Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
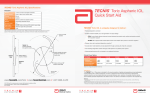
Getting Started GUIDE LEAVE A LEGACY OF EXCELLENT OUTCOMES FOR PATIENTS WITH ASTIGMATISM. TECNIS® TORIC 1-PIECE IOL pg 1 GETTING STARTED WITH THE TECNIS® TORIC IOL TECNIS® TORIC IOL AT A GLANCE The IOL you leave behind is the quality of vision your patients take with them. Use this guide to support optimal toric calculation and insertion, and leave a legacy of excellent outcomes for your patients with astigmatism. Designed for outstanding optical quality, the TECNIS® Toric IOL delivers the sharpest vision, best low-light performance and long-term sustainability. 13.0 mm overall diameter IN THIS GUIDE LENS SPECIFICATIONS pg 3 TECNIS® Toric IOL at a Glance CALCULATION pg 4 Calculate Proper Cylinder Power SURGERY pg 6 Pearls for Optimizing Toric IOL Outcomes Anterior cylinder axis marks denote IOL meridian with lowest power TECNIS® IOL wavefront-designed toric aspheric surface Frosted, continuous 360° posterior square edge Anterior Side Haptics offset for 3 points of fixation Posterior Side PATIENT EDUCATION pg 8 Help Your Patients Understand the Benefits and Risks RESOURCES AND SUPPORT pg 9 Committed to Your Legacy 6.0 mm optic diameter TECHNICAL SPECIFICATIONS pg 10 INDICATIONS AND IMPORTANT SAFETY INFORMATION pg 11 pg 2 TECNIS® TORIC 1-PIECE IOL INDICATIONS: The TECNIS® Toric 1-Piece Posterior Chamber Lens is indicated for the visual correction of aphakia and pre-existing corneal astigmatism of one diopter or greater in adult patients with or without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire improved uncorrected distance vision, reduction in residual refractive cylinder, and increased spectacle independence for distance vision. The device is intended to be placed in the capsular bag. See Important Safety Information on page 11. TECNIS® TORIC 1-PIECE IOL pg 3 CALCULATION Calculate the Proper Cylinder Power for the TECNIS® Toric IOL TECNIS® TORIC IOL AT A GLANCE QUESTIONS & ANSWERS How is the cylinder calculated? Why is the sphere not displayed in the results section? The calculator uses the Holladay 1 formula for calculation of the cylinder. If you prefer to enter another IOL constant, the system will convert it. As the sphere is calculated outside of the toric calculator, please refer to the printout of your biometry device. Why do I need to enter the axial length? In contrast to other online calculators, the TECNIS Toric Calculator uses axial length for high accuracy of the calculation.1 How does the TECNIS Toric Calculator compare to other online calculators? Why are three lens models displayed instead of the most suitable IOL model only? The choice of three IOLs should help to select the lens power that is most suitable for each individual patient. The calculator will provide options for the amount of residual cylinder based on your choice for an individualized patient outcome. This may include a choice of flipping the axis in order to achieve a lower amount of residual cylinder. Most toric calculators use an approximation method rather than the exact solution, using a constant for the ratio of the IOL toricity to corneal astigmatism. This approximation can cause errors. Please be aware that the more a patient’s ocular parameters vary from normal, the more important it is to use the exact, rather than the approximation, solution used by other calculators. For instance, if the residual astigmatism does not change when the calculation is run for 10 D and 22 D IOLs, then the calculator is using the approximation method.1 How should I calculate SIA? Choose your preferred IOL constant and value Enter the spherical equivalent (as calculated with your biometry device) Reminder: How to print this page for surgical planning pg 4 TECNIS® TORIC 1-PIECE IOL Make sure to select the correct corneal index for your keratometer if you have entered your K-readings in diopters Select the IOL model based on the residual cylinder and axis Preselect your preferred units: Please refer to sia-calculator.com. NOTE If you enter the K-readings in mm, the keratometer index is not used in the calculation; however, the TECNIS Toric Calculator requires that you select a value. If you enter the K-readings in diopters, the calculator requires and uses the appropriate keratometer index for the calculation. Format of date and decimal layout Select to display results as plus or minus cylinder Select K-notation input unit as diopters or millimeters PRECAUTIONS: The use of methods other than the TECNIS Toric Calculator to select cylinder power and appropriate axis of implantation were not assessed in the clinical study and may not yield similar results. Accurate keratometry and biometry in addition to the use of the TECNIS Toric Calculator (www.TecnisToricCalc.com) are recommended to achieve optimal visual outcomes. The TECNIS Toric Calculator incorporates the surgeon’s estimated SIA and incision location when providing IOL options. 