Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
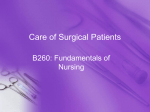
ARTICLE Clinical assessment of defocus curves after Excimer Laser presbyopia surgery using aspheric ablation profiles Marta Romero-Domínguez, MD1; Alfredo Castillo-Gómez, MD, PhD1; David Carmona-González, OD1; Carlos Palomino Bautista, MD1 PURPOSE: To assess binocular visual acuity (VA) through the evaluation of defocus curves in patients who underwent correction of spherical aberration and micro-monovision using PRESBYOND Laser Blended Vision (Carl Zeiss Meditec). SETTING: Universidad Europea de Madrid, Madrid, Spain. METHODS: A prospective study of 80 eyes from 40 patients that underwent PresbyLASIK surgery. Patients were divided into 2 groups according to their preoperative spherical equivalent (SE): group I (range +0.5 to +3 diopters (D) and group II (range −0.75 to −5.5 D). Refractive changes, uncorrected distance and near VA (UDVA and UNVA, respectively), and independence from glasses were assessed. RESULTS: Mean age of patients was 47.75 ± 4.38 years. Defocus curve of group I showed pre- and post-operative UDVA of 0 logMAR, while intermediate visual acuity (IVA) at 67 cm was 0.10 to 0.09 logMAR, and at 33 cm VA increased from 0.47 to 0.41 logMAR. Pre- and post-operate UDVA in group II was 0 logMAR, while for IVA it decreased from 0.06 to 0.11 logMAR, and at 33 cm it decreased from 0.34 to 0.44 logMAR. Independence from distance spectacles was achieved by 100% of patients in both groups, whilst 91.4% of group I and 61.7% of group II achieved independence from near spectacles. CONCLUSION: PresbyLASIK treatment is effective for both myopic and hyperopic patients because it reduces presbyopia symptoms and corrects distance refractive error in the same procedure, thus offering greater independence from spectacles. Defocus curves provide a useful method to assess visual capability after refractive surgery. J Emmetropia 2016; 1: 39-45 Presbyopia is a reduction in the focusing power of the eye, which loses the ability to focus on near objects. It is estimated that presbyopia currently affects around 1 million adults worldwide. As the world population becomes older, presbyopia prevalence will increase. By 2030, the world population aged 40 years or over is expected to increase by up to 41%1-2. Monovision was initially used in optometry as a means to adapt contact lens for the treatment of presbyopia3 (the original term used was “single vision”). Submitted: 10/13/2015 Revised: 1/28/2016 Accepted: 2/17/2016 1 Hospital Universitario Quirónsalud, Madrid, Spain. Financial Disclosure: The authors declare no conflict of interest. No financial support was received for this study. Corresponding Author: Marta Romero-Domínguez Calle Diego de Velazquez 1. 28223 Pozuelo de Alarcón. Spain E-mail: [email protected] © 2016 SECOIR Sociedad Española de Cirugía Ocular Implanto-Refractiva In the 1980s, as a result of advances in crystalline surgery, combined vision became more common as a means to improve both distance and near and intermediate vision for patients who underwent cataract surgery or refractive lensectomy. With the incorporation of excimer laser technology to ophthalmology in the 1990s, multifocal profiles started to be developed to correct presbyopia4. Monovision, with or without modification of corneal asphericity5, was also incorporated as a treatment option for presbyopia (LASIK-monovision or Blended Vision6). There are also other techniques for the correction of presbyopia: multifocal lens, accommodating lens, femtosecond laser7 or intracorneal implant8,9. Defocus curves are graphic tools that assess visual performance after refractive surgery by measuring VA at varying distances with 2 peaks of optimum acuity: 1 at the distance focal point and the other at the near focus. They are mostly used in refractive corneal surgery to correct presbyopia, in contact lens fittings (multifocal), to calculate amplitude of accommodation10 or in the implantation of multifocal intraocular