Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
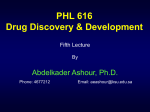
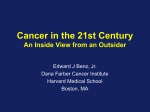
OBSERVATION Neoadjuvant Imatinib Therapy for Dermatofibrosarcoma Protuberans Anne Han, MD; Elbert H. Chen, MD; George Niedt, MD; William Sherman, MD; Désirée Ratner, MD Background: Dermatofibrosarcoma protuberans (DFSP) is an unusual soft-tissue tumor with a propensity for subclinical extension and local recurrence. Surgical excision, even with tissue-sparing techniques, may cause significant deformity or disability because of the infiltrative nature of DFSP. In this study, we evaluate retrospective data obtained from 4 patients with locally advanced or recurrent DFSP who received neoadjuvant imatinib mesylate therapy before undergoing Mohs micrographic surgery. Observations: Patients treated with neoadjuvant imatinib therapy had an average tumor size reduction of D Author Affiliations: Departments of Dermatology (Drs Han, Niedt, and Ratner) and Medicine–Oncology (Dr Sherman), Columbia University Medical Center, New York, New York; and Kaiser Permanente, Rancho Cordova, California (Dr Chen). 36.9%. This clinical response was paralleled by histopathologic changes, including decreased cellularity in 100% of the total area as well as significant hyalinization. Imatinib therapy for DFSP before Mohs micrographic surgery was associated with 100% local control at a maximum follow-up of 4 years. Conclusions: Neoadjuvant imatinib therapy is a welltolerated, novel approach to DFSP that reduces tumor burden and facilitates resection. Larger prospective studies are needed to confirm and expand on these results. Arch Dermatol. 2009;145(7):792-796 ERMATOFIBROSARCOMA protuberans (DFSP) is an indolent soft-tissue tumor that represents approximately 0.1% of all malignant neoplasms.1 It occurs most often on the trunk and extremities and less frequently on the head and neck. It appears as indurated, flesh-colored or erythematous, ill-defined plaques, within which nodules may arise. Microscopically, the tumor often extends far beyond clinically apparent margins, infiltrating by local extension through the dermis, subcutaneous tissue, fascia, and even muscle. It has a high rate of local recurrence (13%-60%)2-5 but rarely metastasizes.6 Excision using Mohs micrographic surgery (MMS) is the standard of therapy for DFSP.7-9 However, given the potential subclinical involvement that characterizes DFSP, resection may still be difficult and associated with significant deformity or disability. In surgically challenging cases, neoadjuvant treatment with imatinib mesylate may reduce tumor bulk, decrease local extension, and improve overall outcome, allowing excisional margins to be reduced without sacrificing surgical cure. Imatinib is a small molecular adenosine triphosphate analogue that competitively inhibits the adenosine triphosphate– binding site of the platelet-derived growth ARCH DERMATOL/ VOL 145 (NO. 7), JULY 2009 792 factor  (PDGF) receptor tyrosine kinase in DFSP. The tumors of DFSP have a pathologic chromosomal rearrangement that fuses the COL1A1 promoter gene of chromosome 17 to the PDGFβ gene of chromosome 22. Overactivation of PDGF receptor tyrosine kinase leads to cellular proliferation and tumor formation. When imatinib binds at the receptor site, kinase activity downregulates, resulting in growth inhibition and increased apoptosis.10-17 Imatinib has been used successfully to treat unresectable and metastatic lesions as well as locally advanced primary and recurrent DFSP.1,6,18,19 This study adds to a growing body of literature showing that the use of imatinib can reduce the tumor burden of DFSP. METHODS Between 2004 and 2007, patients with a biopsy-confirmed diagnosis of DFSP who were referred for MMS at Columbia University Medical Center, New York, New York, were evaluated to determine whether they were appropriate candidates for imatinib treatment. Patients who were offered neoadjuvant imatinib therapy had tumors that appeared to be at a clinically significant risk of functional or aesthetic compromise after surgery. Because we decided to perform this review subsequent to the treatment of these patients, they were not WWW.ARCHDERMATOL.COM ©2009 American Medical Association. All rights reserved. (REPRINTED