Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
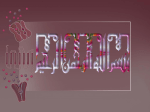
Anaesthesia in myasthenia Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics, PhD (physio) Mahatma Gandhi Medical college and research institute , puducherry India What is myasthenia gravis • MG is an autoimmune disorder – • circulating antibodies to nicotinic acetylcholine receptors at the neuromuscular junction • antibodies reduce the numbers of receptors • Symptoms if only 30% receptors are present reUp to 25% of patients have a concurrent thymoma, • About 10% have evidence for other autoimmune diseases ors reduced to 30% of normal Clinical features • muscle weakness -an overall fatigability increases with exertion over the course of the day. 14:100,000 age 10 and 40. (bimodal ) Females are more frequently affected • diplopia and ptosis resulting from weakness of the ocular muscles. • slowly spread to bulbar muscles, which may lead to aspiration and respiratory failure, and later affect the proximal extremities Osserman and Genkins • class I (ocular muscles only); • class II (eye symptoms plus mild generalize weakness); • class III (eye plus moderate weakness); • class IV (eye plus severe weakness); • class V (intubation, ventilation) How to diagnose ? • blood tests for antibodies; • electromyographic recordings; • electrophysiologic evaluation is often performed and shows a classic decrement in the compound muscle action potential after repetitive nerve stimulation. cholinesterase inhibitor test (edrophonium test); • Tensilon test anticholinesterase, (administration e.g., of an edrophonium). Improvement is usually seen within 5 minutes after administration of the drug and lasts for about 10 minutes • Imaging (to identify thymoma). • • • • Drugs aggravate Neuromuscular weakness Penicillamine Nondepolarizing muscle relaxants Aminoglycosides Procainamide Some other DD s of myasthenia • • • • Graves' disease Eaton lambert syndrome Cranial nerve palsies Congenital myasthenic syndromes Other autoimmune diseases coexisting • hyperthyroidism is present in approximately 10% of patients with myasthenia gravis. • Rheumatoid arthritis, SLE, and pernicious anemia occur more commonly in MG Treatment • Two problems • I. muscle weakness • Cholinesterase inhibitors (neostigmine, • Pyridostigmine • (maximal dose )120 mg every 3 hours) Problem 2. immunosupression • corticosteroids and • immunosuppressive drugs (cyclosporine, azathioprine) • Plasmapheresis-(four to eight treatments over 2 weeks • thymectomy is performed if general symptoms are present Anaesthetic challenges Preop evaluation • preoperative interview that they may be intubated and ventilated when they awaken • All routine investigations • ECG -- Cardiac arrhythmias and myocarditis Preop preparation • pyridostigmine • • • • • • • ↓ Bad response ↓ good response Young old ↓ ↓ Steroids steroids + azathioprine ↓ ↓ Imp. Not imp imp.→taper steroids →thy ↓ ↓ Thy add plasma Preop preparation • Only plasmapheresis Preop • Lung function testing • Respiratory and bulbar functions should be carefully evaluated during the preoperative evaluation • Preop neurologist evaluation • Preoperative plasmapheresis Post op ventilation ?? Four Factors disease duration of longer than 6 years, chronic obstructive pulmonary disease(COPD) unrelated to myasthenia gravis, • a daily dose of pyridostigmine higher than 750 mg, • and a vital capacity less than 2.9 L. Premed • Anticholinesterase to continue ?? • Small dose benzodiazepine • Anticholinergics Anaesthetics-Nondepolarizing Neuromuscular Blockers • Long acting NDNMB (pancuronium, pipecuronium, doxacuronium) :avoided • Intermediate and short acting: used with careful monitoring.. Depolarizers nondepolarizers Succinylcholine • resistance to depolarizing agents.