1.Holladay JT. Improving toric IOL outcomes. Ocular Surgery News. May 25 and June 10, 2011. TECNIS® TORIC 1-PIECE IOL pg 5 SURGERY Clinical Pearls for Optimizing Toric IOL Outcomes Provided by Daniel Chang, MD 1. CORNEAL MARKING Mark the steep corneal axis clearly and accurately • In order to identify specific iris structures, reference the measured steep axis to a preoperative pupil image • Under the guidance of a slit lamp or surgical microscope, place precise intrastromal arcuate incisions with a laser or mark the eye with ink 2. OPENING STEPS Ensure proper wound construction • Whether using a femtosecond laser or a blade, construct a triplanar incision that will seal well at the end of a case • Create a well-centered capsulotomy that can provide 360° of capsular overlap, which may help limit asymmetric capsular forces on the IOL postoperatively 3. IOL UNFOLDING AND POSITIONING Take time for optimal unfolding • Prime the IOL injection cartridge and inflate the capsular bag using a cohesive viscoelastic • Allow ample time for the IOL to unfold — depending on OR temperature, this may take 30–40 seconds • Rotate the IOL in the bag several times, even before unfolding is complete, to ensure the haptics are fully deployed into the capsular fornix and to help loosen any remaining cortical material pg 6 TECNIS® TORIC 1-PIECE IOL – Rotating the lens while it is unfolding eliminates the need to warm the IOL and/or OVD to facilitate faster unfolding, allowing you to utilize the time for proper positioning instead – Occasionally, it may be necessary to assist the haptics in unfolding • Scrape the posterior aspect of the anterior capsular rim to remove lens epithelial cells – Though some surgeons suggest skipping this step to promote stability through adhesion of the capsule to the optic, this may result in capsular fibrosis due to retained lens epithelial cells •O nce the IOL has completely unfolded, align the marks on the IOL with the corneal marks placed on the steep meridian • To help with centration and address the problem of parallax, have the patient fixate on a coaxial light source 4. OVD REMOVAL Completely remove OVD under the IOL •T o help remove the viscoelastic from the poster chamber and from behind the IOL, rotate the IOL and press slightly posteriorly while irrigating and aspirating •A s an extra step, place the I/A hand piece behind the IOL to ensure complete OVD removal 5. IOL AND WOUND CHECK Ensure optimal positioning and pressure •A fter the IOL is rotated into position, lightly press it onto the posterior capsule to help hold it into position •P erform initial wound hydration prior to final IOL positioning •O nce the lens in in position, take care not to induce any IOL movement during subsequent wound hydrations by applying only mild-to-moderate pressure when injecting – To maintain physiologic pressure, meticulously check the wounds for leakage – When performing the check, dry the wound to find any slow leaks and press on the globe to simulate an eye rub •W hen in doubt, do not hesitate to close the wound with a suture 6. FINAL CHECK OF LENS POSITIONING Secure IOL position for outstanding outcomes •T o minimize intraocular turbulence or hyperinflation, inject tangentially to the wound • At the end of the case, check for any IOL movement by having the patient look up, down, left and right •B ring the eye to physiologic pressure, taking care not to hyperinflate • After removing the speculum and drape, perform a final check to ensure the IOL has not moved or shifted, ensuring the patient leaves the operating room with the IOL in an optimal position – Postoperative hypotony likely plays a major role in IOL rotation – A hypotonous eye can compress easily with blinking or eye rubbing, and a gross deformation of the globe could cause a shift in IOL positions • Place an eye shield and instruct the patient not to rub his or her eye after surgery AMO does not engage in the practice of medicine, and Dr. Chang’s clinical tips are not a substitute for appropriate medical education and training or for the exercise of independent medical judgment. AMO cannot warrant the accuracy or completeness of information contained within this document. AMO does not endorse or recommend any particular technique beyond what is contained in the product labeling, and other techniques may be appropriate in a physician’s medical judgment. TECNIS® TORIC 1-PIECE IOL pg 7 PATIENT EDUCATION RESOURCES AND SUPPORT Help Your Patients Understand the Benefits and Risks of a TECNIS® Toric 1-Piece IOL • Tell your patients about the convenience of one procedure to both eliminate their cataracts and correct their astigmatism • Explain to your patients that careful calculations have been performed to choose the optimal lens power for their eye, but: Committed To Your Legacy VISIT TECNISIOL.COM FOR ADDITIONAL RESOURCES SIMULATED VISION Cataracts and astigmatism create cloudy and blurred vision. • Optimizing Toric IOL Outcomes video with Daniel Chang, MD • Toric calculator •V ision simulator - They may still need glasses for reading and distance vision after surgery • Brochure - In rare cases, the lens might change its position after surgery and a second intervention might be needed for realignment • Directions for use - In case of increasing blurred vision after surgery, they need to contact you or at least let