Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
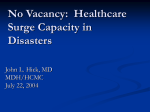
x Guidelines for Managing Inpatient and Outpatient Surge Capacity Recommendations of the State Expert Panel on Inpatient and Outpatient Surge Capacity November 2005 Table of Contents Introduction ……………………………………………………………………….Intro -1 1. Types of Incidents ……………………………………………………………Page 1-1 2. Increasing Availability of Existing Inpatient Beds …………………………Page 2 -1 3. Field Triage …………………………………………………………………….Page 3-1 4. Opening/Creating Areas or Wings for Inpatient Surge Capacity ………………Page 4-1 Classification of Surge Capacity Beds by Triage Colors ……………..…….Page 4-2 Application of Color-Coded Surge Beds to the Level of Incident……..........Page 4-3 Example of Surge Capacity Matrix ………………...……………………… Page 4-4 Surge Capacity Matrix …………………………….………………………Page 4-5 Cohorting Surge Patients …………………………………………………. Page 4-6 Summary of Surge Capacity Beds …………………………..…………… Page 4-7 St. Camillus Hospital Surge Capacity Support Area Matrix …………… Page 4-8 5. Inpatient Units for Special Considerations …………………………………...Page 5-1 6. Criteria for an Inpatient Surge Capacity Bed ………………………………… Page 6-1 7. State Stockpile of Inpatient Surge Capacity Beds …………………………… Page 7-1 8. Patient Care Staffing for Inpatient Surge Capacity Areas ……………………. Page 8-1 Staffing Strategies………………………………………………………… Page 8-1 Assignment of Staff to Color-Coded Beds ………………………………..Page 8-2 Job Action Sheets ………………………………………………………… Page 8-3 Managing the Continuum of Care After the Initial Surge of Inpatients …Page 8-3 Transition Matrix …………………………………………………………Page 8-4 Secondary Surge …………………………………………………………. Page 8-4 Discharge Planning and Case Management …………………….. Page 8 -5 9. Ancillary Care Staffing for Inpatient Surge Capacity Areas ……………Page 9 -1 Anci l l a r y S uppo rt Mat ri x …………… …………………… … … P a ge 9 -2 10. Staff Support Considerations ………………………………………………. Page 10-1 11. Equipment and Supplies …………………………………………………….. Page 11-1 Equipment Location Matrix ……………………………………………… Page 11-2 Equipment Source Matrix ……………………………………………… Page 11-2 Critical Supply Inventory ………………………………………………. Page 11-3 Supply Source Matrix …………………………………………………… Page 11-5 12. Triage Center …………………………………………………………………. Page 12-1 Criteria for Triage Center ………………………………………………. Page 12-1 Decontamination ………………………………………………………… Page 12-1 13. Outpatient Surge Capacity …………………………………………………… Page 13-1 Alternative Treatment Site Matrix ……………………………………….. Page 13-2 14. Exercise ………………………………………………………………………. Page 14-1 15. Off-Site Alternative Inpatient Treatment Centers ……………………………. Page 15-1 16. Risk Communications ……………………………………………………… Page 16-1 17. Business Continuity Plan …………………………………………………… Page 17-1 18. Guidelines for Completing Your Hospital Surge Capacity Plan ……………. Page 18-1 Appendices Appendix A: Map of HRSA Hospital Disaster Preparedness Regions …………Appendix A-1 Appendix B: START Triage Algorithm …………………………………………Appendix B-1 Appendix C: JumpSTART Triage Algorithm …………………………………Appendix C-1 Appendix D: Example of Hospital Surge Capacity ………………………….. Appendix D-1 Appendix E: Prioritization of Patient Care Tasks ……………………………. Appendix E-1 Appendix F: Job Action Sheets ………………………………………………..Appendix F-1 Appendix G: Medications in ChemPacks …………………………………….Appendix G-1 Appendix H: Accessing the ChemPacks ………………………………………Appendix H-1 Appendix I: Rationing Supplies …………………………………………………Appendix I-1 Appendix J: Access to Personal Protective Equipment ………………………….Appendix J-1 Appendix K: Strategic National Stockpile List of Assets ……………………….Appendix K-1 Appendix L: Template Memorandum of Understanding ………………………Appendix L-1 Worksheets Worksheet 1: Incident Level Matrix ……………………………………………Worksheet 1-1 Worksheet 2: Surge Capacity Matrix …………………………………………..Worksheet 2-1 Worksheet 3: Surge Capacity Summary ………………………………………..Worksheet 3-1 Worksheet 4: Surge Support Area Matrix ………………………………………Worksheet 4-1 Worksheet 5: Staffing Ratios for Surge Capacity Matrix …………………….Worksheet 5-1 Worksheet 6: Transition Matrix ……………………………………………….Worksheet 6-1 Worksheet 7: Ancillary Support Matrix ……………………………………….Worksheet 7-1 Worksheet 8: Equipment Location Matrix ……………………………………..Worksheet 8-1 Worksheet 9: Equipment Source Matrix ………………………………………..Worksheet 9-1 Worksheet 10: Critical Supply Inventory Matrix…………………………….Worksheet 10-1 Worksheet 11: Critical Supply Source Matrix ……………………………….Worksheet 11-1 Worksheet 12: Alternative Treatment Site Matrix ……………………………Worksheet 12-1 Introduction This document provides guidelines and recommendations for hospitals to manage a surge of inpatients and outpatients in a mass casualty incident. The National Bioterrorism Hospital Preparedness Program of the Health Resources and Services Administration (HRSA) has granted funds to help hospitals better manage a surge of inpatients, based on a minimum capability of hospitals being able to treat 500 adult and pediatric patients per 1,000,000 population. For the State of Wisconsin this translates to being able to care for a minimum surge of 2,683 additional inpatients. Presently, there are 12,922 staffed beds for the 128 medical/surgical hospitals in the state. Initially, it was felt that surge capacity could be achieved by establishing Alternative Treatment Facilities, that is, other sites, apart from the hospital, such as community centers, schools and other such large buildings that could be converted into use as inpatient facilities. The many logistical, clinical, legal and financial issues involved with the implementation of the Alternative Treatment Centers are myriad. 128 hospitals participated in an exercise in May 2004 to measure their ability to increase inpatient bed capacity. The results of the exercise demonstrated that: Hospitals were able to “empty” existing beds by early discharge and other strategies so that there were approximately 7,000 available inpatient beds1 Hospitals were able to open and/or convert other areas or wings of their facilities to care for inpatients so that there were approximately 17,700 additional inpatient beds available2 The State Expert Panel on Inpatient and Outpatient Surge Capacity was convened to make recommendations, based on the surge capacity goals, presented to hospitals by HRSA, and the options that are available to hospitals to achieve this goal. This Panel was composed of Inpatient Nursing and Emergency Department managers. These Guidelines then are based on the results of the May 2004 exercise and the recommendations of the Expert Panel. The strategy recommended for Wisconsin hospitals is to both “empty” existing inpatient beds to the extent possible (to deal with the initial surge of inpatients) and to open other areas for inpatient care. Based on the results of the May 2004 Exercise, the following matrices represent the surge capacity potential for Wisconsin Hospitals by region (see Appendix A: Map of HRSA Hospital Disaster Preparedness Regions). These beds cannot be counted as surge beds. “Emptying Beds” may be a strategy that can be used in a time-limited traumatic event. In a sustained event, however, these beds will quickly be filled by the “normal sick and injured.” 2 Hospitals were asked to look at all available spaces for conversion to inpatient surge capacity to determine the maximum capacity. This number will be refined with the publication of these “Guidelines”. 1 Intro-1 Region 1 2 3 4 5 6 7 State Total Staffed Beds 1,211 1,184 1,028 694 2,381 991 5,433 12,922 Available Beds3 808 641 588 452 1,066 651 2,757 6,963 Surge Beds4 2,198 1,710 1,828 1,016 2,629 1,337 6,985 17,703 Note: It is important to recognize that the above number of “17,703 additional inpatient beds” does not mean that hospitals have actual beds that can be deployed. The matrix below displays the actual “available surge beds” to accommodate a surge of inpatients. Region Surge Beds 1 2 3 4 5 6 7 State Total Surge Cots Surge Beds Needed 2,198 1,710 1,828 1,016 2,629 1,337 6,985 17,703 Available Surge Beds5 1,171 552 612 448 1,284 370 2,199 9,230 Surge Beds Needed6 1,027 1,158 1,216 568 1,345 967 4,786 11,067 (2,600)7 8,473 Since any mass casualty incident will be local in nature, it is the responsibility of each hospital to have the ability to implement this Inpatient and Outpatient Surge Capacity Plan. How long the hospital will need to manage this surge of patients will depend, of course, on the intensity and geographical footprint of the area affected. “Available Beds” are defined as those inpatient beds that can be made available through such strategies as early discharge, cancellation of elective admissions, etc. 4 “Surge Beds” are defined as those additional inpatient beds, not now operational or staffed, that can be deployed if necessary. 5 “Available Surge Beds” are those beds that hospitals identified in the May 2004 exercise that they have physically available on-site. It should be noted that these are beds that do not necessarily meet the criteria for surge capacity beds as outlined in Section 6 of this plan, since these criteria were not available to hospitals at the time of the exercise. 6 “Surge Beds Needed” are additional inpatient beds that will need to be obtained from other sources. 7 These “beds” are specially designed military cots that will be pre-positioned at hospitals for use in a surge capacity incident. 