 22. Falcon MG, Williams HP. Herpes simplex keratouveitis and glaucoma. Trans Ophthalmol Soc UK. 1978;98:101--4 23. Fechtner RD, Khouri AS, Zimmerman TJ, et al. Anterior uveitis associated with latanoprost. Am J Ophthalmol. 1998; 126:37--41 24. Fortuna E, Cervantes-Castañeda RA, Bhat P, et al. Flare-up rates with bimatoprost therapy in uveitic glaucoma. Am J Ophthalmol. 2008;146:876--82 25. Foster CS, Davanzo R, Flynn TE, et al. Durezol (Difluprednate Ophthalmic Emulsion 0.05%) compared with Pred Forte 1% ophthalmic suspension in the treatment of endogenous anterior uveitis. J Ocul Pharmacol Ther. 2010;26:475--83 26. Foster CS, Havrlikova K, Baltatzis S, et al. Secondary glaucoma in patients with juvenile rheumatoid arthritis--associated iridocyclitis. Acta Ophthalmol Scand. 2000;78:576--9 27. Foster CS, Vitale AT. Diagnosis and treatment of Uveitis, in Foster CS, Vitale AT (eds). WB Saunders; 1st ed., 2002, pp 17--23 28. Freedman SF, Rodriguez-Rosa RE, Rojas MC, et al. Goniotomy for glaucoma secondary to chronic childhood uveitis. Am J Ophthalmol. 2002;133:617--21 29. Gil-Carrasco F, Salinas-VanOrman E, Recillas-Gispert C, et al. Ahmed valve implant for uncontrolled uveitic glaucoma. Ocul Immunol Inflamm. 1998;6:27--37 30. Gritz DC, Wong IG. Incidence and prevalence of uveitis in Northern California; the Northern California Epidemiology of Uveitis Study. Ophthalmology. 2004;111:491--500 31. Gupta K, Hoepner J, Streeten B. Pseudomelanoma of the iris in herpes simplex keratouveitis. Ophthalmology. 1986; 93:1524--7 32. Heinz C, Koch JM, Zurek-Imhoff B, et al. Prevalence of uveitic secondary glaucoma and success of nonsurgical treatment in adults and children in a tertiary referral center. Ocul Immunol Inflamm. 2009;17:243--8 33. Herbert HM, Viswanathan A, Jackson H, et al. Risk factors for elevated intraocular pressure in uveitis. J Glaucoma. 2004;13:96--9 34. Hill RA, Nguyen QH, Baerveldt G, et al. Trabeculectomy and molteno implantation for glaucomas associated with uveitis. Ophthalmology. 1993;100:903--8 35. Hirose S, Ohno S, Matsuda H. HLA-Bw54 and glaucomatocyclitic crisis. Arch Ophthalmol. 1985;103:1837--9 36. Ho CL, Wong EY, Walton DS. Goniosurgery for glaucoma complicating chronic childhood uveitis. Arch Ophthalmol. 2004;122:838--44 37. Hong C, Song KY. Effect of apraclonidine hydrochloride on the attack of Posner Schlossman syndrome. Korean J Ophthalmol. 1993;7:28--33 9 38. Hoskins DH, Hetherington J, Shaffer RN. Surgical management of the inflammatory glaucomas. Perspect Ophthalmol. 1977;1:173--81 39. Hung PT, Chang JM. Treatment of glaucomatocyclitic crises. Am J Ophthalmol. 1974;77:169--72 40. Juzych MS, Chopra V, Banitt MR, et al. Comparison of longterm outcomes of selective laser trabeculoplasty versus argon laser trabeculoplasty in open-angle glaucoma. Ophthalmology. 2004;111:1853--9 41. Kaburaki T, Koshino T, Kawashima H, et al. Initial trabeculectomy with mitomycin C in eyes with uveitic glaucoma with inactive uveitis. Eye (Lond). 2009;23: 1509--17 42. Kafkala C, Hynes A, Choi J, et al. Ahmed valve implantation for uncontrolled pediatric uveitic glaucoma. JAAPOS. 2005; 9:336--40 43. Kanski JJ, Shun-Shin GA. Systemic uveitis syndromes in childhood: an analysis of 340 cases. Ophthalmology. 1984; 91:1247--52 44. Karbassi M, Raizman MB, Schuman JS. Herpes zoster ophthalmicus. Surv Ophthalmol. 1992;36:395--410 45. Key SN 3rd, Kimura SJ. Iridocyclitis associated with juvenile rheumatoid arthritis. Am J Ophthalmol. 1975;80:425--9 46. Kimura SJ, Hogan MJ, Thygeson P. Fuchs’ syndrome of heterochromic cyclitis. AMA Arch Ophthalmol. 1955;54: 179--86 47. Kishi A, Nao-i N, Sawada A. Ultrasound biomicroscopic findings of acute angle-closure glaucoma in Vogt-KoyanagiHarada syndrome. Am J Ophthalmol. 