WITH CORRECTIONS) Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/derm/5211/ on 05/14/2017 Table. Tumor Characteristics and Imatinib Mesylate Treatment Regimens in 4 Cases of Dermatofibrosarcoma Protuberans Variable Tumor size, cm Tumor site Primary or recurrent Daily dosage, mg Duration, mo Initial lesion, cm Size of lesion after imatinib therapy, cm Reduction in size of lesion, % a Depth Patient 1 Patient 2 Patient 3 Patient 4 7.3 ⫻6.5 Left frontal scalp Recurrent 800 3 7.3 ⫻6.5 7.0 ⫻5.5 18.9 Periosteum 2.7⫻ 2.0 Left medial ankle Primary 400 3.5 2.7⫻ 2.0 1.7⫻ 1.2 45.3 Fascia 14.0⫻ 8.6 Left lower abdominal wall Recurrent 800 7 14.0⫻ 8.6 15.4⫻ 3.0 61.6 Fascia 4.0⫻3.2 Left thigh Primary 600 3 4.0⫻3.2 4.0⫻2.5 21.9 Fascia a The percentage of reduction in lesion size after imatinib therapy is calculated as follows: [(XY –XY )/XY ] ⫻ 100%, where IL is the initial lesion and PL is the IL PL IL lesion after imatinib therapy. subject to rigid inclusion or exclusion criteria. Institutional review board approval was obtained to evaluate their records retrospectively. Informed consent was not required. Only records authorized for research use were used. The drug was prescribed by a medical oncologist (W.S.) who monitored all patients’ clinical responses, tolerance, and adverse effects. The standard dose was 800 mg/d based on the observation that PDGF tumors require a higher dose for inhibition than the 400-mg standard dose for BCR-ABL tumors. Doses lower than 800 mg were given at the discretion of the medical oncologist. The length of treatment was determined by clinical response. Treatment was administered until the decrease in tumor size had stabilized or was minimal and continued until 4 weeks before surgery. The cost of the medication, which is usually several thousand dollars per month, was covered by insurance after a letter was submitted that justified the prescription of imatinib. The Mohs surgeon used a ruler to measure the extent of visible and palpable tumor in the X and Y dimensions. The sizes of the lesions were noted at the time of consultation and preoperatively on the day of surgery. Preoperative biopsy specimens obtained to confirm the diagnosis of DFSP were compared with debulking specimens obtained at the time of MMS. These specimens were used to compare the histologic features on hematoxylin-eosin–stained sections before and after imatinib therapy. RESULTS A total of 4 patients with DFSP were referred from the dermatologic surgery unit at Columbia University Medical Center to receive neoadjuvant imatinib therapy before MMS. The Table compares the tumor characteristics, treatment regimens, and percentage of tumor reduction in the 4 patients who were treated with imatinib before surgery. The lesions, which were located on the scalp, abdomen, thigh, and ankle, ranged from 2.0 to 8.6 cm in the X dimension and from 2.7 to 14.0 cm in the Y dimension. Of the 4 imatinib-treated patients, 2 had recurrent lesions and 2 had locally advanced primary DFSP. The median duration of treatment with imatinib was 3 months. The drug was administered at a dosage of 800 mg/d in 2 patients and at lower dosages in 2 patients. One patient requested a dose of 400 mg once a day because she was hesitant to take a new medication. Given the other patient’s history of multiple comorbidities, which included hypertension, diabetes, and obesity, the medical oncologist adjusted the initial dose to 600 mg/d to monitor for adverse events, with the goal of Figure 1. Specimen from the center of the tumor showing spindle cells in a storiform pattern typical of dermatofibrosarcoma protuberans (hematoxylin-eosin, original magnification ⫻20). gradually increasing to the target dose if tolerated. All 4 patients tolerated their starting doses and showed a clinical response. As a result, no further dosage changes were made during the remainder of the treatment periods. Three patients were treated for 3 to 31⁄2 months and experienced initial adverse effects consisting of fatigue, nausea, headache, dizziness, and diarrhea, which resolved within several weeks. The remaining patient was treated for 7 months and complained of dry skin and flank pain during the treatment. Despite these adverse effects, all patients tolerated the drug without requiring dose