3 Intro-2 These Guidelines provide hospitals with a plan to manage a potential surge of approximately 11,830 patients8. This surge of patients could result from an extremely traumatic incident such as a grandstand or building collapse. However, a pandemic flu incident could begin to push even these limits. Each flu season finds many hospitals at full bed capacity with their resources pushed to the limit. In the event of a catastrophic mass casualty incident such as a nuclear explosion or a “Hurricane Katrina Incident”, even this mass casualty surge capacity may not provide sufficient inpatient and outpatient treatment capacity and thus overwhelm the capacity of the healthcare system to manage a catastrophic event. 8 This number is based on available surge beds at hospitals (9,230) in addition to the surge cots (2,600) that are to be pre-positioned at hospitals. Intro-3 1. Types of Incidents There are two major types of mass casualty incidents that may occur: Traumatic incidents may be caused by multiple vehicle accidents, building collapse, explosions, chemical spills, airplane crash, etc. Hospitals will be alerted as to the time of the incident and the Estimated Time of Arrival of the casualties. These incidents are usually time-limited as to their duration. In most cases, within 24 hours from the inception of the incident, the total surge of patients will have arrived at the hospital. Soon thereafter, patients will have been stabilized and treated and the discharge of the first of these patients will occur. Within days, the hospital can expect to return to near normal operations. Except for explosive events, where there may be large numbers of burn patients, it is expected that, in most traumatic incidents, hospitals will be able to manage those in need of long-term hospitalization. Biological incidents may be caused deliberately by such agents as anthrax or smallpox or indeliberately by pandemic flu or by other infectious disease outbreaks. In these incidents, the identification of the incident will occur over time and the surge of patients will occur slowly at first and may then peak considerably at a certain time due to the incubation period. The duration of these incidents cannot be determined and may last for weeks and even months, such as in the case of pandemic flu, which can come in several waves over long periods of time. These Guidelines will address surge capacity for both types of incidents. These Guidelines will apply similarly to both types of incidents with a few special considerations for biological incidents. 1-1 2. Increasing Availability of Existing Inpatient Beds There are various strategies to increase existing inpatient bed capacity such as early discharge of patients, cancellation of elective admission, etc. In a traumatic incident it is recommended that this strategy be used only as a secondary strategy with the opening of surge capacity areas as the first strategy. This is due to the fact that staff will be occupied with the surge of patients and will not have time initially to begin the implementation of the strategies to make occupied beds available. It is expected that patients in a traumatic incident will arrive faster than occupied beds can be “emptied” or made available. In addition, the in-house and outside “traffic”, created by these “emptying” strategies, may add to the congestion, caused by the incoming surge of patients and the family members, media and general public that will arrive at the hospitals along with these victims. This “emptying” strategy will prove more effective and more clinically appropriate as the “surge patients” are treated and then moved to more appropriate beds, which will be made available through early discharge and other such “emptying” strategies. The goal is to return to “normal” operations and bed configurations as soon as possible. 2-1 3. Field Triage Before a hospital can begin to establish its inpatient surge capacity plan, the staff responsible for the implementation of this plan must be familiar with the triage protocols that will take place in the field. This process involves triaging (“sorting”) patients by their severity of injury, based on a color-code system, which is widely used by EMS and First Responders and their hospital partners. The Wisconsin EMS Emergency Preparedness Plan (WEEPP) has recommended the use of START (Simple Triage and Rapid Treatment) as the triage protocols for adult patients and JumpSTART as the triage protocols for pediatric patients (see Appendix B: START Triage Algorithm and Appendix C: JumpSTART Triage Algorithm). START and JumpSTART uses the following color codes to triage (“sort”) patients: GREEN designates patients that are ambulatory and thus their injuries may be of a minor nature. It is anticipated that GREEN patients, in a mass casualty incident, will not be transported to hospitals, but rather will receive initial treatment in the field and/or be transported to alternative outpatient treatment centers (see Section 13). YELLOW designates patients that do not need immediate care and thus are triaged for “delayed” treatment. RED designates patients that are in need of immediate care. BLACK designates patients that either have died or whose injuries are so severe that they are expected to die and thus are designated as “Expectant”. In a mass casualty incident, the number of BLACK patients may increase due to the limited resources and will be brought to the hospital for palliative care. The triage principle that will be used in the field and in the hospital is “Do the greatest good for the greatest number.” 3-1 4. Opening/Creating Areas or Wings for Inpatient Surge Capacity The May 2004 Exercise demonstrated that hospitals were very creative in the identification of wings, areas and spaces that could be opened and/or converted for use as inpatient treatment areas. These potential treatment areas included such areas or spaces as: Waiting Rooms Wings previously used as inpatient areas that can be reopened Conference Rooms Physical Therapy Gyms Appendix D: Example of Hospital Surge Capacity provides an example of the type of data, produced by the May 2004 exercise, which is available for each of the 128 medical/surgical hospitals in the State of Wisconsin. Obviously, there is a hierarchy among these rooms as to which would best and first be used as inpatient surge capacity treatment areas. These Guidelines are intended to provide hospitals with recommendations on how to determine which areas and rooms can best be used for which patients. It is important for the hospital to consider other areas that will be also be affected by the surge of inpatients so that not all space is targeted for inpatient care. For example, a surge of patients will also bring a surge of family members and visitors. Spaces need to be identified to accommodate the needs of these people. For example, the cafeteria usually is a large area that could accommodate inpatient surge beds. However, this space will be necessary for food services for staff and visitors. Family members and visitors will also need spaces to congregate and relax. Patients from distant areas will be accompanied by family and friends, who may stay at the hospital for long periods of time. This selection of areas to be used for surge capacity can best take place when the hospital has an understanding of the intensity of the incident and the resulting number of surge patients that it may receive. Collaboration and the establishment of alert protocols with EMS and other First Responders and the Emergency Operations Center (EOC) will provide hospitals with the necessary information to implement the appropriate number of inpatient surge beds. The following Incident Level Matrix was developed by the Expert Panel to help hospitals tier their plans for the implementation of inpatient surge capacity beds, based on the number of patients expected: 4-1 INCIDENT LEVEL MATRIX Incident Level I II III IV V Number of Patients Expected 1 – 10 11 – 25 26 – 50 51 – 100 >100 Each hospital is expected to build their inpatient surge capacity plan, based on the number of staffed beds they have available. A rural Critical Access Hospital with 20 staffed beds will have a plan that is different than that of a metropolitan hospital with 300 beds. Commentary: The Expert Panel agreed that a disaster code at most hospitals, calls for a response from everyone at the hospital. Consideration is to be given to calling a Disaster Code by the Level of Incident so that only the appropriate resources are deployed, based on the different levels of incident. For example, only ED staff and certain others may need to respond to a Level I incident, while everyone responds to a Level V. Classification of Surge Capacity Beds by Triage Colors The following guidelines are written to help hospitals initially triage or “sort” their surge capacity beds and identify which beds can best be used for which type of patient. Thus, if a hospital is told that it should expect to receive 10 RED patients and 15 YELLOW patients, the hospital will have pre-identified in this plan which rooms can best serve the needs of these patients. Thus, the inpatient surge capacity rooms should initially be designated by the following triage color codes: RED rooms are to be designated for the care of patients in need of immediate care. These RED surge capacity rooms are rooms, which need to be similar to ED rooms with the required gases and equipment. Examples of such rooms are PACU and ICU rooms or, if necessary, a medical/surgical room. YELLOW rooms are to be designated for the care of patients, whose treatment can be delayed. These are medical/surgical rooms or areas or other rooms that are in close proximity to existing medical/surgical rooms and also in close proximity to ancillary services and supplies. BLACK rooms are to be designated for the palliative or comfort care of patients and may be rooms that are more distant from the core acute care service areas because these patients will be provided only with minimal services. 