lens11-13. ISSN: 2171-4703 39 40 DEFOCUS CURVES AFTER PRESBYOPIA SURGERY We present an observational, prospective study to evaluate defocus curves before and after presbyopia treatment with Excimer laser that included correction of spherical aberration and micro-monovision. METHODS The prospective study included 80 eyes of 40 patients between 40 and 55 years of age who underwent presbyopia corrective surgery with MEL-80 excimer laser (Presbyond, Carl Zeiss Meditec, Jena, Germany) at the Hospital Universitario Quirón in Madrid, between January and December 2014. The study followed the principles outlined in the Declaration of Helsinki. Prior to surgery, all participants signed an informed consent form outlining the risks, complications and surgical technique used. The inclusion criteria were: between 40 and 55 years of age, manifest symptoms of presbyopia and absence of cataract. The exclusion criteria included: altered topography, contraindicated for LASIK treatment, clouding of the crystalline lens, absence of symptoms of presbyopia, corneal disease, glaucoma, retinopathy or macular degeneration, previous history of ocular inflammation, and previous corneal or intraocular surgery. Patients were divided into 2 groups according to their preoperative spherical equivalent (SE): group I (range +0.5 to +3 diopters [D]) and group II (range −0.75 to −5.5 D). Preoperative workup consisted of a complete ophthalmic exam that included: binocular best uncorrected distance visual acuity (UDVA), binocular corrected near visual acuity (CNVA), binocular uncorrected near visual acuity (UNVA), autokeratometer measurements (TopCon Corporation, Tokyo Japan), subjective and cyclopegic refraction, applanation tonometry, slit lamp exam, funduscopy with pupil dilated, corneal topography (Pentacam Oculus, Germany), ultrasonic pachymetry (DGH Technology, Inc., United States), ocular dominance test, anisometropia tolerance test using test frames, and CRS-MASTER with H-S aberrometer (Wasca Analyzer), iris registration and corneal anterior surface topographer (ATLAS 9000). Motor ocular dominance was determined using the hole-in-card test. Sensory ocular dominance was determined using the plus 1 D test or swinging-plus test (can also be used for near eyes). These tests were followed by an anisometropia tolerance test using test frames. The correct prescription was set on the dominant eye, while the non-dominant eye in myopic patients was undercorrected within a range of 0.75 D and 1.5 D, and overcorrected within the same range in hyperopic patients. Testing started with the minimum possible overcorrection (0.75 D) in the non-dominant eye (having already set the correct ranking for the dominant eye). The test must always be binocular. The adaptation of the patient is checked after a period of 20-30 minutes. Graduation in the non-dominant eye is gradually increased to a maximum of 1.5 D, until comfortable binocular distance and near vision was achieved. Binocular defocus curves, constructed using vergence ranges between −5.00 D and +3.00 D spherical, in 0.50 D steps, were obtained for all patients preoperatively and 6 months after surgery. Three points were analyzed on the defocus curves: 1 corresponding to the infinite or distance vision (DV), 1 at 67 cm for intermediate visual acuity (IVA) and B 1 at 33 cm for near vision (NV). MEL-80 excimer laser (Presbyond) has a complex wavefront guided laser ablation profile that expands the depth of focus available to each eye. So, while adaptation is similar to micro-monovision, the expanded depth of field achieves a wider range of focus, thus reducing dependence on spectacles as far as possible. Surgical planning with the system includes inputting the functional age of the patient’s eye (this refers to the patient’s actual amplitude of accommodation). The system calculates and programs the spherical aberration (SA) (in Malacara nomenclature14) to be corrected taking into account each patient’s preoperative SE: a) in hyperopic patients: the same