reduction or discontinuation. All 4 patients responded to imatinib therapy with a reduction in tumor size and thickness, achieving a reduction in preoperative tumor size, measured in the X and Y dimensions, between 18.9% and 61.6%, with an average size reduction of 36.9%. On pretreatment histopathologic examination, all lesions exhibited spindle-shaped cells in a typical storiform pattern. After treatment with imatinib, the histopathologic area showing decreased cellularity approached 100%. Also, there was production of hyalinized material throughout the tumors (Figure 1 and Figure 2). Clear margins were achieved with MMS in 3 of the 4 patients. The fourth patient had a large, multiply recurrent, abdominal lesion that, after preoperative debulking, required 1 stage of MMS with a margin of 2 cm to ARCH DERMATOL/ VOL 145 (NO. 7), JULY 2009 793 WWW.ARCHDERMATOL.COM ©2009 American Medical Association. All rights reserved. (REPRINTED WITH CORRECTIONS) Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/derm/5211/ on 05/14/2017 Figure 2. Specimen from the center of the tumor showing decreased cellularity in 100% of the total area as well as significant hyalinization after imatinib mesylate therapy (hematoxylin-eosin, original magnification ⫻20). Figure 3. Lesion on the scalp of patient 1 before imatinib mesylate therapy. clear its peripheral extent. The patient subsequently underwent further resection by surgical oncology. At the time of writing, all patients were free of disease, with follow-up ranging from 1.5 to 4.0 years. COMMENT While MMS and other surgery with complete peripheral and deep margin control are standard therapies for DFSP, neoadjuvant treatment with imatinib can offer considerable advantages. It is striking to note that imatinibtreated patients had an average 36.9% reduction in preoperative tumor size (Figure 3 and Figure 4). Therefore, neoadjuvant imatinib therapy has the potential to facilitate excision of large or difficult tumors. For example, the smallest pretreatment lesion in this case series was a 3-cm, freely movable, exophytic nodule on the medial aspect of the ankle. A complicated surgical course was anticipated owing to the proximity of tendons, muscles, and nerves lying below the lesion. Neoadjuvant treatment with imatinib significantly reduced the preoperative lesion size, resulting in a less extensive surgical defect, and allowed placement of a full-thickness skin graft over a wound that extended to the periosteum. As a re- Figure 4. Lesion on the scalp of patient 1 after imatinib mesylate therapy. Note the reduction in the size and thickness of the tumor at its surface. sult, the patient did not suffer the potential comorbidity of functional damage to her ankle as a result of surgery. Imatinib therapy is also useful in patients with recurrent DFSP. One of the study patients who had a large anterior abdominal wall lesion had previously undergone 2 incomplete resections. He responded well to adjuvant treatment with imatinib but adhered to the regimen for only 4 months. Six years later, the lesion had progressed to a fungating, foul-smelling mass that measured at least 10 cm at the base, with smaller nodules noted at its periphery. After a 7-month neoadjuvant course of imatinib, the size of the mass had decreased to less than 7 cm at the base and the nodules had also decreased in size. The patient then underwent palliative debulking by surgical oncology before MMS both to control bleeding and to minimize the risk of infection. On the day of surgery, 1 surgical stage was taken for peripheral margin clearance; the remaining resection was performed by surgical oncology the next day with the patient under general anesthesia. The resulting defect extended to the fascia, with residual tumor at the deep margin. The wound was left open until clear margins were confirmed. An additional Mohs surgical stage was required after a positive deep margin was discovered extending toward the scrotum. As a result of the combined effort, complete resection with clear margins was ultimately achieved. The clinical response of DFSP to imatinib therapy is paralleled by the changes seen histopathologically. Biopsy specimens of DFSPs from imatinib-treated patients showed a decrease in cellularity in 100% of the total area as well