4-2 IMPORTANT: As in the field, all these patients will need to be constantly retriaged. The color designation may change several times for these patients. Application of Color-Coded Surge Beds According to the Level of Incident The initial alert from the field will give the hospital information regarding the number of color-coded patients that are expected to be transported to the hospital. This will enable the hospital to determine which areas or rooms it will use to care for RED, YELLOW and BLACK patients. Level I: It is expected that at this Level most hospitals9 will be able to handle the surge of inpatients with its existing inpatient staffed bed capacity without the need to deploy any inpatient surge capacity beds. Level II: The first consideration for the hospital is how many RED patients will be coming to the hospital. According to the Incident Level Matrix, Level II will involve 1125 patients. RED patients should ideally be placed in ED rooms. If there are more RED patients than there are ED rooms, then there must be the deployment of areas that can be designated as RED surge capacity rooms, where these RED patients can receive immediate treatment. In this case, these rooms are more treatment areas than they are inpatient rooms. Level III, IV and V: The hospital is to have pre-identified inpatient surge capacity areas for RED, YELLOW and BLACK patients. The Surge Capacity Matrix (see Worksheet 2) should also enable the hospital to identify the maximum number of RED, YELLOW and BLACK patients that the hospital can manage. However, even if hospitals have identified only a certain number of RED rooms, e.g. 10 RED rooms, if 15 RED patients are transported to the hospital10, then the hospital will have to tap into the next level of YELLOW rooms and “do the best they can to meet the needs of their patients, given the limited resources.” 9 The Panel recognizes that there is significant variation among hospitals in their ability to manage a surge of patients and that for a small Critical Access Hospital, even 1 – 10 patients in a Level I incident may be overwhelming. 10 Hospitals must keep in mind that in the midst of this surge incident, “normal sick and injured patients” will still present to the hospital. An “MI” patient in this case will be designated as another RED patient. 4-3 Example of a Surge Capacity Matrix The following Surge Capacity Matrix (see Worksheet 2) is an example of the Inpatient Surge Capacity Plan for St. Camillus Hospital. The Surge Capacity Matrix (see Worksheet 2) shows which surge capacity areas St. Camillus Hospital will open first and for which type of color-coded patient. Note: In the Surge Capacity Matrix (see Worksheet 2), the number in parentheses is the estimated number of beds, which normally may be expected to be unoccupied, based on the average daily census of the hospital. According to the following Surge Capacity Matrix (see Worksheet 2), for a Level I incident, St. Camillus projects that it may have (on average) 2 unoccupied beds in ICU for RED patients, 13 for YELLOW patients and 10 for BLACK patients. If St. Camillus Hospital were to receive more than 2 RED patients, the hospital would then go to Level II of the Surge Capacity Matrix (see Worksheet 2) to see what rooms it would then use for these additional RED patients. In this case, the hospital could utilize either the 2 beds in PACU or the 5 beds on 3 West Rooms 301 - 315. This Surge Capacity Matrix (see Worksheet 2) obviously is not “black-and-white” and the nursing managers will need to meet periodically to evaluate bed availability and decide which pre-designated, color-coded beds may best be used for which patients. The following Surge Capacity Matrix (see Worksheet 2) provides guidance to St. Camillus Hospital on how it will make unoccupied inpatient rooms available for a surge of inpatient and also which surge capacity areas they will open first, based on the initial estimate of patients that they have been told that they can expect. Level I Incident (1- 10 surge patients expected): The hospital has available 25 unoccupied beds that can be used for a surge of inpatients. (This total is arrived at by adding together all the numbers in parentheses: 2 RED beds, 13 YELLOW beds and 10 BLACK beds.) Level II Incident (11 – 25 surge patients expected): The hospital has available 28 unoccupied beds that can be used for a surge of inpatients and can open 10 surge capacity beds for a total of 38 surge capacity beds. Level III Incident (26 – 50 surge patients expected): The hospital has available 31 unoccupied beds that can be used for a surge of inpatients and can open 25 surge capacity beds for a total of 56 surge capacity beds. 4-4 Level IV Incident (51 – 100 surge patients expected): The hospital has available 29 unoccupied beds that can be used for a surge of inpatients and can open 75 surge capacity beds for a total of 104 surge capacity beds. Level V Incident (>100 surge patients expected): The hospital has available 31 unoccupied beds that can be used for a surge of inpatients and can open 123 surge capacity beds for a total of 154 surge capacity beds. SURGE CAPACITY MATRIX Note: The number in parenthesis indicates the number of beds usually unoccupied on any given day. The number in BOLD indicates the number of surge capacity beds that can be deployed. I Number of Patients Expected 1 – 10 Rooms for RED Patients ICU: Rooms 1 – 6 (2) Rooms for YELLOW Patients 3 West: Rooms 301 – 345 (13) Rooms for BLACK Patients 2 West: Rooms 201 – 235 (10) II 11 – 25 ICU: Rooms 1 – 6 (2) PACU: Beds 1 – 4 (2) 3 West: Rooms 301 – 315 (5) 3 West: Rooms 316 – 345 (9) 2 West: Rooms 201 – 235 (10) Meeting Room A: 10 beds III 26 – 50 ICU: Rooms 1 – 6 (2) PACU: Beds 1 – 4 (2) 3 West: Rooms 301 – 325 (11) 3 West: Rooms 325 – 345 (6) 2 West: Rooms 201 – 235 (10) 3 West Atrium: 10 beds Meeting Room A: 10 beds PT Gym: 15 beds IV 51 – 100 ICU: Rooms 1 – 6 (2) PACU: Beds 1 – 4 (2) 3 West: Rooms 301 – 335 (11) 3 West: Rooms 336 – 345 (3) 2 West: Rooms 201 – 235 (11) 3 West Atrium: 10 beds 2 West Atrium: 10 beds Sun Porch: 10 beds Meeting Room A: 10 beds PT Gym: 15 beds Employee Lounge: 20 beds Level 4-5 V >100 ICU: Rooms 1 – 6 (2) PACU: Beds 1 – 4 (2) 3 West: Rooms 301 – 345 (13) 3 West: Rooms 336 – 345 (3) 2 West: Rooms 201 – 235 (11) 3 West Atrium: 10 beds 2 West Atrium: 10 beds Board Room: 20 beds Sun Porch: 10 beds Meeting Room A: 10 beds PT Gym: 15 beds Employee Lounge: 20 beds Chapel: 8 beds Endoscopy: 5 beds Basement Meeting Room: 15 beds Cohorting Surge Patients The Expert Panel has recommended that hospitals cohort surge capacity patients rather than spread them out through the hospital, based on which beds are unoccupied. This cohorting will also be necessary for pediatric and adolescent patients. For example, the following is the surge capacity availability for St. Camillus Hospital for a Level II Incident: Level II Number of Patients Expected 11 – 25 Rooms for RED Patients ICU: Rooms 1 – 6 (2) PACU: Beds 1 – 4 (2) 3 West: Rooms 301 – 315 (5) Rooms for YELLOW Patients 3 West: Rooms 316 – 345 (9) 2 West: Rooms 201 – 235 (10) Rooms for BLACK Patients Meeting Room A: 10 beds If the hospital receives 15 RED patients, it may want to move the existing patients from the 3 West Rooms 301 – 315 to 3 West Rooms 316 – 345 so that RED patients can be cohorted on 3 West Rooms 301 - 315. This cohorting will allow for better patient care for both existing and surge patients. The same cohorting should occur for YELLOW patients. 4-6 Summary of Surge Capacity Beds Another way to display this Surge Capacity Matrix (see Worksheet 2) is to simply list the potential numbers of inpatient surge capacity beds by color-coded area to more easily see the number of surge beds available for each patient type. According to this Surge Capacity Summary (see Worksheet 3), St. Camillus does not have a good availability of surge beds for RED patients. Thus, the hospital knows that it may need to use beds, designated for YELLOW patients as treatment rooms for RED patients. Please note that in this Surge Capacity Summary (see Worksheet 3), the numbers in the columns should not be added. Rather, the numbers in each row are totaled to indicate the number of surge patients that can be accommodated in each Level. SURGE CAPACITY SUMMARY I Number of Patients Expected 1 – 10 RED Rooms 2 YELLOW Rooms 13 BLACK Rooms 10 II 11 – 25 9 19 10 III 26 – 50 15 26 25 IV 51 – 100 15 44 45 V >100 17 64 73 Level 4-7 St. Camillus Hospital Surge Support Area Matrix St. Camillus Hospital has also pre-designated areas that will be used for other purposes such as waiting areas for family and friends, counseling areas, rest areas. The following Surge Support Area Matrix (see Worksheet 4) provides a plan for designating rooms or areas for such purposes. It shows which rooms will be used as the Level of Incident increases. Note: The support areas suggested in this Surge Support Area Matrix (see Worksheet 4) are for exemplary purposes only and the list of support areas needed is not intended to be