( ED95 : 2.6 times of control) • because of the decreased number of functional acetylcholine receptors • more likely to develop phase II block • decrease in cholinesterase activity achieved by anticholinesterase treatment So regarding relaxants • NDP s more sensitive • Depolarizers more resistant Inhaled Anaesthetics • Isoflurane , enflurane: decrease TOF responses • Sevoflurane at 2.5% depresses EMG responses • effects of desflurane in MG ?? Intravenous Anaesthetic Agents • Propofol √ • -- no effect on NMJ • Etomidate, althesin and ketamine : Reports of uneventful anesthesia. • Opioids – do not appear to depress NM transmission in MG muscle. – Central respiratory depression may be a problem Anaesthesia -1 • • • • • • IV induction + inh. Drugs + intubation Maintain on N2O ,O2, Inh. Agent No NonDepolarizers Extubate without reversal Anaesthesia - 2 • • • • • Propofol Scoline N2O ,O2, Inh. Agent Nondepolarizers (10% dose with NMJ monitor) unsuccessful extubation, longer postoperative mechanical ventilation and hospital stay • Suggamadex or post op ventilation Regional Anesthesia • Ester anesthetics, metabolized by cholinesterase, may present particular problems in patients taking anticholinesterases. • Use reduced doses of amide (lidocaine, bupivacaine) to avoid high blood levels. • Remember drugs and coexisting diseases Anaesthesia 3, 4 • TIVA for the management of myasthenics has been reported. • Local anaesthesia is successful Postoperative considerations • • • • • Weakness Pain (local ,epidural opioids ) Myasthenic crisis Cholinergic crisis Resume the anticholinergic therapy as soon as possible after surgery. The postop requirements may be different from the routine preoperative dose and • careful titration because the IV dose is only about 1/30 to 1/120 Post op problems • Nerve stimulator - bulbar Vs limb muscles • Inspiratory force of > - 25 cm is OK • Trans sternal thymectomy – 50 % req. ventilation • Trans cervical thymectomy OR • video-assisted thorascopic (VATS)– • less post op ventilation ,remission more ?? • Early thymectomy better !! Your icu ready Myasthenic crisis • Myasthenic crisis is a life-threatening condition, which is defined as weakness from acquired myasthenia gravis (MG) that is severe enough to necessitate intubation precipitants • • • • infection. Surgery Pregnancy, certain antibiotics (aminoglycosides, erythromycin and azithromycin), cardiac drugs (beta-blockers, procainamide, and quinidine), and magnesium. • TREAT VIGOROUS WITH POSSIBLE OPTIONS Cholinergic crisis • excess of cholinesterase inhibitors (ie, neostigmine, pyridostigmine, physostigmine) • resembles organophosphate poisoning. • excessive ACh stimulation of striated muscle at nicotinic junctions produces flaccid muscle paralysis that is clinically indistinguishable from weakness due to MG. Cholinergic crisis • Miosis and the SLUDGE syndrome (ie, salivation, lacrimation, urinary incontinence, diarrhea, GI upset and hypermotility, emesis) also may mark cholinergic crisis. • Despite muscle weakness, deep tendon reflexes are preserved. Cholinergic crisis • When muscarinic effects are obvious , diagnosis is easily made. Antimuscarinics and respiratory support are given • EDROPHONIUM TEST WILL DIFFERENTIATE BOTH CRISES Myasthenia and pregnancy • Exacerbations of myasthenia must be anticipated during pregnancy • Epidural analgesia and anaesthesia can be used for labour and delivery • Muscle relaxation induced by regional anaesthesia may compound the weakness caused by myasthenia. Myasthenic syndrome • Acq. Disorder • Small cell ca of lungs • IgG antibodies to pre synaptic voltage dep. Calcium channels • Abn. Vesicular release • Exercise improves • Diaminopyridine improves • Sensitive to both DPs and NDPs • anticholinesterase agent - not dependable SUMMARY • Preop bulbar? Anticholinestrase , plasmapheresis , premed atropine • GA with propofol, inh. agents ,no NDPs • Post op ventilation • Or GA, relaxants, suggamadex, ventilation • Other surgeries – possible RA, LA • Post op epidural opioids, muscle weakness Thank you all