as significant hyalinization. These observations correlate with a recently published novel histologic finding in DFSP after treatment with imatinib: that of copious amounts of hyalinized collagen.20 A potential pitfall of neoadjuvant treatment with imatinib is the possibility that imatinib exerts its effect in a discontiguous fashion, resulting in skip areas of histologically normal tissue interspersed with persistent tumor. Such an effect would make MMS less reliable in achieving true tumorfree margins and could lead to more recurrences. To our knowledge, no such findings have been reported in the literature to date, and we have not seen any evidence of skip areas after imatinib therapy in patients with DFSP ARCH DERMATOL/ VOL 145 (NO. 7), JULY 2009 794 WWW.ARCHDERMATOL.COM ©2009 American Medical Association. All rights reserved. (REPRINTED WITH CORRECTIONS) Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/derm/5211/ on 05/14/2017 at our institution. In our series, the positive margin occurred in the patient who had a multiply recurrent tumor, and that margin was contiguous with a deep pocket of tumor. Imatinib appears to be a safe oral medication with the ability to significantly shrink the lesions of DFSP. Among our patients, adverse effects, including fatigue, nausea, headache, dizziness, diarrhea, dry skin, and flank pain, were minimal, and all of them resolved. The mean decrease in size of our patients’ tumors after imatinib pretreatment was 36.9%. All study patients were confirmed to be tumor-free after a follow-up of 1.5 to 4.0 years. To our knowledge, there are no known long-term effects of imatinib therapy, although it should be noted that it is still a relatively new drug, having been first approved for use in 2001 for chronic myeloid leukemia.21 Imatinib has been reported to be efficacious only in tumors exhibiting the chromosomal translocation (17;22), which occurs in 90% of all DFSP lesions.22,23 While the patients in our study did not receive pretreatment evaluation by fluorescence in situ hybridization, routine screening with fluorescence in situ hybridization before imatinib therapy may be useful in identifying this rearrangement, so that patients with DFSP without this translocation will not be pretreated unnecessarily. In the future, adjuvant use of imatinib could also be considered in patients with DFSP who have undergone an incomplete surgical excision and therefore have a high probability of recurrence. Several reports already document a partial or complete response to imatinib in cases of metastatic, recurrent, and locally advanced disease. Five groups have described a total of 7 patients with metastatic DFSP, 5 of whom had partial or complete remission.6,18,24-26 The 2 patients with metastatic DFSP who did not to respond to imatinib therapy were found to be without r(17;22) or t(17;22) chromosomal rearrangements. One imatinib-treated case of recurrent DFSP achieved a good response,22 and a total of 11 patients with locally advanced primary DFSP also had some degree of success.1,19,27,28 Our study documents the utility of imatinib therapy in decreasing tumor size before surgery in 2 locally advanced and 2 recurrent cases of DFSP and shows that imatinib therapy has the potential to transform patients with surgically challenging or recurrent tumors into better operative candidates. However, there are several limitations to our study, including its retrospective design, small sample size, and short-term follow-up. Larger prospective studies are needed to confirm and expand on our results. Furthermore, tumor bulk, or the extent of invasion, is notoriously difficult to assess in DFSP. Tumors can behave differently, even at the same anatomical location; therefore, the surface area may not be indicative of the total tumor volume. Currently, several phase 2 clinical trials are under way to assess the response of DFSP to varying durations of imatinib treatment. Preoperative imatinib therapy may provide a means of decreasing morbidity and recurrence rates for patients with locally aggressive or recurrent cases of DFSP that are surgically challenging but still respectable. While imatinib is currently approved only for treatment of nonsurgical adult candidates with unresectable, recurrent, and/or metastatic