Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
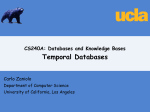
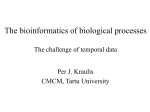
@aestheticsgroup Aesthetics Journal Aesthetics aestheticsjournal.com one point CPD Forehead Forehead rejuvenation and contouring strategies Mr Dalvi Humzah and Anna Baker discuss anatomically-sound approaches to treating and re-contouring the forehead The aesthetic practitioner is able to address and successfully treat many of the senescent changes of the upper face, in particular the forehead and glabellar, through a variety of nonsurgical injectable modalities. To achieve an effective result, a current and accurate anatomical awareness and detailed understanding of product suitability is imperative to reduce complications and yield an excellent cosmesis. In this article, a variety of techniques will be analysed in terms of their suitability to refine skin texture and re-contour this region. Key words Dermal filler, botulinum toxin A, anatomy, forehead, re-contouring Introduction When considering a ‘beautiful’ face, the forehead, in terms of height, contour and appearance, is accepted as one of the seven keystone areas to acknowledge.1 In this article, the anatomy of the forehead and glabellar will be reviewed with regard to the application of specific non-surgical cosmetic treatments. It is acknowledged that botulinum toxin is used to effectively reduce and soften the appearance of static and dynamic rhytides at the forehead and glabellar.2 The use of dermal fillers to re-contour this region can provide exceptional results.3 The current literature covers varied injection techniques to treat the upper face using botulinum toxin, Figure 1: S.C.A.L.P Layer one: Skin Layer two: Subcutaneous layer Layer three: Aponeurotic layer, commonly referred to as the SMAS layer; a strong musculo-aponeurotic sheet, encasing the whole face Layer four: Loose areolar tissue; a gliding plane to allow for mimetic expression Layer five: Periosteum/ deep tissue (muscle/fascia) but little is available in the context of forehead re-contouring. In this article, the authors will share their specialised techniques, underpinned by regional anatomy, with discussion of approaches described within the current literature available. The acronym below (used by many medical students) will be alluded to throughout the article, to allow the reader to clearly visualise the anatomical planes described for product placement.4 DH to reference -book The Forehead Topographically the forehead may be defined as the area bounded laterally by the superior temporal septum which arises from the temporal crest, inferiorly by the orbital rims with the supra orbital adhesion and nasion and superiorly the hairline (a variable which is difficult in those who are follicularly challenged).5 When describing the regional anatomy, many texts will address the course and details of individual structures, which while correct, fails to provide a three-dimensional description of the areas of interest for a nonsurgical practitioner. A different view is required when treating an area with what is essentially a blind approach, as the practitioner can not see the structures under the skin whether using a needle or cannula. The five-layered approach outlined above will enable a practitioner to quickly determine the position of product placement, and also understand where important structures are in relation to the approach utilised. It is, however, imperative when using this approach that the practitioner has an in-depth knowledge of the named structures in each area. Layer One: Skin A lot of vital anatomical information can be learnt by examination of this important structure. Apart from the overall appearance of the skin, and the ageing changes, superficial arterial and venous structures may be visible that will alert the injector to avoid puncturing these – and in doing so, avoid adverse events. The dynamic lines in the glabellar region define the underlying median/ Aesthetics | July 2015 11:27 27 CPD Forehead @aestheticsgroup The separation between the middle temporal compartment and lateral temporal compartment may occasionally be seen as an oblique depression on the skin in some patients. central fat compartment (see below). The glabella line also indicates the line of the supratrochlear vessels located near the subdermis, and the deep insertion of the medial portion of the corrugator. The lateral dermal attachments of the corrugator are often seen as a semicircular depression laterally.6 The horizontal forehead lines represent septal dermal attachments to the underlying frontalis, and when running horizontally indicate the contiguous nature of the frontalis muscle.7 The midline dip and lateral appearance