Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacognosy wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Pharmacogenomics wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Atypical antipsychotic wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Norepinephrine wikipedia , lookup
Theralizumab wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Serotonin syndrome wikipedia , lookup
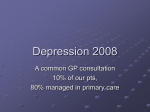
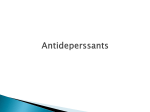
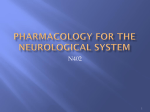
Medications Used for Depression in the Older Adult Jena Ivey Burkhart, PharmD, BCPS, CPP Clinical Assistant Professor, UNC Eshelman School of Pharmacy Geriatric Clinical Pharmacist, UNC Division of Geriatric Medicine [email protected] September 2010 Objectives 1. Describe the mechanism of action of each class of antidepressants 2. Compare and contrast antidepressants with respect to efficacy, safety, and cost 3. Identify appropriate monitoring parameters for antidepressant therapy Treatment of Depression 1. Psychotherapy – cognitive and behavioral 2. Pharmacotherapy – – – – – Tricyclic antidepressants (TCAs) Monoamine oxidase inhibitors (MAOIs) Selective serotonin reuptake inhibitors (SSRIs) Serotonin/norepinephrine reuptake inhibitors (SNRIs) Atypical antidepressants 3. Electroconvulsive therapy (ECT) Challenges of Treatment • Reduced lean body mass, increased body fat affect concentration of drugs • Reduced hepatic and renal drug and metabolite clearance • Presence of medical illness may cause pharmacodynamic changes (e.g. dementia) • Drug-drug interactions Biochemical Changes in Older Adults • Disregulation of CNS involving various neurotransmitters (Limbic system dysfunction) – Decrease in dopamine (DA) and/or 5hydroxytryptamine (5-HT or serotonin) – Decrease in norepinephrine (NE) – Increase in monoamine oxidase (MAO) • Main targets of therapy: 5-HT and NE Neurotransmitter Effects Serotonin Sex Appetite Aggression Norepinephrine Sadness Anxiety Aches and Pain Concentration Attention Motivation Classes of Agents • Tricyclic antidepressants (TCAs) • Monoamine oxidase inhibitors (MAOIs) • Selective serotonin reuptake inhibitors (SSRIs) • Serotonin/norepinephrine reuptake inhibitors (SNRIs) • Atypical antidepressants • Other adjunctive agents TCA – Mechanism of Action www.csusm.edu/DandB/AD.html TCAs • Considered cornerstone of antidepressant therapy for several decades • Classified according to chemical structure • Effectiveness: – major depression – masked depression – pseudodementia • Adverse effects limit use Characteristics of TCAs Drug Mean Dose (mg/day) Half-life (hrs) Anticholinergic Effects Sedation Orthostasis Weight Gain *Amitriptyline 30-100 10-22 +++ +++ +++ ++ *Imipramine 30-100 10-25 ++ ++ +++ ++ *Doxepin 75-150 12-23 ++ +++ +++ ++ *Nortriptyline 25-75 20-50 + ++ + + *Desipramine 30-125 12-24 + + ++ + *Tertiary Amines *Secondary Amines All available as generic Characteristics of TCAs Precautions/Contraindications • Cardiac conduction disturbances • Ischemic heart disease • Existing cognitive dysfunction • Low therapeutic index, potentially fatal in overdose TCAs – Place in Therapy • Potentially severe adverse effects limit use in older adults • All equally effective • May be ideal in certain patient populations for certain indications • Initiate at low dose and titrate to therapeutic effect MAOIs – Mechanism of Action www.csusm.edu/DandB/AD.html MAOIs • Effectiveness: – Depression refractory to TCAs – Depressive phase of bipolar disorder – Atypical depression/anxiety • Adverse effects/potentially serious interactions limit use MAOIs • Available agents – Phenelzine (Nardil®) • dose per