Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
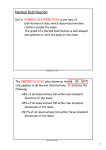
All About the OCT: Glaucoma Fall 2014 Disclosure All About the OCT: Glaucoma • Michael Chaglasian, O.D. is a paid advisor, consultant or researcher for the following commercial/industry groups: – Allergan, Alcon Labs, Carl Zeiss Meditec Michael Chaglasian, O.D. Associate Professor Illinois College of Optometry Illinois Eye Institute [email protected] OCT Image Acquisition “Cube of Data” • Similar to ultrasound but uses light instead of sound to image tissue • Beam of light is directed into tissue and reflections coming from different layers of the tissue are received by a detector Time Domain OCT artifacts can be common Time Domain OCT: susceptible to eye movements •768 pixels (A‐scans) captured in 1.92 seconds is slower than eye movements •Stabilizing the retina reveals true scan path (white circles)1 1. Koozekanani, Boyer and Roberts. “Tracking the Optic Nervehead in OCT Video Using Dual Eigenspaces and an Adaptive Vascular Distribution Model”; IEEE Transactions on Medical Imaging, Vol. 22, No. 12, 2003 1. 2. 3. M. Chaglasian, OD Sadda, Wu, et al. Ophthalmology 2006;113:285‐293 Ray, Stinnett, Jaffe . Am J Ophth 2005; 139:18‐29 Bartsch, Gong, et al. Proc. of SPIE Vol. 5370; 2140‐2151 1 All About the OCT: Glaucoma Fall 2014 Spectral Domain OCT Spectral Domain: Many Options • Enhance sensitivity and specificity in disease detection and reduce uncertainty in glaucoma suspects. • Improved software is available to help detect disease progression. Spectral Domain: Many Options Spectral Domain: Why?? • Enhanced reproducibility and registration. • Objective quantitative data that supports standardization of care at an expert level. • Pinpoint correlations in ocular structure and function, matching areas of abnormal tissue with attendant vision problems. Key Advantage: Progression Analysis Spectral Domain OCT Time Domain OCT SPECTRALIS Stratus 14 M. Chaglasian, OD 2 All About the OCT: Glaucoma How to “Read” a Printout • FIRST!: Signal Strength – A KEY indicator of image quality – Should be 7/10 or higher on Cirrus – DO NOT interpret poor quality scan as “red” disease • Well centered image • No evidence of movement artifact • Review Plots and Displays – Thickness Map and Deviation Map – Quadrant and Sector Plots – TSNIT and Optic Nerve B‐Scan Zeiss: Cirrus OCT Printouts Fall 2014 Printout Signal Strength Here RNFL THICKNESS MAP shows the patterns and thickness of the nerve fiber layer within the full 6mm x 6mm area RNFL thickness and comparison to normative data is shown in circle, quadrants and clock hour display RNFL DEVIATION MAP, overlaid on the OCT fundus image, illustrates precisely where RNFL thickness deviates from the normal range. Data points that are not within normal limits are indicated in red and yellow. Quadrant and Sector MAPs in middle of page Glaucoma – RNFL Thickness Analysis The RNFL thickness map shows the patterns and thickness of the nerve fiber layer within the 6mm x 6mm cube Yellow and Red = Good / Normal • The RNFL deviation map is overlaid on the OCT fundus image to illustrate precisely where RNFL thickness deviates from a normal range • Yellow and Red = Bad / Abnormal RNFL Glaucoma – RNFL Thickness Analysis: TSNIT RNFL thickness is displayed in graphic format and compared to agematched normative data M. Chaglasian, OD 3 All About the OCT: Glaucoma Normative Data: Glaucoma Fall 2014 Example Normative Data: • Average RNFL Thickness Distribution of Normals: • • • • • • RNFL Symmetry Rim Area Disc Area Average C/D Ratio Vertical C/D Ratio Cup Volume Color coded indication of normative data comparison for RNFL and ONH. • The thickest 5% fall in the white area. • 90% of measurements fall