SA obtained by the aberrometer; b) in myopic patients: programmed according to the patient’s preoperative SE to a maximum of −0.8 (this is the maximum value that can be applied). The aberration correction is bilateral and symmetrical, together with the residual myopia previously calculated. Follow-up examinations were set at 1 day, 1 week and 1, 3 and 6 months after surgery. The following were assessed: binocular UDVA, BCDVA, CNVA, UNVA, dominant and non-dominant eye refraction, defocus curves and topography. A slit lamp exam was also carried out. Results are expressed as mean ± standard deviation. Data were analyzed using IBM SPSS Statistics for Windows, Version 21.0 (Armonk, NY: IBM Corp.). The Wilconxon test was used to compare pre- and postoperative data for each group, and to assess the relevance of pre- and post-surgery differences within each group. The non-parametric Mann-Whitney U test was used to compare the differences between 2 independent groups. Statistical significance was set at a p-value of less than 0.05. JOURNAL OF EMMETROPIA - VOL 7, JANUARY-MARCH 41 DEFOCUS CURVES AFTER PRESBYOPIA SURGERY Table 1. Demographic characteristics and preoperative data. Parameter Patients (n) Age, years (mean ± SD) Sex (male / female) Eyes (n) Preoperative spherical equivalent (D) Value 40 47.75 ± 4.38 16 / 24 80 Group I Group II mean ± SD range mean ± SD range 1.31 ± 0.83 +0.50 to +3 −3.46 ± 1.37 −1 to −5.50 mean ± SD range mean ± SD range −0.98 ± 1.32 −0.25 to −4.50 −1.01 ± 0.51 0.25 to −2.50 42.68 ± 1.75 44.12 ± 1.91 Preoperative cylinder (D) Group I Group II Preop keratometry. k1 (D ± SD) Preop keratometry. k2 (D ± SD) Overcorrected nondominant eye Eyes (n) +0.75 D +1 D +1.25 D +1.75 D 12 32 16 20 n= sample size, SD= standard deviation. Table 2. Comparison of pre- and postoperative spherical equivalent (SE). Mean ± SD (range) GROUP I GROUP II PRE-OP SE POST-OP SE (dominant eye) POST-OP SE (non-dominant eye) 1.31 ± 0.83 (+0.50 to +3) −3.46 ± 1.37 (−1 to −5.50) 0.17 ± 0.56 (0.75 to −1) −0.14 ± 0.23 (0.13 to −0.88) −0.89 ± 0.18 (−0.23 to −1.03) −1.05 ± 0.35 (−0.75 to −1.63) SE = spherical equivalent; OP = operative. RESULTS A total of 80 eyes of 40 patients were operated. Average age was 47.75 ± 4.38 years (range 41-55). There were 24 women (60%) and 16 men (40%). The mean preoperative SE of group I was +1.31 ± 0.83 D (range +0.5 D to +3 D), while that of group II was −3.46 ± 1.37 D (range −1 D to −5.50 D). Mean preoperative astigmatism of group I was −0.98 ± 1.32 D (range −0.25 D to 4.50 D) and that of group II was −1.01 ± 0.51 D (range 0.25 D to −2.50 D). Mean preoperative astigmatism axis of group I was 91.92 ± 45.49 (range 5° to 170°) and that of group II was 88.70 ± 47.77 (range 10° to 170°). Overcorrection of patients’ non-dominant eyes was as follows: 6 patients (15%) tolerated an overcorrection of 0.75 D, 16 (40%) tolerated 1 D, 8 (20%) tolerated 1.25 D, and 10 (25%) tolerated 1.50 D (Table 1). The mean postoperative SE of group I was +0.17 ± 0.56 D (range 0.75 D to −1 D) in dominant eye and −0.89 ± 0.18 D (range −0.23 D to −1.03 D) in non-dominant eye, while that of group II was −0.14 ± 0.23 D (range +0.13 D to −0.88 D) in dominant eye and −1.05 ± 0.35 D (range −0.75 D to −1.63 D) in non-dominant eye (Table 2). Mean astigmatism at 6 months was −0.62 ± −0.40 D (range −0.25 D to −1.25 D) in group I, and −0.49 ± 0.27 D (range 0.12 D to −0.75 D) in group II. Mean postoperative astigmatism axis of group I was 96.69 ± 37.81 (range 25° to 170°) and that of group II was 111.16 ± 50.32 (range 33° to −180°). At 6 months after surgery in group I, 12 eyes had againstthe-rule astigmatism (corrector cylinder between 80° and 100°) and only 1 eye with-the-rule astigmatism (170°). In group II, 10 eyes had against-the-rule astigmatism JOURNAL OF EMMETROPIA - VOL 7, JANUARY-MARCH 42 DEFOCUS CURVES AFTER PRESBYOPIA SURGERY Table 3. Visual acuity (logMAR) obtained preoperatively and at 6 months after surgery. PREOPERATIVE UDVA POSTOPERATIVE UDVA DISTANCE GROUP I GROUP II