day: 15-90 mg – Tranylcypromine (Parnate®) • dose per day: 10-60 mg – Selegiline (Eldepryl®) • dose per day: 5-10 mg • Minimal anticholinergic effects and less sedating as compared to TCAs • Risk of hypertensive crisis when combined with tyramine-containing foods or sympathomimetics All agents available as generic MAOIs • Adverse Effects – sexual dysfunction – mild anticholinergic effects – orthostatic hypotension – sedation (phenelzine) – insomnia (tranylcypromine) • Drug Interactions – – – – – sympathomimetics opiates “tryptans” SNRIs SSRIs MAOIs – Place in Therapy • Not first-line, rarely used • Used in more resistant forms of depression • Adverse effects limit use • Initiate at low dose and titrate to therapeutic effect SSRIs – Mechanism of Action www.csusm.edu/DandB/AD.html Selective Serotonin Reuptake Inhibitors • Equal efficacy when compared to TCAs and to each other • Considered first-line in older adults – favorable adverse effect profiles – once-daily dosing – safety in cases of overdose • Preferred agents for depression complicating cardiovascular and cerebrovascular disease Selective Serotonin Reuptake Inhibitors Drug Starting Dose/Day Daily Dose Range Fluoxetine (Prozac®)* 5-10 mg 5-20 mg Fluvoxamine (Luvox®) 50 mg 100-300 mg Paroxetine (Paxil®, Paxil CR®)* 10-20 mg 20-60 mg Sertraline (Zoloft®)* 25-50 mg 50-150 mg Citalopram (Celexa®)* 10-20 mg 20-40 mg Escitalopram (Lexapro®)* 5-10 mg 10-20 mg *Also available in solution or suspension Available as generic SSRI – Adverse Effects • Gastrointestinal – nausea, vomiting, diarrhea • Sexual dysfunction • Headache • SIADH/hyponatremia • • • • Insomnia Fatigue Agitation Akathesia and dystonic reactions SSRI – Adverse Effects • Most likely to cause sedation – paroxetine, fluvoxamine • Most anticholinergic – paroxetine • Fluoxetine – higher rates of anxiety/nervousness – many drug interactions – long t½ SSRI – Adverse Effects • Fluvoxamine – many drug interactions – only approved for OCD • Sertraline – more diarrhea – may be more activating (do not administer at night) • Citalopram, escitalopram – may be more “neutral” SSRI – Drug Interactions Enzyme Drugs metabolized Antidepressants by enzyme that inhibit enzyme 1A2 theophylline, TCAs, caffeine, haloperidol fluvoxamine 2C9 warfarin, phenytoin, diazepam, TCAs fluvoxamine, fluoxetine, sertraline 2D6 Antipsychotics, TCAs, β-blockers, 1C antiarrhythmics fluoxetine, sertraline, paroxetine 3A4 TCAs, alprazolam, triazolam, cyclosporine, erythromycin fluvoxamine, fluoxetine, sertraline SSRI Withdrawal Syndromes • More likely to occur with short t½ life agents (paroxetine warning) • May be due to sudden decrease in available synaptic 5-HT in face of down-regulated receptors • Onset 24-72 hours and lasts up to 7-14 days • Symptoms: dizziness, nausea, lethargy, headache, parasthesia Serotonin Syndrome • Potentially life-threatening condition associated with increased serotonergic activity in the CNS • Seen with therapeutic medication use, inadvertent interactions between drugs, and intentional selfpoisoning • Anxiety, restlessness, tachycardia, vomiting, diarrhea, tremor, muscle rigidity, hyperreflexia • Need emergent medical care…call 911 SSRIs – Place in Therapy • Considered first-line for depression in older adults • Selection of agent depends on side effect profile • Start at low doses and increase every 2-4 weeks to achieve maximal therapeutic efficacy • Citalopram, escitalopram, sertraline seem to be best tolerated Serotonin/Norepinephrine Reuptake Inhibitors Mechanism of Action • Inhibit both 5-HT and NE reuptake • Weak reuptake inhibition of DA • Degree of neurotransmitter reuptake inhibition dependent on dosing