in the green area. • The thinnest 5% fall in the yellow area or below. • The thinnest 1% of fall in the red area. • Measurements in red are considered outside normal limits. • ONH values will be shown in gray when the disc area does not match with normative data. Example Normative Data: NEW: Ganglion Cell Analysis • Measures thickness for the sum of the ganglion cell layer and inner plexiform layer (GCL + IPL layers) using data from the Macular 200 x 200 or 512 x 128 cube scan patterns. Carl Zeiss Meditec, Inc Cirrus 6.0 Speaker Slide Set CIR.3992 Rev B 01/2012 Anatomy: Ganglion Cell Layer and IPL Cirrus: Ganglion Cell Analysis The analysis contains: • Data for both eyes (OU) • Thickness Map – – shows thickness measurements of the GCL + IPL in the 6mm by 6mm cube and contains an elliptical annulus centered about the fovea. • Deviation Maps – – shows a comparison of GCL + IPL – thickness to normative data. • Thickness table – – shows average and minimum thickness within the elliptical annulus. M. Chaglasian, OD 4 All About the OCT: Glaucoma Macular/Ganglion Cell Analysis for Glaucoma • Is a “complement” to traditional RNFL scans • Has a large number of false positives. • Should NOT be used as the sole basis of a diagnosis for glaucoma. Fall 2014 What are practitioners' most common misunderstandings of imaging technology? “The thought that these devices can diagnose glaucoma in the absence of corroborating clinical evidence is, in my opinion, the most common (and potentially dangerous) misunderstanding. The limited normative databases against which scans are compared can never cover the remarkably varied appearance and structure of the optic nerve we encounter in normal individuals.” James Brandt, MD Red Disease! Red Disease Disc Photos CASE EE IOP 21‐24 mmHg CCT 545 M. Chaglasian, OD 5 All About the OCT: Glaucoma Fall 2014 Visual Fields Combined Report Disc Photos CASE MZ IOP in high teens CCT= 560 M. Chaglasian, OD 6 All About the OCT: Glaucoma Fall 2014 Visual Fields CASE CM 38 yo GAT= 22 OD 25 OS Visual Fields M. Chaglasian, OD 7 All About the OCT: Glaucoma Fall 2014 Two important questions every glaucoma practitioner has: Combined Report • Is my patient getting worse? Newer Question: • What is the rate of progression? • Variability in perimetric testing • Can we quantify this? • Challenges of ONH serial assessment – How can I tell for certain? Different Rates of Progression Caprioli J. AJO 2008 M. Chaglasian, OD Variability in Progression Rates Heijl A. Acta Ophthalmol. 2013: 91: 92–99 8 All About the OCT: Glaucoma Fall 2014 Progression in Glaucoma: EMGT Progression in Glaucoma: EMGT ~ -0.08 dB/yr 3x Normal Aging Rate Rate of Progression Range ~ -4 dB/yr 90 x Normal Rate ~ -0.05 dB/yr 2x Normal Aging Rate Rate of Progression Range ~ -0.60 dB/yr 12x Normal Aging Rate ~ -0.35 dB/yr 7x Normal Aging Rate ~ -2.5 dB/yr 50x Normal Aging Rate Zeiss Humphrey GPA Summary Printout Glaucoma Progression Index CONCLUSIONS: Glaucoma progression rates calculated using the GPI seem to be considerably less affected by cataract and cataract surgery than rates based on the traditional MDI. Am J Ophthalmol 2008;145:343–353 GPA Summary Printout Baseline Exams Visual Field Index Visual Field Index (VFI) Central points weighted more heavily than those on periphery Reduces cataract contribution to the measurement of VF loss B A Most Recent Test VFI = 90% VFI = 81% “ B”has more damaged central points and lower VFI than“A”. M. Chaglasian, OD 9 All About the OCT: Glaucoma Fall 2014 Measures of Progression: Trend Analysis HFA GPA VFI Summary - Interpretation at a Glance Trend Analysis Loss to date Projected future loss 100% • “Measures the rate of change” • A regression line is drawn to determine rate of change for all the data that has been collected over time. The VFI Bar • historical and projected VFI loss • Using VFI measures a % rate of change • Most valuable when multiple VF tests have been completed • Good for identifying fast progressors Arch Ophthalmol. 