inclusive: SURGE SUPPORT AREA MATRIX Room/Area Family Waiting Level II 3 West Waiting Room Level III Meeting Room 5 Level IV Meeting Room 6 Counseling Chaplain’s Office Discharge Planning Office Rest Area (with cots) 2 West Waiting Room Medical Library Administrative Conference Room Medical Library Hallway Media Physical Therapy Office Radiology Conference Room Physical Therapy Gym EMS Garage EMS/Law Break Room Child Care Physical Therapy Gym Physical Therapy Gym Level V High School Neurology Lab Emmanuel Lutheran Church Hall Other essential room needs will be holding areas for patients that may have been early discharged, who are waiting to be picked up. A surge of GREEN patients at the hospitals or at alternative outpatient treatment sites may also need a holding area where they can wait before they are cared for. 4-8 5. Inpatient Units for Special Consideration There are a number of inpatient areas that are not clinically suited for surge capacity use. The following list is not to be considered as inclusive and each hospital will need identify the areas that may not be suitable for surge capacity use. OB is recommended to be considered as a “clean” unit (no infectious patients should be placed in OB), but may be filled with other “clean” patients only as a last resort. However, some OB rooms also should be held for new deliveries. It is not recommended to count OB as potential surge capacity areas, since its use will be limited and any available OB beds may need to be used for “normal sick and injured” female patients. Any unit that is used for immuno-suppressed patients should be treated in the same way as the OB unit and thus should not be counted as inpatient surge capacity beds. PEDS beds that have smaller sized beds or cribs should be counted as potential inpatient surge capacity beds, but only for PEDS patients. Nursery beds are not to be considered as potential inpatient surge capacity beds even for infants, since these beds are used only for neonates <28 days. If an infant with an infectious disease or with trauma is brought in, the infant is to be placed in PEDS. 5-1 6. Criteria for an Inpatient Surge Capacity Bed The May 2004 Exercise documented that hospitals have physically available on-site a limited number of beds that can be used when inpatient surge capacity areas are opened. The question was raised in the exercise as to what can be used for a surge capacity “bed”. The following criteria were developed by the Expert Panel to identify what should qualify for a surge capacity “bed”: 1. 2. 3. 4. the bed provides for full horizontal (head to toe) support of a patient the bed has protective mechanisms such as litter straps or side rails the bed is at working level height the bed is designed to be moved by carry or by wheel. (Limited staff availability to move the “bed” is also to be considered when evaluating whether a “bed” can be used for inpatient surge capacity)* 5. the bed has the capability to hang an IV (if this capability is not available on the bed, the hospital must have options to hang the IV (ceiling hooks, etc.) in the surge capacity area. *Note: Beds that are heavy or not easily moved can be used for BLACK patients, since these beds are not likely to be moved. 6-1 7. State Stockpile of Inpatient Surge Capacity Beds A panel of experts (Infection Control, Ergonomics, Laundry, Pressure Mapping, Physical Therapy) investigated an “army style cot” for use as a surge capacity bed. Various recommendations were made to the manufacturer, resulting in the surge capacity cots that are have been made available to hospitals: a. b. c. d. e. f. the “army style” cot was 18 inches in height; it was raised to “24” to mimic normal bed height and to allow a patient more easily to lift him/herself out of the bed with his/her feet the “army style” cot was 24” in width; it was widened to 34” to allow a patient to roll on his/her side and to increase overall comfort the “army style” cot had fabric that can easily be cleaned with normal hospital cleaning supplies; no changes were recommended the “army style” cot had construction and fabric with identified “pressure areas” that could result in an immobile patient acquiring bed sores; inflatable mattresses will be purchased as an adjunct to the cot; the “army style” cot had no IV pole; a tethered IV pole 18” in height was added to the cot the “army style” cot came with a pocket that hangs from the side of the cot that can contain patient personal items and also hold a patient chart/clipboard An initial supply of 2,600 cots is to be pre-positioned at hospitals. It is also planned to have an additional stockpile of these cots, stored in trailers that can be brought to the hospital(s), requesting additional surge beds. 7-1 8. Patient Care Staffing for Inpatient Surge Capacity Areas The Surge Capacity Matrix (see Worksheet 2) can also to be used as a tool to determine the staff needed for these inpatient surge capacity beds. Hospitals are to plan for staffing for the first 72 hours of a traumatic incident. It is felt that in the first 72 hours of a traumatic incident, especially if other hospitals are involved, there will not be the ability to call upon other organizations for assistance or to begin to recruit volunteers to assist, given the time necessary to implement these processes. A hospital will need “to do what it must do” to manage the surge of patients that comes to the hospital. Given the human resource problems that hospitals face in filling existing positions in “normal” times, there is no “surplus labor pool” in the community that the hospital can easily draw upon. For example, the state volunteer registry has over 1,100 registered volunteers. Of these registered volunteers about 20% are RNS, 15 % LPNs and 1% are physicians. The majority of these registered volunteers are already employed at various health care organizations and may not be available for service, since they may be needed by their own facility. Staffing Strategy Given the fact that, especially in the first 72 hours, there will be limited additional staff, the Expert Panel has recommended the consideration of the following staffing strategies: Strategy One: staffing ratios will need to be adapted to the need. Each of the colorcoded patient categories will require different staffing ratios. Strategy Two: 8 hour shifts may be changed to 12 hour shifts Strategy Three: work tasks are to be prioritized so that only essential patient care tasks are provided by staff. (see Appendix E: Prioritization of Patient Care Tasks) Strategy Four: hospitals are to consider using family members for certain tasks such as bathing and feeding the patient Strategy Five: the hospital can put out a call through the media for volunteer health care workers In regard to Strategy Five, although the hospital may consider a campaign to recruit additional healthcare workers in an incident, this will be a service provided by the local or state Emergency Operations Center (EOC), if the EOC is activated. Wisconsin Disaster Credentialing (WDC) is a web-based process for the credentialing and privileging of volunteer healthcare workers that is available to hospitals. 8-1 Assignment of Staff to Color-Coded Beds In a surge incident, it is most likely that the hospital will not have the right mix of RNs, LPNs and Nurse Assistants and other staff and will need to assign available staff and volunteers to the color-coded beds, based on the skills sets that they possess. The Expert Panel has recommended the following minimum skill sets that staff are to have in order to provide patient care, based the color-coded designation of the patient: 1. Staff skills necessary to care for RED patients: These are to be staff or volunteers, who are acute care RNs and Residents, who can perform primary and secondary assessment of critical care patients. The hospital can also use acute care LPNs, technicians, PCAs and student nurses to assist these RNs and Residents; this will allow for increased productivity of these RNs and Residents. 2. Staff skills necessary to care for YELLOW patients: These are to be staff or volunteers, who are RNs and LPNs, who can perform initial and on-going assessment of patients and who are presently employed either in acute care settings or in nonhospital work sites. 3. Staff skills necessary to care for BLACK patients: These are to be staff or volunteers, who are comfortable with death and dying, such as: a. b. c. d. e. f. hospice volunteers clergy social workers retired Health Care Workers hospital volunteers members of service organizations It will be necessary to have a RN supervisor and Team Leader in each area to assess these staff, their skills and their stress and rehabilitation needs. Staffing Ratios It will be very difficult to plan for staffing these areas, given existing staffing shortages in most hospital in most areas. The following suggested ratios are meant only to give the hospital an estimated number of staff that it will need for planning purposes: Note: The higher ratio may be used if the patients are cohorted. 