GROUP I GROUP II p-value* Infinite 0.00 ± 0.00 0.00 ± 0.00 0.00 ± 0.00 0.00 ± 0.00 - 2m 0.01 ± 0.01 0.00 ± 0.00 0.00 ± 0.00 0.00 ± 0.01 - 1m 0.03 ± 0.06 0.01 ± 0.01 0.03 ± 0.03 0.04 ± 0.04 - 67 cm 0.10 ± 0.14 0.06 ± 0.06 0.09 ± 0.04 0.11 ± 0.06 0.012 50 cm 0.20 ± 0.21 0.14 ± 0.12 0.19 ± 0.06 0.19 ± 0.09 - 40 cm 0.32 ± 0.24 0.22 ± 0.21 0.30 ± 0.12 0.34 ± 0.11 - 33 cm 0.47 ± 0.26 0.34 ± 0.29 0.41 ± 0.13 0.44 ± 0.19 0.023 29 cm 0.63 ± 0.25 0.45 ± 0.29 0.59 ± 0.20 0.55 ± 0.22 - 25 cm 0.82 ± 0.19 0.57 ± 0.30 0.71 ± 0.21 0.74 ± 0.28 - 22 cm 0.93 ± 0.23 0.66 ± 0.38 0.83 ± 0.15 0.88 ± 0.24 - 20 cm 1.08 ± 0.18 0.78 ± 0.35 0.97 ± 0.16 1.07 ± 0.18 0.011 UDVA = binocular best uncorrected distance visual acuity. Values given as mean ± standard deviation; *p-value indicated when significant differences present. Postop Preop 1.00 0.80 0.60 0.40 0.20 Postop Visual Acuity (logMAR) Preop 1.20 0.80 0.60 0.40 0.20 0.00 -5 -4.5 -4 -3.5 -3 -2.5 -2 -1.5 20 cm 22 cm 25 cm 29 cm 33 cm 40 cm 50 cm 67 cm -1 1m -0.5 2m -0.20 0 ь 1.00 Visual Acuity (logMAR) 1.20 0.00 -5 -4.5 -4 -3.5 -3 -2.5 -2 -1.5 20 cm 22 cm 25 cm 29 cm 33 cm 40 cm 50 cm 67 cm -1 1m -0.5 2m -0.20 0 ь Figure 1. Pre and postoperative defocus curves in group 1. Figure 2. Pre and postoperative defocus curves in group 2. (corrector cylinder between 65° and 105°) and 6 eyes with-the-rule astigmatism (corrector cylinder between 155° and 180°). Residual myopia in the non-dominant eyes was higher in group II (−1.05 ± 0.35 D) than in group I (−0.89 ± 0.18 D). The preoperative SA obtained using OSA nomenclature (Optical Society of America) for a 6 mm pupil in group I was 0.22; at 6 months it was 0.04. In group II, SA changed from 0.14 to 0.18 at 6 months. Three points were analyzed on each defocus curve: 1 corresponding to the infinite or distance vision (DV), 1 at 67 cm for intermediate visual acuity (IVA), and 1 at 33 cm for near vision (NV) (Table 3). Defocus curves of group I showed pre- and postoperative UDVA of 0 log of the minimum angle of resolution (logMAR) (20/20), while for IVA at 67 cm it changed from 0.10 to 0.09 logMAR (20/32 to 20/25), and at 33 cm VA increased from 0.47 to 0.41 logMAR (20/60 to 20/50) (Figure 1). Pre- and post-operate UDVA in group II was 0 logMAR (20/20), while for IVA at 67 cm it decreased from 0.06 to 0.11 logMAR (20/25), and at 33 cm, it decreased from 0.34 to 0.44 logMAR (20/45 to 20/55) (Figure 2). JOURNAL OF EMMETROPIA - VOL 7, JANUARY-MARCH DEFOCUS CURVES AFTER PRESBYOPIA SURGERY Postoperative defocus curve of group I showed an overall improvement across the range of distances from 2 m to 20 cm, with the most significant improvement observed at 25 cm (29.89%) and the least significant observed at 2 m (1.35%). This is because preoperative VA was maintained at practically the same value. UDVA of 0 logMAR was maintained, while for IVA at 67 cm there was a 15.69% improvement, and for NV at 33 cm a 15.69% improvement was observed. Postoperative defocus curve of group II showed an overall decrease in vision across the range of distances from 2 m to 20 cm, though maintaining a postoperative distance VA of 0 logMAR. The most significant change in postoperative VA was observed at 20 cm, with VA decreasing an average of 39.77% (0.78 to 1.07 logMAR) (p = 0.011). VA decreased postoperatively an average of 11.49% at 67 cm (0.06 to 0.11 logMAR) (p = 0.012) and 20.65% at 33 cm (0.34 to 0.44 logMAR) (p = 0.023). None of the operated eyes required a second intervention to modify the refractive results obtained. There were no complications during or after any of the surgeries performed. All of the patients (100%) in both groups achieved complete independence from distance spectacles, while 91.4% of patients in group I and 61.7% of patients in group II achieved complete independence from near spectacles. DISCUSSION Defocus curves are a graphic tool used to evaluate a patient’s visual performance at various distances in order to establish a connection between those distances and visual acuity. As mentioned