of the forehead lines indicate the point of separation and lateral position of the muscle. This approach to injection, named the ‘objectivemuscle-identification approach’, will help the injector to accurately and effectively tailor toxin placement.8 Layer Two: Subcutaneous This is an important layer as many structures are located here and understanding this area in detail will allow a practitioner to reduce adverse events. Prior to the seminal work by Rohrich and Pessa, the subcutaneous fat was viewed as an amorphous structure under the skin. However, these authors identified three compartments.7 The (median) central compartment is located in the midline region of the forehead. It has a consistent location that abuts the middle temporal compartments on either side with an inferior border at the nasal dorsum (supratrochlear artery). The lateral boundary is possibly a septal barrier and could be referred to as the central temporal septum. The middle temporal fat compartments lie on either side of the central forehead, the inferior border is the orbicularis retaining ligament, and the lateral border corresponds to the superior temporal septum. The lateral temporal-cheek compartment connects the lateral forehead fat to the lateral cheek and cervical fat. The separation between the middle temporal compartment and lateral temporal compartment may occasionally be seen as an oblique depression on the skin in some patients. While these are important anatomic concepts, it is interesting to note that we are unclear as yet what their role is in the ageing of the forehead, unlike other regions that have been examined, for example the mid-face fat 28 Aesthetics Journal Aesthetics aestheticsjournal.com compartments as described by Gierloff et al.9 Other important structures are the nerves and vessels. The Trigeminal nerve (Cranial nerve V) branches supply the sensory innervation to the forehead.5 Lateral to the medial end of the upper margin of the orbit, the supraorbital nerve indents the bone into a foramen. The nerve passes superiorly and penetrates the frontalis around the superior orbital adhesion and runs superiorly in the forehead fat (layer two) to supply the scalp and vertex. The smaller supratrochlear nerve passes up on the medial side of the supraorbital nerve penetrating frontalis similarly to innervate the medial forehead and the infratrochlear nerve supplies skin on the medial eyelid(s), passing above the medial palpebral ligament.10 Frontal branches of the facial nerve transition subcutaneously in the temple to innervate the frontalis segmentally in the subcutaneous plane (layer two).11 Accompanying the nerves, the arteries follow a similar course. The skin of the glabellar and forehead region is mainly supplied by branches from the bilateral supratrochlear, supraorbital and superficial temporal arteries.12 The supreatrochlear artery branches from the ophthalmic artery in the orbit and emerges by piercing the orbital septum above the medial canthal tendon.10 It runs in the vicinity of the procerus and corrugator muscles in the nasal root and the glabellar area, passing subcutaneously in level two on its superior path. The artery has several branches during its course and anastomoses with the supraorbital artery and supratrochlear artery.10 Within the corrugator complex, the artery is vulnerable to injury from needle puncture from toxin needle placement and caution is advised here due to its superficial path. The main artery runs in the glabellar line often just under the subdermis in layer two.12 The supraorbital artery is the larger of the two; it divides into a superficial and deep branch, and the former penetrates the frontalis and enters layer two; then anastomosing with the superficial temporal artery and lacrimal artery. It thus connects the internal and external carotid systems.12 Due to these anastomoses within this layer, the injector must approach layer two with a high degree of caution to reduce potentially irreversible complications. The deep branch runs on the deep surface of the frontalis and runs obliquely laterally – often leaving an indentation on the bone. Occasionally the deep branch will separate in the orbital cavity and enters the forehead through a separate bony canal approximately one cm above the midportion of the orbital rim.13 Deep injections of toxin in this region may spread down this canal and enter the orbital contents, resulting in ptosis.13 The venous return from the face is usually superficial; the supraorbital and supratrochlear veins traverse to the medial canthus where they unite to form the angular vein.14 This becomes the facial vein, which pursues a straight course behind the facial artery, just below the border of the mandible. Blood