8-2 STAFFING RATIOS FOR SURGE CAPACITY MATRIX I Number of Patients Expected 1 – 10 Patient Care Staff Ratios for RED beds Existing Staff Patient Care Staff Ratios for YELLOW beds Existing Staff Patient Care Staff Ratios for BLACK beds Existing Staff II 11 – 25 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 III 26 – 50 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 IV 51 – 100 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 V >100 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 Level The above ratios assume that nurses and other care givers are providing only essential patient care services. The ratios also will vary based on the acuity of the patients. For example, based on these ratios, the hospital can estimate that if it is to be receiving 10 RED patients, it will need 5 RNs (1:2 ratio); if it is receiving 20 YELLOW patients, it will need 4 RNs (1:5 ratio). The hospital needs to consider at what point it can no longer accept other patients. The best indicator of this threshold may be the physical and emotional status of the staff as they manage this surge. Job Action Sheets The hospital is to have Job Action Sheets (see Appendix F) for each of the color-coded areas, detailing the responsibilities that the staff are to carry out. In addition, these Job Action Sheets are to detail the location of supplies, ancillary services and other such information so that those HCWs, who may be unfamiliar with the particular area, have available this information on where they can find supplies and equipment. Managing the Continuum of Care after the Initial Surge of Inpatients The categorization of rooms as RED, YELLOW and BLACK will assist the hospital with initially receiving patients from the field. This initial period may last for approximately 24 hours. As patients are received and retriaged, it becomes more necessary to plan for housing these patients, based on their acuity. It is suggested that the color-coded rooms TRANSITION to your traditional hospital terminology. On the Transition Matrix (see Worksheet 6) below, each hospital will use the terminology for beds that is common at that hospital. 8-3 TRANSITION MATRIX Beds: First 24 Hours RED Beds: > 24 Hours Critical Care YELLOW Monitored Intermediate Care YELLOW/BLACK Medical/Surgical Care Secondary Surge It is very likely that the hospital will experience a secondary surge in inpatients 24 hours or more after the initial surge, caused by the incident. This may be due to some GREEN patients, who present with their illness/injury exacerbating, causing them to seek help at the hospital. The “normal sick and injured” will continue to present to the hospital. Some patients, who may have delayed presenting at the hospital, may now present, thinking that the “surge” is over. In addition, the hospital should consider that the patient length of stay will most likely increase due to the lack of resources to care for patients according to the “normal” protocols. Services such as surgery and the ancillaries may be fully “booked”, caring for the surge of patients and thus patients may need to wait for these services. It is recommended, in a surge capacity incident, that a Medical Staff Admissions Committee be formed on an ad hoc basis to assist physicians in determining whether or not certain patients need to be admitted. Some physicians may be reluctant to have the admission of their patients delayed and will need the support of both hospital administration and their physician peers to understand that the delay of admission of their patient(s) is medically appropriate under these surge conditions. 8-4 Discharge Planning and Case Management In the first 24 hours, these professionals may be concerned with “bed emptying” strategies. The role of these professionals becomes even more critical >24 hours after the incident as they assist in the management of the inpatients, involved in the surge incident. They will need to present options to physicians to assist in the management of these inpatients and discharge them as soon as it is medically appropriate. It is recommended, in a surge capacity incident, that a Medical Staff Discharge Committee be formed on an ad hoc basis to assist physicians in the discharge of their patients. Some physicians may be reluctant to have their patients early discharged and will need the support of both hospital administration and their physician peers to understand that the discharge of their patient(s) is medically appropriate under these surge conditions. It is also recommended that these professionals develop Job Action Sheets for other person, who may be called upon to assist with the discharge process. Having “checklists” prepared may assist with “just-in-time” training for those called upon to assist with the discharge process. 8-5 9. Ancillary Care Staffing for Inpatient Surge Capacity Areas As it is essential for the hospital to have a plan and a strategy to have staff to provide patient care in the inpatient surge capacity areas, it is equally important that each ancillary department also have a plan and a strategy to have the staff and supplies necessary to support these inpatient surge capacity areas. The Ancillary Support Matrix (see Worksheet 7) can also be used as a tool for this purpose with each department completing the Ancillary Support Matrix (see Worksheet 7). Ancillary services are to consider not only the staffing necessary to care for patients and staff, but also the staffing necessary to care for additional family members and visitors, who may come to the hospital with the surge of inpatients. The following ancillary departments are to complete their staffing plans and strategies (the list is an example only and is not intended to be inclusive): Housekeeping Food Services Security Radiology Laboratory Admissions Billing Medical Records Pastoral Care Transport Services Day Surgery Chemotherapy Dialysis 9-1 ANCILLARY SUPPORT MATRIX I Number of Patients Expected 1 – 10 II 11 – 25 III 26 – 50 IV 51 – 100 V >100 Level Housekeeping Staff for RED rooms Existing Staff Housekeeping Staff for YELLOW rooms Existing Staff Housekeeping Staff for BLACK rooms Existing Staff ANCILLARY SUPPORT MATRIX I Number of Patients Expected 1 – 10 II 11 – 25 III 26 – 50 IV 51 – 100 V >100 Level Food Services Staff for RED rooms Existing Staff Food Services Staff for YELLOW rooms Existing Staff Food Services Staff for BLACK rooms Existing Staff Each department is to complete its own Ancillary Support Matrix (see Worksheet 7). Departments and functions, however, are to collaborate to determine which staff can be pulled from other departments to assist with these functions so that departments do not identify and depend upon the same staff. 9-2 10. Staff Support Considerations The following are other issues that the hospital is to consider for its staffing plans and strategies. The hospital should consider the formation of Staff Disaster Support Committee or have its Human Resources Department pre-plan for the following (the list is not intended to be inclusive): 1. Some staff will not be able to report to work due to the fact that they or their loved ones may have been directly involved in the incident. There should be a policy to address these absences and also some strategies to provide support to these employees. 2. Some staff will refuse to report to work due to concerns about their own and their family members’ safety and health. In the case of a biological incident, they may have fear of contracting the disease or bringing the disease home. There should be a policy to address these absences and also some strategies to provide support and or options to these employees. 3. Many staff will have concerns about childcare. The normal childcare provider may not be able to provide these services in an incident. These same concerns apply to staff, who may be caring for their parents or others. There should be options available for childcare/eldercare so that staff are free to report to work. 4. Some staff may have concerns about the shelter and care of their pets. 5. The hospital is to consider the provision of rooms for staff for rest and sleep and for personal hygiene needs (blankets, pillows, sheets, showers, towels, soap, shampoo, etc.). In the case of a biological incident, there may be the implementation of work quarantine in addition to staff working longer shifts or not being able to go home. The hospital may also want to consider what is available in local hotels, churches, and other such organizations for sleeping accommodations and showers. 6. The hospital is to consider areas for staff to eat and have refreshments 7. Staff may be away from home for extended shifts and need to communicate with family members and other loved ones. The hospital is to consider the availability of telephones to call home and computer access for email. 8. For staff working extended shifts or not going home, there may be the need for laundry services or the provision of scrubs. Staff are also to consider having an “Emergency Kit” with personal items such as underwear, socks, toiletries, a supply of medications, etc. readily available so that this “Kit” is readily available. 10-1 9. Staff are to also have a “Family Plan” so that everyone in the family knows what will need to happen and who is responsible for various duties if a family member, who works at the hospital, needs to work longer shifts or is quarantined at the hospital. 10. The hospital should also give consideration for back-up of essential services such as food services, laundry, housekeeping and other services, especially if these services are out-sourced and the incident affects the ability of the contractor to continue to provide these services and if the surge of patients and visitors overwhelms the capacity of these contractors. 