2009;127(12):1610-1615 GPA Summary Report: Baseline Trend Analysis GPA Summary Report: Trend Analysis Most Recent Exam Zeiss: Cirrus OCT Printouts Case Example: Progression Left Eye? Visual Field is Stable M. Chaglasian, OD 10 All About the OCT: Glaucoma Fall 2014 Cirrus GPA Progression Report How to Evaluate Progression? Cirrus OCT GPA Analysis Cirrus RNFL “Event” Analysis • Event Analysis: – Progression is defined when the difference between baseline and follow up is greater than test‐retest SS = 10 Baseline Registration SS = 10 Baseline Registration SS = 8 Registration SS = 9 • Trend Analysis: – Progression is defined when there is a significant negative slope of a regression line, which is performed on a particular parameter Patterns of Progression • Two baseline exams are required • Yellow Coded: Change greater than test-retest variability. • Red: Confirmed on follow up. Appearance of Defect • Initial Appearance of Defect • Widening of Defect • Deepening of Defect Leung et al. Ophthalmol 2012 M. Chaglasian, OD Leung et al. Ophthalmol 2012 11 All About the OCT: Glaucoma Fall 2014 Widening of Defect Deepening of Defect Leung et al. Ophthalmol 2012 Leung et al. Ophthalmol 2012 Cirrus RNFL/ONH Trend Analysis Cirrus GPA Analysis Four Parameters: Average, Superior, Inferior RNFL; Average C/D Ratio Trend Analysis: Statistical Program A Regression Line is drawn to determine rate of change for all the data that has been collected over time. RNFLT (microns) Less variability with Structural/OCT testing as compared to Functional/ Visual Field testing. 250 TSNIT Progression Graph 200 150 100 50 TSNIT values from each exam are shown Significant difference is colorized yellow or red Yellow denotes change from both baseline exams Red denotes change from 3 of 4 comparisons 0 0 50 100 150 200 250 TSNIT Cirrus GPA: Trend Analysis Cirrus Guided Progression Analysis Page 1 Page 2 • Average RNFL Thickness values are plotted for each exam. • Yellow marker denotes change from both baseline exams. • Red marker denotes change sustained over consecutive visits. • Rate and significance of change are shown in text M. Chaglasian, OD Ver 6.0 77 12 All About the OCT: Glaucoma Fall 2014 Page 2 Data Cirrus GPA: TSNIT Analysis •TSNIT values from baseline and current exams are plotted. •Areas of statistically significant change are color‐coded yellow when first noted and then red when the change is sustained over consecutive visits. •Progression is less frequently noted on this plot. Leung, 2012 Cirrus GPA™ Analysis RNFL Summary • Legend summarizes GPA analyses and indicates with a check mark if there is possible or likely loss of RNFL • RNFL Thickness Map Progression (best for focal change) • RNFL Thickness Profiles Progression (best for broader focal change) • Average RNFL Thickness Progression (best for diffuse change) M. Chaglasian, OD 13 All About the OCT: Glaucoma Limitations to OCT Progression Fall 2014 Age Related Change: • Age Related RNFL and Macular Thinning: – Is not accounted for in the analysis – ‐0.52 µm/year and ‐0.25 µm/year • Leung et al Ophthalmology 2012, 2013 – thus, not all negative slope is disease related and may not be related to glaucoma progression • Review all clinical findings, do not base management decisions on OCT alone – Avoid “Red Disease” Leung. Curr Opinion 2013 Disc Photos CASE VM 48 yo Several Year History of OHTN CCT ~ 575µ Negative Family History Monitored q3‐4m without Treatment Current and Initial OCT M. Chaglasian, OD Right OCT 14 All