1996;122:735--7 48. Knox DL. Glaucomatocyclitic crises and systemic disease: peptic ulcer, other gastrointestinal disorders, allergy and stress. Trans Am Ophthalmol Soc. 1988;86:473--95 49. Liesegang TJ. Classification of herpes simplex virus keratitis and anterior uveitis. Cornea. 1999;18:127--43 50. Liesegang TJ. Clinical features and prognosis in Fuchs uveitis syndrome. Arch Ophthalmol. 1982;100:1622--6 51. Markomichelakis NN, Kostakou A, Halkiadakis I, et al. Efficacy and safety of latanoprost in eyes with uveitic glaucoma. Graefes Arch Clin Exp Ophthalmol. 2009;247:775--80 52. Matsuda K, Izawa Y, Mishima S. Prostaglandins and glaucomatocyclitic crisis. Jpn J Ophthalmol. 1975;19:368--75 53. Mendrinos E, Mermoud A, Shaarawy T. Nonpenetrating glaucoma surgery. Surv Ophthalmol. 2008;53:592--630 54. Merayo-Lloves J, Power WJ, Rodriguez A, et al. Secondary glaucoma in patients with uveitis. Ophthalmologica. 1999; 213:300--4 55. Miserocchi E, Waheed NK, Dios E, et al. Visual outcome in herpes simplex virus and varicella zoster virus uveitis: a clinical evaluation and comparison. Ophthalmology. 2002;109:1532--7 56. Moorthy RS, Mermoud A, Baerveldt G, et al. Glaucoma associated with uveitis. Surv Ophthalmol. 1997;41:361--94 57. Morad Y, Donaldson CE, Kim YM, et al. The Ahmed drainage implant in the treatment of pediatric glaucoma. Am J Ophthalmol. 2003;135:821--9 58. Neri P, Azuara-Blanco A, Forrester JV. Incidence of glaucoma in patients with uveitis. J Glaucoma. 2004;13:461--5 59. Netland PA, Denton NC. Uveitic glaucoma. Contemp Ophthalmol. 2006;5:1--26 60. Papadaki TG, Zacharopoulos IP, Pasquale LR, et al. Longterm results of Ahmed glaucoma valve implantation for uveitic glaucoma. Am J Ophthalmol. 2007;144:62--9 61. Patitsas CJ, Rockwood EJ, Meisler DM, et al. Glaucoma filtering surgery with postoperative 5-fluorouracil in patients with intraocular inflammatory disease. Ophthalmology. 1992;99:594--9 62. Prata JA Jr, Neves RA, Minckler DS, et al. Trabeculectomy with mitomycin C in glaucoma associated with uveitis. Ophthalmic Surg. 1994;25:616--20 63. Pujari S, Siddique SS, Zakka F et al. Selective Laser Trabeculoplasty for Uveitic Glaucoma: A One-Year Follow Up. Submitted to Ocular Immunology and Inflammation. 64. Quentin CD, Reiber H. Fuchs heterochromic cyclitis: rubella virus antibodies and genome in aqueous humor. Am J Ophthalmol. 2004;138:46--54 10 Surv Ophthalmol 58 (1) January--February 2013 65. Raitta C, Vannas A. Glaucomatocyclitic crisis. Arch Ophthalmol. 1977;95:608--12 66. Rao PV, Deng PF, Kumar J, et al. Modulation of aqueous humor outflow facility by the Rho kinase--specific inhibitor Y-27632. Invest Ophthalmol Vis Sci. 2001;42:1029--37 67. Realini T. Selective laser trabeculoplasty: a review. J Glaucoma. 2008;17:497--502 68. Sallam A, Sheth HG, Habot-Wilner Z, et al. Outcome of raised intraocular pressure in uveitic eyes with and without a corticosteroid-induced hypertensive response. Am J Ophthalmol. 2009;148:207--13 69. Sijssens KM, Rothova A, Berendschot TT, et al. Ocular hypertension and secondary glaucoma in children with uveitis. Ophthalmology. 2006;113:853--9 70. Smith JR. Managing uveitic glaucoma. Asian J Ophthalmol. 1999;1:8--11 71. Smith SL, Pruitt CA, Sine CS, et al. Latanoprost 0.005% and anterior segment uveitis. Acta Ophthalmol Scand. 1999;77: 668--72 72. Souissi K, El Afrit MA, Trojet S, et al. Deep sclerectomy for the management of uveitic glaucoma. J Fr Ophtalmol. 2006; 29:265--8 73. Stavrou P, Murray PI. Long-term follow-up of trabeculectomy without antimetabolites in patients with uveitis. Am J Ophthalmol. 1999;128:434--9 74. Stavrou P, Misson GP, Rowson NJ, et al. Trabeculectomy in uveitis: are antimetabolites necessary at the first procedure? Ocular Immunol Inflamm. 