of agent • Available agents – Venlafaxine (Effexor®, Effexor XR®)** – Duloxetine (Cymbalta®) – Desvenlafaxine (Pristiq®) **Venlafaxine immediate release (BID dosing) is only SNRI with generic availability] **Recently approved Venlafaxine ER but is not pharmaceutical equivalent to Effexor XR, only costs about 20% less, 225 mg strength available Serotonin/Norepinephrine Reuptake Inhibitors • Dosing – Venlafaxine: 37.5 mg-75 mg up to 375 mg daily (no more than 225 mg/day extended release) • enhanced response on NE with increasing doses – Duloxetine: 20 mg up to 60 mg daily • equal 5HT/NE reuptake inhibition at lower and higher doses – Desvenlafaxine: 50 mg daily (doses higher than this have little efficacy, more side effects) • Prodrug of venlafaxine • Use SNRIs for those who have not responded to appropriate trials of other antidepressant agents SNRI – Adverse Effects • • • • • Nausea Constipation Headache Dizziness Nervousness • • • • Somnolence Dry mouth Sexual dysfunction Increased seizure risk • Increased BP* Atypical Antidepressants • Mirtazapine* (Remeron®) – 5-HT2/5-HT3 blockade, histamine-1 blockade – little activity on alpha1, muscarinic, DA • Trazodone* (Desyrel®) – specific inhibitor of 5-HT reuptake – α-adrenergic blockade • Bupropion* (Wellbutrin®, Wellbutrin SR®, Wellbutrin XL®) – weak inhibitor of 5-HT, NE, and DA *Available as generic Mirtazapine (Remeron®) • Dosing: 15 mg up to 45 mg daily, usually at bedtime • More sedating at lower doses • Side effects (decreased frequency reported at higher doses) – – – – sedation appetite stimulation/weight gain dry mouth constipation • May be optimal agent for depression accompanied by insomnia, weight loss Trazodone (Desyrel®) • Dosing (depression): 100 mg up to 600 mg daily – Used infrequently for depression due to side effects at higher doses • Dosing (insomnia): 25 mg up to 100 mg daily, dosed at bedtime • Side effects – sedation (drug of choice for insomnia in the elderly) – Orthostasis, bradycardia, hypotension • Dose titration every 2-3 days may be necessary to achieve adequate response Bupropion (Wellbutrin®) • Dosing: 75 mg up to 150 mg daily, XL forms • Appears well tolerated but limited data available in older adults • May be good agent for apathetic depression, augmenting agent • Used in smoking cessation (Zyban®) • Side effects – – – – – – insomnia increases seizure risk agitation constipation weight loss NO sexual dysfunction Other Adjunctive Agents • May augment response to antidepressants for specific target symptoms • Stimulants – Methylphenidate (Ritalin®) – Modafinil (Provigil®) • Mood stabilizers – Carbamazepine – Lithium • Antipsychotics – approved for resistant depression (last line option) Choosing an Antidepressant • All equally effective • Limited clinical data in older adults • Patient characteristics • Prior response • • • • Side effect profile Drug interactions Cost Adherence Monitoring Parameters • Week 1 – anxiety – insomnia – appetite • Week 2-3 – increase in energy – increase suicide risk – increase in libido • Up to 4-8 weeks – improvement in dysphoria or sadness – improvement in pessimism – improvement in anhedonia *If response not adequate, may need to modify initial therapy Summary of Antidepressant Therapy in Older Adults • Start low and go slow • At least 6-8 weeks of treatment recommended to achieve optimal effect • Older patients may take longer to respond • Achieving effective doses important Summary of Antidepressant Therapy in Older Adults • Monitoring for response/adverse effects key • Continuation of therapy – Treat initial episode at least 9-12 months – If relapse when therapy discontinued, may need treatment for life