About the OCT: Glaucoma Fall 2014 Left OCT GPA Visual Fields Ganglion Cell Analysis Case EG • • • • • • • 67 yo, AA male, Retired school teacher Good health, no medications + Family History of glaucoma OHTN/Early Glaucoma CCT= 565, 555 Pre‐ Tx IOP ~ 30 mmHg OD, OS With PGA: – Always 20‐23 mmHg x 5+yrs – Good Compliance ONH Photos M. Chaglasian, OD Current and Initial 15 All About the OCT: Glaucoma Fall 2014 Progression? Cirrus GPA: Stable OD and OS Page 2 Data GPA Visual Fields GCA Case EW • 73 yo, “Snowbird” • Pseudophakic OU • PreTx GAT: – 34 mmHg and 24 mmHg • Currently: – 22 and 18 mmHg on a PGA M. Chaglasian, OD 16 All About the OCT: Glaucoma Photos Current and Initial OCTs Cirrus GPA Right Eye: Page 2 Data GPA Visual Fields M. Chaglasian, OD Fall 2014 GCA 17 All About the OCT: Glaucoma Detection of Progression using both Structure and Function • Structural tests not necessarily better than functional tests in early disease • Both imaging and visual function tests should be used to monitor OHT and early glaucoma • Earliest detection/progression will vary amongst patients M. Chaglasian, OD Fall 2014 Take Home Message: • RNFL and ONH Progression Analysis on OCTs is now at a higher level. – Macular/Ganglion Cell Scans may be included in the future • Structural Progression Analysis will become a regular part of the best practice patterns for glaucoma. 18 All About the OCT: Retina Disclosure Statement Retinal and OCT Grand Rounds Steven Ferrucci, OD, FAAO Chief, Optometry Sepulveda VA Professor, SCCO/MBKU OCT Technology: Advantages Has ushered in a whole new era of retinal care Diagnosis Response to treatment New diagnoses once only speculated VMT Macular Schisis Information once only available through histopathology or dissection Can replace FA in some cases CME S. Ferrucci, OD Speakers bureau/Advisory Board Alcon Macula Risk MacuLogix Nicox Autogenomics Science Based Health Thrombogenics OCT Technology: Caveats DOES NOT take place of clinical exam! DOES NOT take place of careful history taking DOES NOT replace FA in some cases! DOES NOT REPLACE COMMON SENSE! ONE MORE PIECE OF CLINICAL PICTURE Not the end all be all!! Not to be taken in vacuum FA 1 All About the OCT: Retina Plaquenil Toxicity: How Prevalent? 1: 10-2 2: ERG 3. SD-OCT 4. FAF Reading the OCT associated with plaquenil toxicity Normal Patient Where’s the damage? Plaquenil Patient Impact of the guidelines on today's practice! AJO 8/2013 OCT: Saucerazation & Sinkhole appearance perifoveal outer retinal abnormalities displacement of the inner retinal structures toward the RPE with increase retinal atrophy n=183 pts came for f/u & 36 were evaluated for baseline Evaluated by 26 ophthalmologist & 3 ODs Results 40% increase on health care cost No additional pts discover with toxicity in accordance to new guideline. Incidence of toxicity remains at 1%, as noted in f/u pts No pts was followed at recommended guidelines of 5-year period after baseline (even if low-risk patient) Chen et al. Clinical Ophthalmology 2010 S. Ferrucci, OD 2 All About the OCT: Retina Macular Thickness Normative Data Cirrus HD-OCT Healthy Macula NFL ILM GCL IPL INL OPL ONL Macular thickness is compared to an agematched normative database as indicated by a stop-light color code ELM NFL: Nerve Fiber Layer ILM: Inner Limiting Membrane GCL: Ganglion Cell Layer IPL: Inner Plexiform Layer INL: Inner Nuclear Layer IS IS/OS OS OPL: Outer Plexiform Layer ONL: Outer Nuclear Layer ELM: External limiting membrane IS: Photoreceptor Inner Segment RPE Choroid IS/OS: Junction of inner and outer photoreceptor segments OS: Photoreceptor Outer Segment RPE: Retinal Pigment Epithelium 13 Retinal Layers ! EXAMPLES Basic B-Scan Interp. MH Case MH Case 65 yo Hispanic male CC: decreased VA