DFSP, studies like this one may help to expand the Food and Drug Administration’s indications for its use. In conclusion, neoadjuvant treatment of locally advanced and recurrent DFSP with imatinib improves surgical outcomes and may facilitate resection of difficult tumors. Oral imatinib therapy is a well-tolerated, novel approach to the treatment of DFSP that does not appear to have any long-term sequelae. It offers patients with DFSP with highly infiltrative lesions the possibility of reducing their tumor size before surgery, thereby resulting in a smaller postsurgical defect and a less complicated repair. Accepted for Publication: January 6, 2009. Correspondence: Anne Han, MD, Department of Dermatology, Columbia University Medical Center, 161 Fort Washington Ave, 12th Floor, New York, NY 10032 (dr [email protected]). Author Contributions: All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Han, Chen, Niedt, and Ratner. Acquisition of data: Han, Chen, Niedt, Sherman, and Ratner. Analysis and interpretation of data: Han, Chen, Niedt, and Ratner. Drafting of the manuscript: Han and Niedt. Critical revision of the manuscript for important intellectual content: Han, Chen, Niedt, Sherman, and Ratner. Administrative, technical, and material support: Han, Chen, Niedt, and Sherman. Study supervision: Ratner. Financial Disclosure: None reported. Additional Contributions: Spiros Manolidis, MD, and Bret Taback, MD, generously offered their expertise and support in the treatment of these patients. REFERENCES 1. Mehrany K, Swanson NA, Heinrich MC, et al. Dermatofibrosarcoma protuberans: a partial response to imatinib therapy. Dermatol Surg. 2006;32(3):456459. 2. Gloster HM Jr. Dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1996; 35(3, pt 1):355-374, quiz 375-376. 3. Mark RJ, Bailet JW, Tran LM, Poen J, Fu YS, Calcaterra TC. Dermatofibrosarcoma protuberans of the head and neck: a report of 16 cases. Arch Otolaryngol Head Neck Surg. 1993;119(8):891-896. 4. Rutgers EJ, Kroon BB, Albus-Lutter CE, Gortzak E. Dermatofibrosarcoma protuberans: treatment and prognosis. Eur J Surg Oncol. 1992;18(3):241-248. 5. Bowne WB, Antonescu CR, Leung DH, et al. Dermatofibrosarcoma protuberans: a clinicopathologic analysis of patients treated and followed at a single institution. Cancer. 2000;88(12):2711-2720. 6. Labropoulos SV, Fletcher JA, Oliveira AM, Papadopoulos S, Razis ED. Sustained complete remission of metastatic dermatofibrosarcoma protuberans with imatinib mesylate. Anticancer Drugs. 2005;16(4):461-466. 7. Ratner D, Thomas CO, Johnson TM, et al. Mohs micrographic surgery for the treatment of dermatofibrosarcoma protuberans: results of a multi-institutional series with an analysis of the extent of microscopic spread. J Am Acad Dermatol. 1997;37(4):600-613. 8. Gloster HM Jr, Harris KR, Roenigk RK. A comparison between Mohs micrographic surgery and wide surgical excision for the treatment of dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1996;35(1):82-87. 9. Snow SN, Gordon EM, Larson PO, Bagheri MM, Bentz ML, Sable DB. Dermatofibrosarcoma protuberans: a report on 29 patients treated by Mohs micrographic surgery with long-term follow-up and review of the literature. Cancer. 2004;101(1):28-38. 10. Sawyers CL. Imatinib GIST keeps finding new indications: successful treatment of dermatofibrosarcoma protuberans by targeted inhibition of the plateletderived growth factor receptor. J Clin Oncol. 2002;20(17):3568-3569. ARCH DERMATOL/ VOL 145 (NO. 7), JULY 2009 795 WWW.ARCHDERMATOL.COM ©2009 American Medical Association. All rights reserved. (REPRINTED WITH CORRECTIONS) Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/derm/5211/ on 05/14/2017 11. McArthur GA. Dermatofibrosarcoma protuberans: a surgical disease with a molecular savior. Curr Opin Oncol. 2006;18(4):341-346. 12. Greco A, Roccato E, Miranda C, Cleris L, Formelli F, Pierotti MA. Growthinhibitory effect of STI571 on cells transformed by the COL1A1/PDGFB rearrangement. Int J Cancer. 2001;92(3):354-360. 13. Sjöblom T, Shimizu A, O’Brien KP, et al. Growth inhibition of dermatofibrosarcoma protuberans tumors by the platelet-derived growth factor receptor antagonist STI571 through induction of apoptosis. Cancer Res. 2001;61(15):57785783. 