11. Most hospitals use “calling trees” to notify staff. The hospital is to consider a back-up system for notifying staff should the telephone lines be down or the circuits busy. 12. The hospital is to consider pre-identifying staff persons, who will manage and supervise volunteers and in which areas or departments the hospital is likely to utilize volunteers. 13. The hospital is also to consider that there may not be sufficient managers to supervise the staff in the surge capacity areas. 14. With staff being asked to work in the surge capacity areas, work in these areas may not necessarily involve their normal work responsibilities. It is suggested that Job Action sheets be available for all positions in the RED, YELLOW and BLACK surge capacity areas so that staff can receive “just-in-time” training by reading the Job Action Sheets. 10-2 11. Equipment and Supplies The inpatient surge capacity areas demand not only the availability of additional staff and beds. Each surge capacity areas will also needed the equipment and supplies necessary to deploy these beds. The hospital needs to determine the amount of equipment that will be needed in the area and how this equipment can be obtained for each Incident Level. This list will include such critical equipment as (the list is not intended to be inclusive): Crash carts IV pumps Defibrillators Portable suction Syringe pumps Portable oxygen Ventilators Blood PCA pumps Commodes Privacy Screens Pressure infusers Warming devices The following are key issues that the hospital is to consider when developing its list of equipment: 1. The hospital is to estimate the amount of equipment that will be needed for each color-coded area, tiered for each Incident Level. 2. The hospital is to consider equipment needs for both adult and pediatric patients. 3. The hospital or its Material Management Director is to identify where this equipment is located in relation to the surge capacity areas so that staff not familiar with equipment location can know where to obtain it, based on the surge capacity area they are working in (see Equipment Location Matrix: Worksheet 8). 11-1 EQUIPMENT LOCATION MATRIX Surge Area: Critical Equipment Crash carts IV pumps Defibrillators Portable suction Syringe pumps Portable oxygen Ventilators Blood PCA pumps Commodes Privacy Screens Pressure infusers Warming devices Location 4. The hospital is to consider what can be used as an alternative if particular equipment is not available. 5. The hospital or its Materials Management Director is to determine the potential source(s) of where this equipment can be obtained (see Equipment Source Matrix: Worksheet 9). This list should include not only suppliers and vendors, but also local clinics, nursing homes, etc. that may be sources of this equipment. EQUIPMENT SOURCE MATRIX Critical Equipment Crash carts IV pumps Defibrillators Portable suction Syringe pumps Portable oxygen Ventilators Blood PCA pumps Commodes Privacy Screens Pressure infusers Warming devices Source 11-2 6. The hospital is also to identify the electrical power available in these surge capacity areas. Rooms that will be powered by emergency power need to be prioritized for RED patients, since these are the most likely patients to be using electrical equipment. Although not included on the equipment list, the hospital is to have flashlights or other battery-powered light sources that may need to be used in those areas that will not have emergency power. Special Note on Crash Carts: Staff are to determine where these crash carts will be placed when inpatient surge capacity is activated. It is recommended that placement of these crash carts is based on the concentration of patient population versus distance. The hospital may also want to consider bringing in Automatic Electronic Defibrillators (AEDs) from the community as an optional supply source. Thus, the hospital may consider maintaining an inventory of where in the community these AEDs are maintained and note this on the Equipment Source Matrix (see Worksheet 9). Crash Cart Supplies from the ChemPacks: Medications and supplies on the crash carts may be quickly depleted. Although AEDs may be utilized, AEDs do not come with medications or supplies. The State has a cache of nerve agents antidotes (ChemPacks). These caches contain atropine and other medications that may be accessed. Appendix G: Medication in ChemPacks lists the medications and supplies that are included in the ChemPacks. Appendix H: Accessing the ChemPacks provides instructions on how these ChemPack caches may be accessed Critical Supply Inventory The hospital is to estimate the amount of supplies needed on the Critical Supply Inventory Matrix (see Worksheet 10). The Critical Supply Inventory Matrix (see Worksheet 10) is a tool to help the hospital determine the amount of supplies that may be needed, based on the maximum number of patients that it can accept. Instructions for Completing the Critical Supply Inventory Matrix (see Worksheet 10): 1. Identify the maximum number of patients that the hospital can accept by referring to the Surge Capacity Matrix (see Worksheet 2). (In the example of St. Camillus Hospital, their maximum number of patients is 17 RED patients, 64 YELLOW patients and 73 BLACK patients.) 2. This maximum number provides the hospital with a number to use when estimating the amount of supplies needed. This will help in comparing what is in normal inventory as compared to what may be needed and where these additional supplies can be obtained. 3. The hospital should estimate the amount of supplies based on a 72 hour period. After this time, there may be other resources available to help the hospital replenish its resources. 11-3 4. The hospital can add to or delete supplies from this list. For example stethoscopes are items that may be needed. 5. IMPORTANT: The hospital is to begin rationing and triaging of supplies immediately when the surge capacity plan is implemented. The process for requesting additional supplies is also to begin immediately upon activation of the surge capacity plan. (see Appendix I: Rationing of Supplies. For example, rationing may begin by not using IV solutions for patients that can take oral fluids by mouth. CRITICAL SUPPLY INVENTORY Maximum Number of RED Patients (X) Maximum Number of YELLOW Patients (X) 11-4 Critical Supply Inventory (X) IV tubing (X) IV start supplies (X) IV fluids (X) medicines (X) bed pans/urinals (X) needles/syringes (X) catheters (X) dressings (X) linens (X) alcohol wipes (X) tape (X) hand sanitizer (X) PPE (X) OB delivery supplies (X) casting supplies Critical Supply Inventory (X) IV tubing (X) IV start supplies (X) IV fluids (X) medicines (X) bed pans/urinals (X) needles/syringes (X) catheters (X) dressings (X) linens (X) alcohol wipes (X) tape (X) hand sanitizer (X) PPE (X) OB delivery supplies (X) casting supplies Maximum Number of BLACK Patients (X) Critical Supply Inventory (X) IV tubing (X) IV start supplies (X) IV fluids (X) medicines (X) bed pans/urinals (X) needles/syringes (X) catheters (X) dressings (X) linens (X) alcohol wipes (X) tape (X) hand sanitizer (X) PPE (X) OB delivery supplies (X) casting supplies The hospital or its Materials Management Director is to determine the potential source(s) of where these supplies can be obtained (see Supply Source Matrix below). This list should include not only suppliers and vendors, but also local clinics, nursing homes, etc. that may be sources of this equipment. SUPPLY SOURCE MATRIX Critical Supplies IV tubing IV start supplies IV fluids Medications Bed pans/urinals Needles/syringes Catheters Dressings Linens Alcohol wipes Tape Hand sanitizer PPE OB delivery supplies Casting supplies Source Special Note on Supply Inventory: It will be very difficult to list all the various supplies that will be needed such as syringes, sponges, etc. The hospital is to have a process in place with its vendors for the immediate ordering of additional supplies. “Just-in-Time” inventories may cause problems in a surge capacity situation. 11-5 The goal is for the hospital to be self-sufficient for the first 72 hours. The Materials Management Director is to discuss with the vendor/supplier the back-up plan or Business Continuity Plan of the supplier/vendor, should the operations of the supplier/vendor also be affected. Memoranda of Understanding: All hospitals in the state have signed a Memorandum of Understanding (MOU), declaring their willingness to share staff, equipment and supplies with other hospitals. If the Emergency Operations Center in the jurisdiction has been activated, the hospital can call upon the EOC to assist in procuring needed supplies. The EOC Hospital Liaison will be available to assist the hospital Logistics Section Chief in the procuring of needed supplies and equipment. PPE Stockpiles: Each hospital, through the HRSA Cooperative Agreement, has received increased inventories of PPE for use in an incident, involving infectious disease. The State of Wisconsin also has stockpiled additional PPE that can be accessed by hospitals. Appendix J: Access to Personal Protective Equipment lists the PPE that is stockpiled and the protocol for accessing these stockpiles. Strategic National Stockpile/Vendor Managed Inventory: In an incident that has been declared a disaster by the Governor, the Strategic National Stockpile (SNS) will arrive in the state within 12 hours of notification of the Centers of Disease Control (CDC) by the state. The SNS is a national repository of antibiotics, chemical antidotes, antitoxins, lifesupport medications, IV