OS for several years. Unsure of exact diagnosis. Was curious if anything could be done to improve vision. Laser? Injection? Oc hx: (+) POAG father and sister Med hx: hyperlipidemia VA cc 20/20 OD, 20/200 OS Ant seg: unremarkable S. Ferrucci, OD 3 All About the OCT: Retina Macular Hole Macular Hole Full thickness macular hole OS Consult with retinal specialist Felt that due to duration of situation, unlikely that any surgery would have meaningful benefit on vision RTC q 6 mos Monocular precautions including polycarbonate RX Macular Hole Present as a circular to oval depression of varying degrees in the avascular area of the macula May have surrounding cuff of edema Most common cause is idiopathic other causes include blunt trauma, severe myopia, solar retinopathy, CME Highest incidence in 7th decade of life Women 2x as often as men Macular Hole-OCT Vision typically 20/80 to 20/200 with fullthickness hole If pt has macular hole in one eye, 28-44% chance of macular hole in other eye w/o a PVD If PVD already, very little chance Watzke-Allen sign useful to differentiate true hole from similar appearance OCT very useful FTMH S. Ferrucci, OD 4 All About the OCT: Retina VMT CASE VMT OCT 80 yo male Decreased VA OS x 1 mos 20/20 OD, 20/125 OS Med Hx: HTN, DM, CAD, s/p CVA Meds: acarbose, metformin, glipizide, lisinopril, simvastatin Post op OCT VMT Case Dx: VMT with CME OS Pt underwent Avastin x 1 OS followed by PPV and membrane peel OS POM #1 VA 20/200 OS! Another presentation Examination 60 yo male presents for yearly diabetic exam Cc: noted left eye had blurry spot in center of vision, with lines compressed and distorted vertically Med Hx: Type II DM x 3 years, HTN, Hyperlipidemia Oc Hx: unremarkable BVA: OD 20/20, OS 20/50 Amsler Grid: OD WNL OS central distortion, metamorphopsia Post pole: S. Ferrucci, OD 5 All About the OCT: Retina OD 194um VMT Case OD 397um Last VMT Case 63 yo white male 1 wk, noted straight lines were curved, both horizontally and vertically left eye Lines of text seemed “shrunken” as well, OS Pt seen about 3 mos previous for routine exam Unremarkable, 20/20 OU Mild HTN, ED HCTZ, vardenafil Last VMT Case 12/2011 VA 20/30-1 CRT: 241 S. Ferrucci, OD A: VMT OS with impending macular hole Window defect on FA with no leakage P: repeat OCT in 1 month to see if hole progresses or resolves Pt agrees with plan VA has since increased OS to 20/30+ with decreased metamorphopsia Last VMT case 9/2011: VA 20/20 OD, 20/40 OS OCT: CRT 309 Pt elects to wait and see what happens Last VMT Case 3/2012 VA 20/20 CRT: 3/2/2012 183 6 All About the OCT: Retina VMT: Vitreomacular Traction VMT syndrome is characterized by a partial detachment of the posterior detachment with persistent adherence to the macula Can lead to CME, ERM, and macular hole formation Once thought to be relatively rare, with advent of OCT now being seen more and more In one study, 8% of pts were thought to have VMT by clinical observation only, but 30% by OCT VMT VMT VMT More commonly encountered in older women Can occur in either sex, and age, no apparent racial predilection Aphakia and pseudophakia are protective, as these patient typically have a complete PVD Pts may report decreased vision, metamorphopsia and photopsia VMT Natural progression of disease is rather variable Slow progression possible with near normal acuity Approx 10% will have spontaneous PVD and resolution Therefore, close monitoring my be advised for some patients S. Ferrucci, OD Clinically, very hard to diagnose PVD with adherence to macular area Can present as macular surface wrinkling/striae , similar to ERM, or loss of foveal reflex May also note a thickened posterior hyaloid membrane Retinal blood vessel distortion straightening may be present Retinal thickening /macular edema may be associated OCT IS THE KEY!!!! VMT In patients with poor vision, or symptomatic, a pars planar vitrectomy (PPV) may be considered Duration, severity should also be considered Literature repots up to a 75% success rate and improvement of vision following PPV 7 All About the OCT: Retina Jetrea (Ocriplasmin) Intravitreal injection of thrombolytic agent that causes lysis of vitreous Pharmacologic vitrectomy FDA approved October 2012 for treatment of symptomatic vitreomacular adhesion Two phase 3 trails 26.5% of pts had resolution of VMA vs. 10.1% with placebo Minimal adverse effects 0.125 mg (0.1 ml) injection Available January 2013 Cost? ERM Case 78 year old male Notes mild decreased VA OS, and lines appear “crooked when reading” OS. Older brother has AMD so worried Med hx: unremarkable NO MEDS!!! Oc hx: unremarkable, older brother with “bad” AMD VA : OD 20/20-1, OS 20/40 ERM OS ERM Case OD: Normal OS: ERM ERM Case ERM Case 2 Due to good VA, pt defers consult to retina service for possible membrane peel/PPV Pt relieved it is not AMD!! RTC 6-12 mos HAG 2011 63 yo male Just wants new glasses Feels OS is not as good as OD 20/20 OD, 20/40 OS S. Ferrucci, OD 8 All About the OCT: Retina ERM case 2 -2011 20/25 20/40: mild ERM ERM Case 2 Mild ERM OS Overall satisfied with acuity “95% of the time” Not that interested in retinal consult RTC 1 yr or PRN ERM Case 2 Pt comes back in 2014, about 3.5 years later Feels Vision may be “a tad worse “ OS ERM Case 2 ERM Case 2 ERM OS, progressed VA from 20/40 to 20/150 Pt offered retinal consult Pt ed that VA reduced and good time for surgical evaluation Decides not really bothered, so defers Comes back a week later and states saw outside retinal specialist (with his wife) who recommended sx Suddenly symptomatic!!!! Refer to Retina clinic PPV/MP OS scheduled in 1 mos Happy with vision “90% of the time” S. Ferrucci, OD 9 All About the OCT: Retina ERM case 3 ERM case 3 67 yo male Notes gradual decreased VA OD x 1 yr 20/70 OD 20/20 OS 1+ NSC OU Does not seem like 20/70 cataract Fundus appears normal Plan: get OCT ERM case 3 ERM case 3 Epi-retinal Membrane ERM case 3 ERM with traction OD on OCT CRT 472 vs 296 No edema on FA Refer to retina clinic for surgical eval ERM peel S. Ferrucci, OD AKA macular pucker, cellophane maculopathy Can be secondary to peripheral retinal disease, such as detachment or tear; a retinal vascular disease such as BRVO; inflammation; trauma or idiopathic Idiopathic tend to be more mild and nonprogressive vs. those after retinal tear 10 All About the OCT: Retina Epi-retinal Membrane VA can range from 20/20 to 20/200 or worse Studies show > 5% have worse than 20/200 Often metamorphopsia is only complaint with idiopathic ERM Fewer than 20% of cases are bilateral Surgical removal is considered if severe vision loss or distortion Epi-retinal Membrane Consider surgery if: VA 20/40 or worse Symptomatic Visual need of patient 30 minute procedure Face down compliance after surgery for up to 2 weeks Make sure you have an experienced surgeon!! Epi-retinal Membrane ERM S. Ferrucci, OD 11 All About the OCT: Retina CSR Case CSR Case 40 yo male. Works as used car salesman Presents with blurry vision OS x 3 days Med hx: HTN Meds: HCTZ VA 20/20 OD, 20/40 OS CSR Case CSR Case CSR OS Pt ed stress as risk factor as well as steroids RTC 1 mos Pt calls clinic 3 mos later. Reports saw local OD who said VA now 20/20 OS CSR case #2 38 year old male Small grey spot in central vision OS x 3 days Color distorted when looks through grey spot Peripheral vision normal Oc Hx: unremarkable Med Hx: h/o ulcerative colitis Meds: prednisone 30 mg/day S. Ferrucci, OD 12 All About the OCT: Retina CSR case 2 Consult to GI Clinic regarding systemic steroids as