from the upper lateral forehead is also collected into the tributaries of the superficial temporal vein.14 Layer Three: Frontalis The occipito-frontalis is an exceptionally thin muscle, fusing with the galea aponeurotica from the lateral two thirds of the highest nuchal line of the occipital bone, extending its fine fibres anteriorly to fuse with the procerus muscle at the nasal bone.15 It is part of a group of musculoaponeurotic muscles, which elevate the brow with medial fibres blending inferiorly with the corrugator supercilli and orbicularis oculi muscles blending laterally with orbicularis oculi over the external frontal bone. Aesthetics | July 2015 @aestheticsgroup Aesthetics Journal Aesthetics aestheticsjournal.com The occiptofrontalis muscle represents the third layer in the scalp, which equates to the superficial musculoaponeurotic system (SMAS) layer in the face. Spiegel et al established that superiorly to the nasion, the frontalis fibres are contiguous for a variable distance before an aponeurosis is apparent in the space between the bilateral muscles, which may vary considerably between individuals.16 Male subjects may display a wide variation in the medial muscle border as a ‘W’ shape with a variable attenuation point. Female subjects demonstrate a less irregular central dehiscence shape with a continuous frontalis and ‘V’ shape dehiscence. The dynamic forehead lines may indicate the muscle configuration (see above layer one). These findings are key in analysing the frontalis muscle activity accurately, to treat effectively and administer botulinum toxin judiciously. Appropriate patient selection for botulinum toxin is crucial. Patients with brow ptosis are poor candidates for correction of forehead ryhtides with toxin.1 This needs to be assessed prior to considering treatment. If present, in the authors’ experience, dermal fillers (including skin boosting or intradermal blanching) may provide superior results, and may additionally subtly enhance the position of the brows. Layer Four: Loose Areolar tissue This layer represents a gliding plane – essentially an avascular plane. The frontalis glides over this layer and is a safe plane to place dermal fillers for deep forehead contouring (See below), as an avascular plane does not comprise any vessels or structures to compromise. Layer Five: Periosteum The final layer is anatomically the point where the ligaments that define the forehead arise. Moss et al5 describe the following arrangement of ligamentous attachments in the upper face: the temporal ligamentous adhesion supports the region immediately superior to the eyebrow at the junction of its middle and lateral thirds. Located at the intersection of the temporal, frontal and periorbital regions are the superior temporal septum, the inferior temporal septum and the supraorbital adhesion. The temporal ligament arises from the frontal bone as an expansion at the anterior end of the superior temporal septum, inserting into the Figure 2: XXXXXXXXXXXXXXXX Superior temporal septum Inferior temporal septum CPD Forehead superficial fascia at the junction of the superficial temporal fascia and galea, on the deep surface of the frontalis muscle. The base is located parallel to the arcus marginalis of the orbital rim at a distance of 10mm above it. The superior temporal septum arises from the periosteum along the superior temporal line of the skull and inserts into the line of junction between the superficial temporal fascia and the galea. Anteriorly, this line of junction occurs between the superficial temporal fascia and the galea, lining the deep surface of the lateral border of the frontalis muscle; the expanded end is the temporal ligamentous adhesion. The supraorbital ligamentous adhesion arises from the frontal bone above the orbital rim, extending between the temporal ligament and the origin of the corrugator muscle. The inferior border is located approximately 6mm above the deep attachment of the periorbital septum; the ligament is condensed around the branches of the supra-orbital nerve and corrugator muscle origin. The periorbital septum originates from threequarters of the circumference of the orbital rim, extending from the corrugator origin around to the inferomedial boney origin of the orbicularis oculi. The origin and boundaries of these attachments are significant in terms of re-contouring the forehead with dermal fillers within the supraperiosteal plane; placement with a blunt cannula does not permit dissection of these fixed attachments, thus, product remains safely enclosed within the desired plane and anatomical boundary. (Fig 1) Anaesthesia For optimum patient comfort when re-contouring the forehead, it may be preferable to block the supratrochlear and supraorbital nerves respectively. 