14. Shimizu A, O’Brien KP, Sjöblom T, et al. The dermatofibrosarcoma protuberans– associated collagen type Ialpha1/platelet-derived growth factor (PDGF) B-chain fusion gene generates a transforming protein that is processed to functional PDGF-BB. Cancer Res. 1999;59(15):3719-3723. 15. Abrams TA, Schuetze SM. Targeted therapy for dermatofibrosarcoma protuberans. Curr Oncol Rep. 2006;8(4):291-296. 16. McArthur G. Molecularly targeted treatment for dermatofibrosarcoma protuberans. Semin Oncol. 2004;31(2)(suppl 6):30-36. 17. McArthur GA. Molecular targeting of dermatofibrosarcoma protuberans: a new approach to a surgical disease. J Natl Compr Canc Netw. 2007;5(5):557-562. 18. Mizutani K, Tamada Y, Hara K, et al. Imatinib mesylate inhibits the growth of metastatic lung lesions in a patient with dermatofibrosarcoma protuberans. Br J Dermatol. 2004;151(1):235-237. 19. Price VE, Fletcher JA, Zielenska M, et al. Imatinib mesylate: an attractive alternative in young children with large, surgically challenging dermatofibrosarcoma protuberans. Pediatr Blood Cancer. 2005;44(5):511-515. 20. Thomison J, McCarter M, McClain D, Golitz LE, Goldenberg G. Hyalinized colla- 21. 22. 23. 24. 25. 26. 27. 28. gen in a dermatofibrosarcoma protuberans after treatment with imatinib mesylate. J Cutan Pathol. 2008;35(11):1003-1006. Gleevec (imatinib mesylate). Food and Drug Administration Web site. http://www .fda.gov/cder/drug/infopage/gleevec/default.htm. Accessed April 10, 2007. Wright TI, Petersen JE. Treatment of recurrent dermatofibrosarcoma protuberans with imatinib mesylate, followed by Mohs micrographic surgery. Dermatol Surg. 2007;33(6):741-744. Sandberg AA, Bridge JA. Updates on the cytogenetics and molecular genetics of bone and soft-tissue tumors: dermatofibrosarcoma protuberans and giant cell fibroblastoma. Cancer Genet Cytogenet. 2003;140(1):1-12. Kasper B, Lossignol D, Gil T, Flamen P, De Saint Aubain N, Awada A. Imatinib mesylate in a patient with metastatic disease originating from a dermatofibrosarcoma protuberans of the scalp. Anticancer Drugs. 2006;17(10):1223-1225. Maki RG, Awan RA, Dixon RH, Jhanwar S, Antonescu CR. Differential sensitivity to imatinib of 2 patients with metastatic sarcoma arising from dermatofibrosarcoma protuberans. Int J Cancer. 2002;100(6):623-626. Rubin BP, Schuetze SM, Eary JF, et al. Molecular targeting of platelet-derived growth factor B by imatinib mesylate in a patient with metastatic dermatofibrosarcoma protuberans. J Clin Oncol. 2002;20(17):3586-3591. McArthur GA, Demetri GD, van Oosterom A, et al. Molecular and clinical analysis of locally advanced dermatofibrosarcoma protuberans treated with imatinib: Imatinib Target Exploration Consortium Study B2225. J Clin Oncol. 2005;23 (4):866-873. Savoia P, Ortoncelli M, Quaglino P, Bernengo MG. Imatinib mesylate in the treatment of a large unresectable dermatofibrosarcoma protuberans: a case study. Dermatol Surg. 2006;32(8):1097-1102. Announcement Volunteering With Health Volunteers Overseas The American Academy of Dermatology partnered with Health Volunteers Overseas (HVO) in 2004 to match interested dermatologists with overseas volunteer opportunities. Through HVO programs, volunteer dermatologists train local health care providers, giving them the knowledge and skills to make a difference in their own communities. The major goal of the HVO dermatology programs is to build capacity through training local health care providers (ranging from dermatology residents to primary care health workers) in clinical dermatology. Sites with volunteer opportunities for dermatologists include Costa Rica, Palau, India, Peru, Uganda, Cambodia, and Saint Lucia. Volunteers generally serve for 2 to 4 weeks, although shorter and longer assignments are possible. A private, nonprofit membership organization, HVO was founded in 1986 to improve global health through education. HVO designs and implements clinical education programs across the spectrum of health specialties. To learn more about volunteering with HVO, visit the Web site (www.hvousa.org) or contact the HVO Program Department at (202) 296-0928. ARCH DERMATOL/ VOL 145 (NO. 7), JULY 2009 796 WWW.ARCHDERMATOL.COM ©2009 American Medical Association. All rights reserved. (REPRINTED WITH CORRECTIONS) Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/derm/5211/ on 05/14/2017