above, they are an excellent way of assessing range of vision after surgical procedures, mainly after presbyopia corrective surgery. Most studies that use spherical lenses to construct defocus curves employ ranges between −5 D and +3 D spherical, although many different ranges are described in the literature13,15. The step size may vary from 0.25 D to 0.75 D or higher. However, increasing the step size may distort the results and affect their validity16. Thus, a step size of 0.50 D or 0.75 D across vergence ranges is generally preferred. Our study used 0.50 D steps and vergence ranges between −5 D and +3 D. Points discussed in the defocus curves differ between authors13,17. For intermediate visual acuity, the distance varies from 63, 64 or 67 cm. For near vision, the distance varies from 33 to 40 cm. We analyzed 1 point at 67 cm for intermediate visual acuity, and 1 at 33 cm for near vision. These points are the most widely used in the literature. According to the refractive results obtained, emmetropia was almost achieved in all dominant eyes, 43 with a postoperative SE of 0.17 ± 0.56 D in group I and −0.14 ± 0.23 D in group II. These results coincide with those reported by other authors, such as Baudu et al.18, who achieved a postoperative SE of +0.17 ± 0.34 D in the dominant eye. Pre-programming the correction of spherical aberration during surgery is also important when aiming to achieve successful refractive outcomes, since it extends depth of focus by increasing the axial defocus range. The higher the spherical aberration induced, the greater the depth of focus generated, although sensibility to contrast will be affected as a result. Consequently, adherence to the nomograms provided by the manufacturer is essential in order to avoid unexpected results. After LASIK surgery, increased higher-order aberrations, primarily, an increase of SA, and to a lesser extent, coma or astigmatism, irregularities induced by treatment or ablationn offset pattern are observed. This increase in SA is directly related to loss of compensation between the SA of the cornea and crystalline lens. The corneal photoablation generates a quasi-spherical cornea and even oblate (Q > 0). The myopic correction induces positive SA, and the hyperopic induces negative SA19. Some studies have demonstrated that negative SA correlated well with improved near performance20. The vertical coma and other aberrations could hinder near visual acuity and patient satisfaction. Decentered ablations on SA could reduce the effectiveness of aspheric shape design and induce coma. With the modification of the SA-inducing treatment used, we reduced SA in hyperopic eyes (0.2 to 0.04), while the increase in myopic eyes was less significant (from 0.14 to 0.18) than if they were treated without control of SA, in which case the increase in myopic eyes after surgery would be much greater. Reinstein et al.21, in emmetropic patients, achieved a change in SA from 0.14 to −0.08 (in OSA), much more striking than that obtained in our study in either group; however, the study was conducted in emmetropic patients. We found some differences in inclusion age between ours and previous studies. Luger et al.22 included patients within an age range of 51 ± 3, while the average age in Reinstein’s21 study was 55, with an age range of 44 and 65 (in another study by Reinstein23, average age was 56, with range of 44 and 66). The age range in Falcon24 et al. was between 42 and 69. In contrast, the age range in our study was inferior to that in other published studies, with an average age of 47.75 ± 4.38 and an age range of 41 to 55. This difference could have affected the postoperative results obtained, since near and intermediate VA is normally higher in younger patients. JOURNAL OF EMMETROPIA - VOL 7, JANUARY-MARCH 44 DEFOCUS CURVES AFTER PRESBYOPIA SURGERY Regarding the refractive outcomes obtained with the surgical procedure, in Reinstein et al.25, 100% of patients achieved 20/20 or better binocular UDVA and 96% achieved binocular UNVA