risk factor Pt eager to get off steroids Gained 30 lbs since started Unable to verify with FA as pt has h/o passing out when “sees a needle” Pt Ed: RTC 6-8 weeks EDI: Enhanced Depth Imaging Normal EDI CSR Case 3 56 yo white male h/o decreased VA OS x 30 yrs CSR case 3 20/20 20/20 Unknown etiology Was told might resolve on own Probably related to stress Med HX: mild HTN, obesity, ED, hip replacment S. Ferrucci, OD 13 All About the OCT: Retina EDI: Enhanced Depth Imaging Central Serous Retinopathy CSR Case 3 Inactive CSR in Macula New area temporal to macula Review with retinal specialist Agrees with findings PDT was discussed but not readily available Suggest grid laser OS since temporal due to previous vision loss Central Serous Retinopathy Pt typically presents with fairly recent onset of blurred VA in one eye with a scotoma, micropsia, or metamorphopsia VA typically 20/30-20/70 Often correctable with low hyperopic RX Unilateral in 70% of cases S. Ferrucci, OD Common disorder of unknown etiology which typically affects men between age 20 and 45 Males to females 10:1 Serous detachment of neurosensory retina due to leakage from small defect in RPE Central Serous Retinopathy Appears as a shallow round or oval elevation of the sensory retina often outlined by a glistening reflex FA is helpful in providing definitive diagnosis Classic Smoke stack appearance (occasionally) Ink-blot appearance OCT shows marked elevation 14 All About the OCT: Retina Central Serous Retinopathy Central Serous Retinopathy Risk factors Type A personality Stress Use of systemic cortico-steroids Pregnancy 80-90% of pts will undergo spontaneous resolution and return to normal (or near normal) VA within 1-6 mos. >60% resolve back to 20/20 Rare to have vision remain < 20/40 Approx 40% will get recurrence CNVM is VERY rare occurrence, but possible Central Serous Retinopathy No known medical therapy has been proven effective Topical steroids, NSAIDs etc Localized photocoagulation may be of some benefit, but only if Duration at least 4 months VA in other eye is reduced from other attacks Recurrent CSR has already reduced VA in that eye Pt is intolerant of vision and willing to take risk PDT suggested in some cases Avastin? Behavior modification? Solar Maculopathy 65 yo male No complaints Med hx: HTN, Obesity 20/30 OU h/o sungazing in past ≈15 yrs ago when cocaine/LSD abuser Solar Maculopathy Solar Maculopathy OCT characteristic for solar maculopathy Pt ed, monitor S. Ferrucci, OD 15 All About the OCT: Retina Solar Maculopathy Damage to the outer layers retina as shown on OCT Outer segment of photoreceptors and RPE Clinical exam, small yellowish lesion Acuity typically 20/40-20/60 Little to no correlation with appearance and acuity Greater risk in younger individuals who are more likely to start at sun or eclipse High Myopia 67 yo presents for annual exam. Wonders if glasses need update States never had great vision OS OD: -9.25-2.75x080 20/30-2 OS: -11.00-1.75x103 20/20- With clear lenses Also, schizophrenic pts, pts on LSD, etc. Macular Schisis Relatively new entity, ≈1999 by Takano and Kishi Prior to this, misinterpreted as shallow RD or even edema With OCT, thought to be not uncommon in highly myopic individuals with posterior staphyloma Characterized by intraretinal splitting, in both inner and outer retina, with cystoid spaces Macular Schisis OCT: Final Thoughts Fairly stable with time, with mild fluctuations in vision Treatment (vitrectomy) generally only recommended if vitreal traction, as may lead to macula hole Consider OCT in high myopes with central vision problems Has ushered in a whole new understanding of retinal disease Fast becoming the standard of care Many models /makes available S. Ferrucci, OD THANK YOU!! 16