1995;3:209--16 75. Sundmacher R, Neumann-Haefelin D. Herpes simplex virus isolation from the aqueous of patients suffering from focal iritis, endothelitis, and prolonged disciform keratitis with glaucoma. Klin Montatsbl Augenheilkd. 1979;104:488 76. Tektas OY, Heinz C, Heiligenhaus A, et al. Morphological changes of trabeculectomy specimens in different kinds of uveitic glaucoma. Curr Eye Res. 2011;36:442--8 77. The Herpetic Eye Disease Study Group. Acyclovir for the prevention of recurrent herpes simplex virus eye disease. N Engl J Med. 1998;339:300--6 78. Towler HM, McCluskey P, Shaer B, et al. Long-term follow-up of trabeculectomy with intraoperative 5fluorouracil for uveitis-related glaucoma. Ophthalmology. 2000;107:1822--8 79. Towler HM, Bates AK, Broadway DC, et al. Primary trabeculectomy with 5-fluorouracil for glaucoma secondary to uveitis. Ocular Immunol Inflamm. 1995;3:163--70 80. Tripathi RC, Kirschner BS, Kipp M, et al. Corticosteroid treatment for inflammatory bowel disease in pediatric patients increases intraocular pressure. Gastroenterology. 1992;102:1957--61 SIDDIQUE ET AL 81. Uchoa UB, Rezende RA, Carrasco MA, et al. Long-term acyclovir use to prevent recurrent ocular herpes simplex virus infection. Arch Ophthalmol. 2003;121:1702--4 82. Vadot E. Epidemiology of intermediate uveitis: a prospective study in Savoy. Dev Ophthalmol. 1992;23:33--4 83. Vernon SA, Koppens JM, Menon GJ, et al. Diode laser cycloablation in adult glaucoma: long-term results of a standard protocol and review of current literature. Clin Experiment Ophthalmol. 2006;34:411--20 84. Wand M, Gaudio AR, Shields MB. Latanoprost and cystoid macular edema in high-risk aphakic or pseudophakic eyes. J Cataract Refract Surg. 2001;27:1397--401 85. Warwar RE, Bullock JD, Ballal D. Cystoid macular edema and anterior uveitis associated with latanoprost use. Experience and incidence in a retrospective review of 94 patients. Ophthalmology. 1998;105:263--8 86. Wolf MD, Lichter PR, Ragsdale CG. Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology. 1987;94:1242--8 87. Wright MM, McGehee RF, Pederson JE. Intraoperative mitomycin-C for glaucoma associated with ocular inflammation. Ophthalmic Surg Lasers. 1997;28:370--6 88. Yalvac IS, Sungur G, Turhan E, et al. Trabeculectomy with mitomycin-C in uveitic glaucoma associated with Behçet disease. J Glaucoma. 2004;13:450--3 89. Yamamoto S, Pavan-Langston D, Tada R, et al. Possible role of herpes simplex virus in the origin of Posner Schlossman syndrome. Am J Ophthalmol. 1995;119:796--8 90. Yamashita T, Kodama Y, Tanaka M, et al. Steroid-induced glaucoma in children with acute lymphoblastic leukemia: a possible complication. J Glaucoma. 2010;19:188--90 Other Cited Materials A. Unpublished data B. Herdnon L Jr. Glaucoma, uveitic treatment, and management. http://emedicine.medscape.com/article/1206838overview. Accession date 30 May 2012 C. Salim S, Boyle JW, Netland PA. Pathophysiology and management uveitic glaucoma. Ophthalmic Pearls: Glaucoma (Sep 2008). http://www.aao.org/publications/ eyenet/200809/pearls.cfm. Accession date 29 May 2012 Reprint address: C. Stephen Foster, MD, FACS, FACR, Massachusetts Eye Research and Surgery Institution, 5 Cambridge Center, 8th floor, Cambridge, MA 02412. e-mail: [email protected]. Outline I. Introduction II. Pathogenesis of glaucoma associated with uveitis III. Signs and symptoms IV. Uveitic disorders associated with glaucoma A. B. C. D. Fuchs heterochromic uveitis Posner-Schlossman syndrome Juvenile idiopathic arthritis Herpetic uveitis V. Management A. Medical B. Surgical 1. 2. 3. 4. 5. 6. Laser iridotomy Trabeculectomy Non-penetrating glaucoma surgery Glaucoma drainage device implantation Stents Cycloablation VI. Conclusion VII. Method of literature search VIII. Disclosure