3% mepivicaine or 2% lidocaine may utilised for this purpose, with small volumes used to specifically block these nerves low in the supraorbital region.17Lidocaine mixed with the dermal filler may also be used, although the injection technique is slower and may still be uncomfortable for the patient. Topical anaesthesia is insufficient for this advanced deep technique, despite the use of a blunt cannula as the supraorbital nerves innervate the underside of frontalis and periosteum.17 Deep Correction Re-contouring the forehead using a supraperiosteal approach is gaining popularity.13 Redefining this anatomical region provides a youthful contour, and facilitates deep support in counteracting the morphological age-related bone resorbtion noted in both male and female individuals at the glabellar angle.15 Restoring the boney support to the frontal eminence, as well as the lateral brow, achieves a subtle redraping of the overlying tissues and the procedure is popular within certain ethnic populations who strive achieve a rounded, convex appearance to the forehead.3 Facial mapping prior to treatment, along with baseline photography, is key for practitioner and patient to agree on the expected outcome from treatment. Once the full face has been thoroughly cleaned with chlorhexidine and hair tied back, re-contouring may be achieved by commencing an entry point medial to the temporal fusion line, utilizing a 25g needle entry point to the depth of the supraperiosteal plane (layer four). Calcium hydroxylapatite with its highly viscous, elastic and cohesive properties without additional lidocaine Aesthetics | July 2015 29 CPD Forehead @aestheticsgroup A male patient may favour augmentation of the supraciliary arch to enhance a masculine brow in conjunction with the frontal eminence, with threads placed supraperiosteally. provides an ideal product to use in this layer. A 25g cannula is inserted along the supraperiosteal plane to deposit linear threads of product to augment the right and left frontal eminences from the lateral entry points. The volume of product required to achieve the desired result will vary between individuals, depending upon the degree of correction required. A cannula length of 38mm or 50mm is preferable, depending on the dimensions of the frontal bone; within the supraperiosteal plane, the cannula will glide with ease without risk of injury to nerves or vascular compromise. Busso and Howell describe this technique as ‘horse shoe’ placement of product, which achieves a subtle lift across the length of the brow. 3 A male patient may favour augmentation of the supraciliary arch to enhance a masculine brow in conjunction with the frontal eminence, with threads placed supraperiosteally. Following correction, the product is then moulded into the desired contour, and the patient advised to withhold from applying makeup for 48 hours. Loghem et al concur that a cannula approach is preferable, and also advocate an entry point from the temporal crest.18 The ligamentous attachments in the upper face aid in retaining the product supraperiosteally, facilitated further by cannula placement.18 Superficial correction To further enhance the result of the deep correction, it is possible to combine the use of botulinum toxin A to soften dynamic ryhtides across the forehead and glabellar complex. For more established ryhtides, a cohesive, polydensified matrix hyaluronic acid dermal filler may be combined through a ‘blanching’ technique using a 30g needle, described by Micheels et al, who postulate that blanching is not caused by vasoconstriction, but instead by the transparent and transient appearance of the gel in close proximity to the skin’s surface.19 A superficial or intradermal depth may be established by ‘tenting’ the needle to visualise the outline in the skin, with the bevel placed downwards, depositing multiple bead-like punctures, just under the skin until the rhytide has been eliminated. The product is gently massaged following correction, providing exceptional levels of correction for static and/or superficial rhytides. 