of J2. In Luger’s22 study, 93% of patients achieved 20/20 or better binocular UDVA and 90% achieved J2 or better UNVA; 7% of patients lost 2 lines of CDVA. In Falcon et al.24, 91.1% of patients achieved a binocular distance vision of 20/20 or better, and 86.7% achieved a near vision of J1. In our study, 100% of patients achieved a UDVA of 20/20, while 33.3% of group I and 20% of group II achieved a UNVA of J4 or better. Therefore, the near vision outcomes in our study are lower than those reported by other authors. Some differences between the 2 study groups were observed in terms of defocus curves. Vergences range from 0 to +3 is not specified because there is no change in either pre- and postoperative focusing results in vergences −5 to 0. Both groups had a preoperative UDVA of 0 logMAR, which was maintained postoperatively. Some differences were observed between groups for all the other distances, although these are not statistically significant for any of the distances measured (p > 0.05). Before surgery, Group II achieved a higher VA in distances ranging from 1 m to 40 cm and from 25 to 20 cm. Preoperative UDVA at 67 cm was 0.10 in group I and 0.06 in group II. Similarly, VA at 33 cm was 0.47 in group I and 0.3 in group II. These results affected the near and intermediate visual outcomes after surgery, as group II did not achieve the same improvement percentages as group I, because the latter had higher initial visual acuities. Luger et al.22, in their evaluation of defocus curves, reported that patients with a mean initial SE of −1.08 ± 2.62 D and 0.52 ± 0.42 D astigmatism achieved a mean gain of 2 lines of near vision at 33 cm (−3 D), no changes at 67 cm, and lost half a Snellen line of distance vision. Our defocus curves show that patients in group I gained VA in the 40-20 cm range after surgery, with no changes in distance vision. Patients in group II did not experience any changes in distance vision either, but lost VA in the 29-20 cm range. Surgical outcomes were more satisfactory in group I, though only with regard to intermediate and near VA. This discrepancy may be explained by the fact that myopic patients usually maintain excellent VA at these distances. With regard to against-the-rule astigmatism, the curvature of greater power is near the horizontal meridian, between the meridians of 30° to 150°, so that the corrector cylinder is between 60° to 120°. This astigmatism generates an increased depth of focus, improving near vision26. Due to this factor, 12 eyes of group I and 10 eyes of group II received additional help in near vision. All patients in both groups achieved complete independence from distance spectacles after surgery. Independence from near spectacles was achieved by 91.4% of patients in group I and 61.7% in group II, showing that a correct near VA can be maintained for most tasks, while glasses are only needed to carry out certain tasks. In conclusion, the results obtained in our study demonstrate that corneal ablation decreases presbyopia symptoms and corrects distance refraction in a single surgical procedure, thus offering patients greater independence from glasses in their daily lives. Studies with larger sample sizes and a longer postoperative monitoring period are needed to assess refractive stability over time. Defocus curves are useful tools to evaluate visual performance after refractive surgery. REFERENCES 1. Census data and global changes in demographics. Available at: http://www.census.gov/cgi-bin/broker. Accessed March 15, 2012. 2. Patel I, West S. Presbyopia: prevalence, impact and interventions. Community Eye Health J. 2007; 20:40-1. 3. Jain S, Arora I, Azar DT. Success of monovision in presbyopes: review of the literature and potential applications to refractive surgery. Surv Ophthalmol. 1996; 40:491-9. 4. Alió JL, Chaubard JJ, Caliz A, Sala E, Patel S. Correction of presbyopia by Technovision central multifocal LASIK (presbyLASIK). J Refract Surg. 2006; 22:453-60. 