administration, airway maintenance supplies, and medical/surgical items. The SNS is designed to supplement and re-supply state and local public health agencies in the event of a national emergency anywhere and at anytime within the U.S. or its territories. The SNS is organized for flexible response. The first line of support lies within the immediate response 12-hour Push Packages. These are caches of pharmaceuticals, antidotes, and medical supplies designed to provide rapid delivery of a broad spectrum of assets for an ill defined threat in the early hours of an event. These Push Packages are positioned in strategically located, secure warehouses ready for immediate deployment to a designated site within 12 hours of the federal decision to deploy SNS assets. If the incident requires additional pharmaceuticals and/or medical supplies, follow-on vendor managed inventory (VMI) supplies will be shipped to arrive within 24 to 36 hours. If the agent is well defined, VMI can be tailored to provide pharmaceuticals, supplies and/or products specific to the suspected or confirmed agent(s). In this case, the VMI could act as the first option for immediate response from the SNS Program. Appendix K: Strategic National Stockpile List of Assets lists the equipment, supplies and medications that are included with the SNS. 11-6 12. Triage Center The hospital is to consider the deployment of a triage center separate from the ER so as to maintain an easy, unobstructed access for patients, being transported by ambulance to the hospital. GREEN patients will be sent to alternative outpatient treatment centers for care and treatment. Only RED, YELLOW and BLACK patients will be treated within the hospital. The purpose of the Triage Center is to manage walk-in patients, who present to the hospital. It is expected that Transport Ambulances will notify the hospital prior to transport and no later than en route of the number of RED, YELLOW and BLACK patients that are being transported so that these patients can be taken directly to the ER. This same “alert” protocol to the hospital is to apply to the “normal sick and injured”, who are being transported to the hospital by the Transport Ambulance. Criteria for the Triage Center include: 1. sufficiently distant from the ED entrance and ambulance driveway so as not to congest the ED area 2. located on the hospital campus or in close proximity to the hospital campus 3. climate-controlled area 4. allow for unobstructed transport of patients by gurney or wheelchair from the Triage Center to the hospital 5. (for infectious disease incidents) HVAC is separate from the hospital HVAC system 6. communications capability with the hospital, especially ED, Nursing, and Admissions 7. ability to lock down the Triage Center It is important for the hospital to pre-identify this Triage Area and also to pre-identify staff by function, which will staff this area when it is deployed. It is also advisable to have Job Action Sheets for the persons, who will staff the Triage Center. Note: Most hospital have received a portable decontamination shelter that has the potential to be used as a Triage Center under certain weather conditions. Decontamination: Special consideration will need to be given to the decontamination of patients, if the incident calls for decontamination. If the hospital has a fixed decontamination room, there will need to be a plan for the flow and holding of patients, if there are large numbers of patients in need of decontamination. If the hospital has a portable decontamination shelter, then consideration needs to be given as to its placement relative to the Triage Center. 12-1 13. Outpatient Surge Capacity Each hospital is to have a plan whereby it can direct GREEN patients for care and treatment. Hospitals in a surge incident will be overwhelmed, especially the Emergency Department. The hospital will be challenged with the management of RED, YELLOW and BLACK patients. It is expected that GREEN patients will be directed from the field and through the media to go to Alternative Outpatient Treatment Sites. Various outpatient centers such as physician offices, clinics and Urgent Care Centers are to be identified as Alternative Outpatient Treatment Sites. It is anticipated that the physicians and their staff, who normally work in these outpatient centers, will be able to staff these areas. It is assumed that 1. these Alternative Outpatient Treatment Sites will need to be relatively close to the Triage Center 2. that the physicians and staff will have training on the deployment of their office as an Alternative Outpatient Treatment Site 3. that the physicians will bill for their services 4. that these offices will have limited supplies and equipment and a plan for supplying and resupplying these Alternative Outpatient Treatment Sites needs to be addressed 5. that these sites will serve not only the victims of the incident, but also the GREEN “normal sick and injured”, who will not be able to be treated in the ED The plan, to be developed in collaboration with the hospital and the physicians and staff of these outpatient centers, is to include protocols to deploy these Alternative Outpatient Treatment Sites after business hours and on weekends and holidays and also for extended periods of time (as long as there are patients in need of care). Critical to the success of the deployment of these alternative outpatient treatment sites will be a system to call up the physicians and staff and notify them of the need to deploy the site, especially outside normal business hours. In some locations, there are no clinics or other suitable sites adjacent or near to the hospital that can serve as these alternative outpatient treatment sites. In these cases, the hospital swill need to determine which locations on campus can best be utilized as these sites, since the goal is still to maintain the ED for RED and YELLOW patients. Since GREEN patients will be directed to report to these sites from the “field” and will also be redirected to these sites from the hospital, it is important that these sites be able to become operational at the same time that the Triage Center becomes operational. 13-1 The Expert Panel recommends that the hospital have a Memorandum of Understanding (MOU) with each clinic that will serve as an alternative outpatient treatment site. This MOU is to spell out all the terms under which the clinic commits to serving as an alternative outpatient treatment site. (see Appendix L: Template Memorandum of Understanding) The following Alternative Treatment Site Matrix (see Worksheet 12) can serve as a planning tool to assist the hospital in determining what outpatient centers may serve as alternative treatment sites for GREEN patients and also the “normal sick and injured”, who do not need immediate ED care and treatment: ALTERNATIVE TREATMENT SITE MATRIX Type of Patient/Injury/Illness Pediatric Patients Name and Location of Outpatient Center OB Patients Lacerations Broken Bones Patients in Need of Medical Evaluation Cardiac Symptoms Psychiatry Other 13-2 14. Exercise It is necessary for the hospital to exercise for “Day 2” and “Day 3” of surge incident scenarios. These exercises are to focus on physicians and staff, who are dealing with the 2nd wave of surge and its related problems such as strain on OR and ancillary services, the need to discharge patients, stress of staffing. These exercises should also consider other service areas such as housekeeping, laundry, food services and others, who are usually involved in a disaster drill through the “Labor Pool.” In a surge incident, these staff will also be stressed and overwhelmed as they deal with a surge of not only patients but also of the family members and visitors, who accompany the patients. For example, Food Services may see a 200% or even 300% increase in the cafeteria lines due to staff working longer shifts and an increased number of visitors. Each department is to exercise its own department surge capacity plan at least annually so that the specific department can focus on the issues that it will face. The exercise should also include discussion regarding the standard of care and how this will need to be adjusted. A mass casualty incident will result in a severe mismatch between “Patient Needs” and “Hospital Resources”. Thus, there may be a need to limit care, based on the principle of “the greatest good for the greatest number.” Most health care workers have not been faced with the situation where they will need to limit care for patients. This may become a necessity in an incident that produces a surge of patients. The Expert Panel recommends that the hospital look at exercising its surge capacity with its lowest level of staffing (usually during the third shift or using the third shift staffing levels as a proxy) to determine how well this surge of patents can be managed with these limited resources. 14-1 15. Off-Site Alternative Inpatient Treatment Centers The State Expert Panel has recommended the implementation of this in-house inpatient surge capacity plan versus the use of Off-Site Alternative Inpatient Treatment Centers. The logistics involved with these alternative inpatient treatment sites are daunting and the hospital may be better able to manage a surge on-site despite the challenges that this will present to the hospital. However, there is the scenario where the hospital has surpassed even its own in-house surge capacity and can no longer accept further inpatients. In addition, there may be the scenario where the hospital, itself, is damaged wholly or in part and may need to move its services off-site. The options in both of the above scenarios will be to transport patients from the “field” to other hospitals or from the damaged hospitals to other hospitals. If either of these scenarios occurs, it is likely then that the local or state EOC has been activated and this EOC will able to serve as a resource to the affected hospitals. 