the referring doctor know that they have received a toric lens ATTENTION: Reference the Directions for Use for a complete listing of indications, warnings, precautions and safety information. • Spec sheet Even after the cataract is removed, the astigmatism will still cause blurred vision. •P romotional tools For support, contact your Abbott representative or call 1-800-366-6554. • Explain the potential risks of cataract surgery and lens replacement, including worsening of vision, bleeding or infection • Let your patients know they should contact you if they experience itching, redness, pain, “floaters,” flashing lights, severe headache, light sensitivity or watery eyes after the surgery • Tell your patients the side effects specific to the TECNIS® Toric Lens, including the potential need for secondary surgical intervention to replace the lens or repair the eye, macular edema and retinal detachment pg 8 TECNIS® TORIC 1-PIECE IOL With the TECNIS® Toric IOL, you may have less dependence on glasses for distance vision. TECNIS® TORIC 1-PIECE IOL pg 9 TECHNICAL SPECIFICATIONS INDICATIONS AND IMPORTANT SAFETY INFORMATION FOR THE TECNIS® TORIC 1-PIECE IOL CAUTION: Federal law restricts this device to sale by or on the order of a physician. TECNIS® Toric Aspheric IOL Specifications Powers +5.0 D to +34.0 D in 0.5 diopter increments Cylinder Powers 1.50 D, 2.25 D, 3.00 D, 4.00 D, 4.50 D, 5.25 D, 6.00 D Diameter 6.0 mm Optic Overall Length 13.0 mm Shape Biconvex, anterior toric aspheric surface Material UV-blocking hydrophobic acrylic Refractive Index 1.47 INDICATIONS: The TECNIS® Toric 1-Piece Posterior Chamber Lens is indicated for the visual correction of aphakia and pre-existing corneal astigmatism of one diopter or greater in adult patients with or without presbyopia in whom a cataractous lens has been removed by phacoemulsification and who desire improved uncorrected distance vision, reduction in residual refractive cylinder, and increased spectacle independence for distance vision. The device is intended to be placed in the capsular bag. WARNINGS: Physicians considering lens implantation should weigh the potential risk/benefit ratio for any circumstances described in the TECNIS® Toric 1-Piece IOL Directions for Use that could increase complications or impact patient outcomes. The clinical study did not show evidence of effectiveness for the treatment of preoperative corneal astigmatism of less than one diopter. The TECNIS® Toric 1-Piece IOL should not be placed in the ciliary sulcus. Rotation of the TECNIS® Toric 1-Piece IOL away from its intended axis can reduce its astigmatic correction. Misalignment greater than 30° may increase postoperative refractive cylinder. Edge Design ProTEC continuous 360° posterior, frosted square edge Haptic Design Offset from optic with 3-point fixation A-constants 119.3* (Optical Biometry) 118.8† (Ultrasound Biometry) PRECAUTIONS: Accurate keratometry and biometry in addition to the use of the TECNIS Toric Calculator (www.TecnisToricCalc.com) are recommended to achieve optimal visual outcomes. The safety and effectiveness of the toric intraocular lens have not been substantiated in patients with certain preexisting ocular conditions and intraoperative complications. Refer to the TECNIS® Toric 1-Piece IOL Directions for Use for a complete description of the preexisting conditions and intraoperative complications. All preoperative surgical parameters are important when choosing a toric lens for implantation. Variability in any of the preoperative measurements can influence patient outcomes. All corneal incisions were placed temporally in the clinical study. Do not reuse, resterilize, or autoclave. *Derived from clinical evaluation results of the TECNIS® 1-Piece Platform. † Value theoretically derived for a typical 20.0 D lens. Abbott Medical Optics recommends that surgeons personalize their A-constant based on their surgical techniques and equipment, experience with the lens model and postoperative results. ADVERSE EVENTS: The most frequently reported cumulative adverse event that occurred during the TECNIS® Toric 1-Piece IOL clinical trial was surgical re-intervention which occurred at a rate of 3.4% (lens repositioning procedures and retinal repair procedures). Cylinder Power Options Lens Model ZCT150 ZCT225 ZCT300 ZCT400 ZCT450 ZCT525 ZCT600 Cylinder Powers IOL Plane 1.50 D 2.25 D 3.00 D 4.00 D 4.50 D 5.25 D 6.00 D Corneal Plane* 1.03 D 1.54 D 2.06 D 2.74 D 3.08 D 3.60 D 4.11 D Corneal Astigmatism Correction Range† (Preop Kcyl+SIA) 0.75 – 1.50 D 1.50 – 2.00 D 2.00 – 2.75 D 2.75 – 3.62 D 3.00 – 3.50 D 3.50 – 4.00 D 4.00 – 4.75 D *Based on average pseudophakic human eye. † Based on a vector sum of preoperative corneal astigmatism (preop Kcyl) and the predicted effect of surgically induced astigmatism (SIA). pg 10 TECNIS® TORIC 1-PIECE IOL TECNIS® TORIC 1-PIECE IOL pg 11 TECNIS and ProTEC are trademarks owned by or licensed to Abbott Laboratories, its subsidiaries, or affiliates. All other trademarks and tradenames are the intellectual property of their respective owners. ©2015 Abbott Medical Optics Inc. | www.AbbottMedicalOptics.com | PP2015CT0789 Reorder: TEC15-19