5. Jackson WB, Tuan KM, Mintsioulis G. Aspheric wavefront-guided LASIK to treat hyperopic presbyopia: 12-month results with the VISX platform. J Refract Surg. 2011; 27:519-29. 6. Moreira H, Garbus JJ, Fasano A, Lee M, Clapham TN, McDonnell PJ. Multifocal corneal topographic changes with Excimer laser photorefractive keratectomy. Arch Ophthalmol. 1992; 110:994-9. 7. Cosar CB, Sener AB. Supracor hyperopia and presbyopia correction: 6-month results. Eur J Ophthalmol. 2014; 24:325-9. 8. Tomita M, Kanamori T, Waring GO, 4th, Nakamura T, Yukawa S. Small-aperture corneal inlay implantation to treat presbyopia after laser in situ keratomileusis. J Cataract Refract Surg. 2013; 39:898-905. 9. Limnopoulou AN, Bouzoukis DI, Kymionis GD et al. Visual outcomes and safety of a refractive corneal inlay for presbyopia using femtosecond laser. J Refract Surg. 2013; 29:12-8. 10. Gupta N, Wolffsohn JS, Naroo SA. Optimizing measurement of subjective amplitude of accommodation with defocus curves. J Cataract Refract Surg. 2008; 34:1329-38. 11. Holladay JT, Van Dijk H, Lang A, et al. Optical Perfomance of multifocal intraocular lenses. J Cataract Refract Surg. 1990; 16:413-22. 12. Mastropasqua R, Pedrotti E, Passilongo M, Parisi G, Marchesoni I, Marchini G. Long-term visual function and patient satisfaction after bilateral implantation and combination of two similar multifocal IOLs. J Cataract Refract Surg. 2015; 31:308-14. JOURNAL OF EMMETROPIA - VOL 7, JANUARY-MARCH 45 DEFOCUS CURVES AFTER PRESBYOPIA SURGERY 13. Plaza-Puche AB, Alió JL, MacRae S, Zheleznyak L, Sala E, Yoon G. Correlating optical bench performance with clinical defocus curves in varifocal and trifocal intraocular lenses. J Refract Surg. 2015; 31:300-7. 14. Malacara D. Optical Shop Testing, 2nd Ed. New York, NY: John Wiley & Sons, Inc; 1992. 15. Gupta N, Naroo SA, Wolffsohn JS. Is randomisation necessary for measuring defocus curves in pre-presbyopes? Cont Anterior Eye. 2007; 30:119-24. 16. Wolffsohn JS, Jinabhai AN, Kingsnorth A, et al. Exploring the optimum step size for defocus curves. J Cataract Refract Surg. 2013; 39:873-80. 17. Alió JL, Vega-Estrada A, Plaza-Puche AB. Clinical outcomes with a new microincisional diffractive multifocal IOL. Eye Vis (Lond). 2015; 2:2. 18. Baudu P, Penin F, Arba Mosquera S. Uncorrected binocular performance after biaspheric ablation profile for presbyopic corneal treatment using AMARIS with the PresbyMAX module. Am J Ophthalmol. 2013; 155:636-47. 22. Luger MH, McAlinden C, Buckhurst PJ, Wolffsohn JS, Verma S, Arba Mosquera S. Presbyopic LASIK using hybrid bi-aspheric micro-monovision ablation profile for presbyopic corneal treatments. Am J Ophthalmol. 2015; 160:493-505. 23. Reinstein DZ, Couch DG, Archer TJ. LASIK for hyperopic astigmatism and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 platform. J Refract Surg. 2009; 25:37-58. 24. Falcon C, Norero Martínez M, Sancho Miralles Y. Laser Blended Vision for presbyopia: Results after 3 years. J Fr Ophtalmol. 2015; 38:431-9. 25. Reinstein DZ, Archer TJ, Gobbe M. LASIK for Myopic Astigmatism and Presbyopia Using Non-Linear Aspheric MicroMonovision with the Carl Zeiss Meditec MEL 80 Platform. J Refract Surg. 2011; 27:23-37. 26. Kordić R, Kalauz M, Kuzman T, et al. Effect of the against the rule myopic astigmatism on the near vision of the elderly. Coll Antropol. 2014; 38(4):1223-4. 19. Artal P, Guirao A, Berrio E, Williams DR. Compensation of corneal aberrations by the internal optics in the human eye. J. Vision. 2001; 1:1-8. 20. Jackson WB, Tuan KM, Mintsioulis G. Aspheric wavefront-guided LASIK to treat hyperopic presbyopia: 12-month results with the VISX platform. J Refract Surg. 2011; 27:519-29. 21. Reinstein DZ, Carp GI, Archer TJ, Gobbe M. LASIK for presbyopia correction in emmetropic patients using aspheric ablation profiles and a micro-monovision protocol with the Carl Zeiss Meditec MEL 80 and VisuMax. J Refract Surg. 2012; 28:531-41. JOURNAL OF EMMETROPIA - VOL 7, JANUARY-MARCH First author: Marta Romero-Domínguez, MD Hospital Universitario Quirónsalud, Madrid, Spain.