30 Aesthetics Journal Aesthetics aestheticsjournal.com Conclusion The content of this paper has been compiled to equip the clinician with current evidence and knowledge pertaining to non-surgical forehead re-contouring. The key to successfully and safely treating this region is a current and accurate anatomical knowledge and in particular an understanding of the layered concept in relation to the forehead (SCALP). Anatomy is a dynamic and three dimensional subject; as anatomical awareness develops, it is imperative that practitioners keep abreast of this specialist subject. Didactic and interactive practical teaching courses will enable an in-depth analysis in respect to important facial structures. Once this view is appreciated, it will enable practitioners to develop safe and effective techniques in treating facial zones. Mr Dalvi Humzah is a consultant plastic reconstructive and aesthetic surgeon, with a BSc in Anatomy. He has been a tutor for the Royal College of Surgeons of England and is an examiner for the Intercollegiate MRCS for the Royal College of Surgeons of Glasgow. He is the lead tutor for the award-winning Anatomy teaching programme, Facial Anatomy Teaching, and actively teaches and lectures internationally. Anna Baker is a dermatology and cosmetic nurse practitioner. She runs the nurse-led Medicos Rx Skin Clinic at The Nuffield Health Hospital in Cheltenham, and is the coordinator for Facial Anatomy Teaching. Baker runs nurse-led photodynamic therapy clinics for non-melanoma skin cancer and is currently studying post graduate Applied Clinical Anatomy at Keele University. REFERENCES (NEW) 1. Little A.C., Jones B.C., DeBruine L.M., ‘Facial attractiveness: evolutionary based research’, Trans P., Soc B., 366 (2011), pp. 1638-1659. 2. Dubina M., Tung R., Bolotin D., Mahoney A.M., Tayebi B., Sato M., Mulinari-Brenner F., Jones T., West D.P., Poon E., Nodzenski M., Alam M., ‘Treatment of forehead/glabellar rhytide complex with combination botulinum toxin a and hylaruronic acid versus botulinum toxin A injection alone: a split-face, rater-blinded, randomized control trial’, Journal of Cosmetic Dermatology, 12(4) (2013), pp. 261-6. 3. Busso M., Howel J.D., ‘Forehead Recontouring Using Calcium Hydroxylapatite’, Dermatologic Surgery, 36 (2010), pp. 1910-1913. 4. Smith A.G., Irving’s Anatomy (4th Ed.) (Churchill Livingstone, 1972) 5. Moss J.C., Mendelson B.C., Taylor G.I. ‘Surgical Anatomy of the Ligamentous Attachments in the Temple and Periorbital Regions’, Plastic And Reconstructive Surgery, 105 (4) (2000), pp. 1475-1489. 6. Weider J.M., Moy L.R, ‘Understanding botulinum toxin surgical anatomy of the frown, forehead and periocular region’, Dermatological Surgery, 24 (1998), pp. 1172-1174. 7. Rohrich R.J., Pessa J.E. (2007) The Fat Compartments of the Face: Anatomy and Clinical Implications for Cosmetic Surgery. Plastic And Reconstructive Surgery. 119(7):2219-2227. 8. Guerrerosantos J., Eduardo P.G.C., Arriola J.M., Manzano A.I.V.,Villarian-Munoz B., Benavides L.G., Vazquez M.G., ‘Effectiveness of Botulinum Toxin (Type A) administered by the fixed-site dosing approach versus the muscle area identification’, Aesthetic Plastic Surgery, 39 (2015), pp. 243-251. 9. Gierloff M., Stohring C., Buder T., Gassling V., Acil Y., Wiltfang J., ‘Aging Changes of the Midfacial Fat Compartments: A Computed Tomographic Study’, Plastic And Reconstructive Surgery, 129(1) (2012), pp. 263-273. 10. Sinnatamby C.S. (2006) Lasts Anatomy Regional & Applied. 11th Edition. Churchill Livingstone Elsevier. 11. Agarwal C.A., Mendenhall S.D., Foreman K.B., Owsley J.Q., ‘The Course of the Frontal Branch of the Facial Nerve in Relation to Facial Planes: An Anatomic Study’, Plastic And Reconstructive Surgery, 125(2) (2010), pp. 532-537. 12. Shimizu, Y., Imanishi N., Nakajima T., Nakajima H., Aiso A., Kishi K., ‘Venous Architecture of the Glabellar to the Forehead Region’, Clinical Anatomy, 26(2) (2013), pp. 183-195. 13. Carruthers J.D.A., Fagien S., Rohrich., R.J., Weinkle S., Carruthers A. (2014). Blindness Caused by Cosmetic Filler Injection: A Review of Cause and Therapy. Plast Reconstr Surg 134(6):1197-1201. 14. Imanishi N., Najajima H., Minabe T., Chang H., Aiso S., ‘Venous Drainage Architecture of the Temporal and Parietal Regiosn: Anatomy of the Superficial Temporal Artery and Vein’, Plastic And Reconstructive Surgery, 109(7) (2002), pp. 2197-2203. 15. Lorenc Z.P., Smith S., Nestor M., Moradi A. ‘Understanding the functional anatomy of the frontalis and glabellar complex for optimal aesthetic botulinum toxin type A therapy’, Aesthetic Plastic Surgery, 37(5) (2013), pp. 975-83. 16. Spiegel J.H., Goerig R.C., Lufler R.S., Hoagland T.M., ‘Frontalis midline dehiscence: An anatomical study and discussion of clinical relevance’, Journal of Plastic, Reconstructive & Aesthetic Surgery, 62 (2009), pp. 950-954. 17. Zide B.M., Swift R. (1998). How to block and tackle the face. Plast Reconstr Surg. 101(3):840-51 18. Loghem J., Yutskovskaya Y.A., Werschler W.P., ‘Calcium Hydroxylapatite: Over a Decade of Clinical Experience’, The Journal of Clinical and Aesthetic Dermatology, 8(11) (2015), pp. 38-49. 19. Micheels P., Sarazin D., Besse S., Sundaram H., Flynn T.C. ‘A Blanching Technique for Intradermal Injection of the Hylauronic Acid Belotero’, Plastic And Reconstructive Surgery, 132(4S-2) (2013), pp. 59S-68S. Aesthetics | July 2015