15-1 16. Risk Communications Even with the deployment of in-house surge capacity and the deployment of alternative outpatient treatment sites, these facilities may still be overwhelmed. Risk Communications are then to be employed for the following purposes: 1. instructions on how to prevent transmission of the disease 2. instructions on quarantine and isolation 3. instructions on home-care for yourself and/or for your family members, who are ill 4. instructions on what the indications are to seek care at the Physician’s Office 5. instructions on what the indications are to seek care at the hospital The purpose of these Risk Communications is to keep hospitals, Urgent Care Centers and Physicians’ Offices and Clinics open only for those who can truly benefit from these services. It will be important to begin Risk Communications at the onset of the incident so as not to overwhelm the hospitals and other treatment sites. 16-1 17. Business Continuity Plan A sustained disaster incident that takes place over days and even weeks will have serious effects on the business operations of the hospital. Although initially all staff may be called upon to help with patient care in some way, after a very short time, there is the necessity to continue with essential business operations such as medical records, billing, coding, etc. Each hospital department is to consider the effects of a sustained disaster on its operations and determine how it will carry out essential functions with limited resources in a sustained disaster. 17-1 18. Guidelines for Completing Your Hospital Surge Capacity Plan 18-1 Appendices Appendix A: HRSA Hospital Disaster Preparedness Regions Duluth Bayfield Douglas Iron Ashlan d Washburn Pol k Twin Cities St. Croix Pric e Sawye r Burnett Barron Dunn Vilas Florence Onied a Rus k Forest Marinette Lincoln Langlade Taylo r Chippewa Menomonee Marathon Clark Pierce Pepin Buffalo Oconto Oconto Door Shawano Eau Claire Portage Trempealeau Adams Junea u Vernon Sau k Richlan d Gree Marquette n Lake Dodg e Columbia Gree n Sheboyga n Fond du Lac Ozauke e Washington Jefferson Iowa La Fayette Calumet Waushara Dan e Gran t Kewaune e Manitowoc Winnebago Monro e Crawford Outagamie Brown Outagamie Wood Jackso n La Crosse Waupaca Rock Rockford Appendix A-1 Waukesha Walworth Milwauke e Racin e Kenosha Appendix B: START triage Algorithm Appendix B-1 Appendix C: JumpSTART Triage Algorithm Appendix C-1 Appendix D: Example of Hospital Surge Capacity St. Camillus Hospital Patient Care Units M/S ICU PEDS BURN PSYCH TOTAL Staffed Beds Available Beds 217 91 33 8 14 8 0 0 25 14 289 121 Surge Capacity Bed Capacity Available Beds Beds Needed Private Rooms 0 0 0 Converted Areas 189 84 105 Converted Areas Include: Rehab Bays 1- 5 Hallway OP Surgery PreOP Surgery and Care Center CPU Endoscopy Bay 6 Meeting Rooms/Waiting Rooms TOTAL 189 84 105 # of Beds 3 40 10 24 7 32 5 13 25 30 Total: 189 Detail of Patient Care Units 5SW 6W 3SW 1NW 4SW 3NW 37 13 15 4 35 11 26 16 37 11 31 10 OB M/S 36 26 217 91 MICU PICU SICU NICU ICU 12 2 7 4 10 0 4 2 33 8 Appendix D-1 Appendix E: Prioritization of Patient Care Tasks This Appendix is in development Appendix E-1 Appendix F: Job Action Sheets These Job Action Sheets are in development Appendix F-1 Appendix G: Medications in ChemPacks EMS CHEMPACK Container for 1000 Casualties Mark 1 auto-injector Atropine Sulfate 0.4mg/ml 20ml Pralidoxime 1gm inj 20ml Atropen 0.5 mg Atropen 1.0 mg Diazepam 5mg/ml auto-injector Diazepam 5mg/ml vial, 10ml Sterile water for injection (SWFI) 20cc Vials Sensaphone® 2050 Satco B DEA Container Unit Pack Cases QTY 240 100 276 144 144 150 25 100 1 11 1 1 2 2 4 4 3 1 2640 100 276 288 288 600 100 300 1 1 1 1 Hospital CHEMPACK Container for 1000 Casualties Unit Pack Cases QTY Mark 1 auto-injector Atropine Sulfate 0.4mg/ml 20ml Pralidoxime 1gm inj 20ml Atropen 0.5 mg Atropen 1.0 mg Diazepam 5mg/ml auto-injector Diazepam 5mg/ml vial, 10ml 240 100 276 144 144 150 25 2 9 10 1 1 1 26 480 900 2760 144 144 150 650 Sterile water for injection (SWFI) 20cc Vials Sensaphone® 2050 100 1 23 1 2300 1 1 1 1 Satco B DEA Container Appendix G-1 Appendix H: Accessing the ChemPacks This Appendix is in development Appendix H-1 Appendix I: Rationing of Supplies This Appendix is in development Appendix I-1 Appendix J: Access to Personal Protective Equipment This Appendix is in development Appendix J-1 Appendix K: Strategic National Stockpile List of Assets Appendix K-1 Appendix L: Template Memorandum of Understanding This Appendix is in development Appendix L-1 Worksheets Worksheet 1: Incident Level Matrix INCIDENT LEVEL MATRIX Incident Level I II III IV V Number of Patients Expected 1 – 10 11 – 25 26 – 50 51 – 100 >100 Worksheet 1-1 Worksheet 2: Surge Capacity Matrix SURGE CAPACITY MATRIX Note: The number in parenthesis indicates the number of beds usually unoccupied on any given day. The number in BOLD indicates the number of surge capacity beds that can be deployed. I Number of Patients Expected 1 – 10 II 11 – 25 III 26 – 50 IV 51 – 100 V >100 Level Rooms for RED Patients Worksheet 2-1 Rooms for YELLOW Patients Rooms for BLACK Patients Worksheet 3: Surge Capacity Summary SURGE CAPACITY SUMMARY I Number of Patients Expected 1 – 10 II 11 – 25 III 26 – 50 IV 51 – 100 V >100 Level RED Rooms Worksheet 3-1 YELLOW Rooms BLACK Rooms Worksheet 4: Surge Support Area Matrix SURGE SUPPORT AREA MATRIX Room/Area Family Waiting Level II Level III Counseling Rest Area (with cots) Media EMS/Law Break Room Child Care Worksheet 4-1 Level IV Level V Worksheet 5: Staffing Ratios for Surge Capacity Matrix STAFFING RATIOS FOR SURGE CAPACITY MATRIX I Number of Patients Expected 1 – 10 Patient Care Staff Ratios for RED beds Existing Staff Patient Care Staff Ratios for YELLOW beds Existing Staff Patient Care Staff Ratios for BLACK beds Existing Staff II 11 – 25 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 III 26 – 50 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 IV 51 – 100 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 V >100 1:2 to 1:4 1:5 to 1:12 1:10 to 1:16 Level Worksheet 5-1 Worksheet 6: Transition Matrix TRANSITION MATRIX Beds: First 24 Hours RED Beds: > 24 Hours Critical Care YELLOW Monitored Intermediate Care YELLOW/BLACK Medical/Surgical Care Worksheet 6-1 Worksheet 7: Ancillary Support Matrix ANCILLARY SUPPORT MATRIX I Number of Patients Expected 1 – 10 II 11 – 25 III 26 – 50 IV 51 – 100 V >100 Level Housekeeping Staff for RED rooms Existing Staff Housekeeping Staff for YELLOW rooms Existing Staff Housekeeping Staff for BLACK rooms Existing Staff ANCILLARY SUPPORT MATRIX I Number of Patients Expected 1 – 10 II 11 – 25 III 26 – 50 IV 51 – 100 V >100 Level Food Services Staff for RED rooms Existing Staff Food Services Staff for YELLOW rooms Existing Staff Worksheet 7-1 Food Services Staff for BLACK rooms Existing Staff Worksheet 8: Equipment Location Matrix EQUIPMENT LOCATION MATRIX Surge Area: Critical Equipment Crash carts IV pumps Defibrillators Portable suction Syringe pumps Portable oxygen Ventilators Blood PCA pumps Commodes Privacy Screens Pressure infusers Warming devices Location Worksheet 8-1 Worksheet 9: Equipment Source Matrix EQUIPMENT SOURCE MATRIX Critical Equipment Crash carts IV pumps Defibrillators Portable suction Syringe pumps Portable oxygen Ventilators Blood PCA pumps Commodes Privacy Screens Pressure infusers Warming devices Source Worksheet 9-1 Worksheet 10: Critical Supply Inventory Matrix CRITICAL SUPPLY INVENTORY Maximum Number of RED Patients (X) Maximum Number of YELLOW Patients (X) 10-1 Critical Supply Inventory (X) IV tubing (X) IV start supplies (X) IV fluids (X) medicines (X) bed pans/urinals (X) needles/syringes (X) catheters (X) dressings (X) linens (X) alcohol wipes (X) tape (X) hand sanitizer (X) PPE (X) OB delivery supplies (X) casting supplies Critical Supply Inventory (X) IV tubing (X) IV start supplies (X) IV fluids (X) medicines (X) bed pans/urinals (X) needles/syringes (X) catheters (X) dressings (X) linens (X) alcohol wipes (X) tape (X) hand sanitizer (X) PPE (X) OB delivery supplies (X) casting supplies Maximum Number of BLACK Patients (X) Critical Supply Inventory (X) IV tubing (X) IV start supplies (X) IV fluids (X) medicines (X) bed pans/urinals (X) needles/syringes (X) catheters (X) dressings (X) linens (X) alcohol wipes (X) tape (X) hand sanitizer (X) PPE (X) OB delivery supplies (X) casting supplies Worksheet 10-2 Worksheet 11: Critical Supply Source Matrix SUPPLY SOURCE MATRIX Critical Supplies IV tubing IV start supplies IV fluids Medications Bed pans/urinals Needles/syringes Catheters Dressings Linens Alcohol wipes Tape Hand sanitizer PPE OB delivery supplies Casting supplies Source Worksheet 11-1 Worksheet 12: Alternative Treatment Site Matrix ALTERNATIVE TREATMENT SITE MATRIX Type of Patient/Injury/Illness Pediatric Patients Name and Location of Outpatient Center OB Patients Lacerations Broken Bones Patients in Need of Medical Evaluation Cardiac Symptoms Psychiatry Other Worksheet 12-1