Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
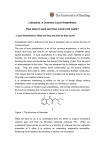
1 Local anaesthetics: Local anaesthetics: refers to chemical that are applied or administered locally to cause reversible blockade of axonal conduction with consequent loss of sensations from the concerned area without affecting consciousness. Or refers to the state of local analgesia produced by local anaesthetics.it is of different types depending upon the mode of use of local anaesthetics. Topical or (surface anaesthesia ) : refers to the state of local anaesthesia accomplished by applying local anaesthetic directly to mucus membranes or exposed nerve endings so as to block primarily peripheral exposed nerve terminals . the agents used for this purpose are called topical anaesthetics. Also include dental analgesics (inserted into carious teeth) or the agents used on the skin to relieve pruritis. Cutaneous inflammatory conditions or for minor surgical procedures where relief from pain is required. Infiltration anaesthesia : Refers to anaesthetizing an area or tissue by making one or more injections (usually subcutaneous and occasionally into organs or joints spaces) of a local anaesthetics without taking into consideration the course of the nerve supply. Spinal anaesthesia : refers to depositing local anaesthetics into the CSF (i.e. subarachnoid space) so as to block many nerve roots quickly as they emerge from spinal cord. It is also known as : Regional anaesthesia : is a general term referring to local anaesthesia that pertains to a larger area or region of the body.it includes paravertebral , epidural , spinal , nerve plexus blocking or retrograde intravenous regional anaesthesia. Retrograde regional anaesthesia : erfers to anaesthetization of extremities by injecting local anaesthetic into superficial veins(radial or metatarsal) after tying a tourniquet to confine the drug into the region for action ; the drug diffusing from blood to peripheral nerve sites. 2 Refrigeration anaesthesia : refers to anaesthetization of surface , mainly skin , by spraying a high volatile agent (as alkyl halides) that causes sueface cooling and freezing following evaporating of agent with consequent tissue heat loss. Such agents are called refrigerant anaesthetics. Spraying of liquefied carbon dioxide to the skin surface also produces same action. Differences between local & general anesthesia : Parameter Local anesthetic General anaesthetic Site of action Peripheral nervous system Central nervous system ( (peripheral nerve) brain) Mode of action Block axonal conduction Alter synaptic transmission) Consciousness unaffected lost Analgesia Localized analgesia generalized administration Local deposition away from Systemic systemic circulation Systemic availability : inhalant or parenteral Undesirable responsible for Requisite for action toxicity Toxic potential and Low toxicity (CNS stimulation High , CNS depression. (convulsion , seizures) An ideal local anaesthetic An ideal local anaesthetic should qualify four principal qualities : it should be selective and effective for action and safe and stable for use : Selective : it should selectively block the function of sensory nerves (reversible paralysis) to produce local analgesic. 3 Effective : it should be effective whether applied topically or upon injection. Onset of action should be rapid . duration of action should be adequate , neither too short nor too prolonged to extend recovery period.high potency is desirable so that smaller amounts can be used. Safe : it implies requirements as i) it should not damage the tissue at therapeutic concentrations as irritancy be negligible ii) it should be slowly absorbed from the site of application into the systemic circulation so that its action is prolonged and systemic toxicity is minimized iii) once absorbed into circulation it should be rapidly detoxified iv) it should produce low systemic toxicity v) anaesthesia should not be preceded by sensory nerve stimulation (unlike aconite or phenol) nor followed by hyperaesthesia. There is none that qualifies all the criteria . however , commonly employed local anaesthetics. As lidocaine and procaine fulfill most of the criteria at recommended concentrations. Other agents differ from these mainly with respect to relative potency, duration of action and toxicity. General indications of local anaesthetics : Emergencies : Minor operation : Obstetrical practice : Field conditions : Patient conditions : Major operation : Classification of local anaesthetics : 1- On the basis of chemical features : 4 a)- amino-group containing agents :( common category) i)-Esters : contain esteric linkage : most are benzoic acid esters as cocaine , procaine , chloroprocaine , tetracaine , benzocaine, hexylcaine , butamben , proxymetacaine , benozinate ii)-Amides : contain amide linkage : longer acting than esters Lidocaine , prilocaine , bupivacaine , mepivacaine , rupivacaine , etidocaine , dibucaine iii)- Ketone : contain keto group in the intermediate chain / dyclonine B)-Non-amino agents (non-classical local anaesthetic agents) i) alcohols : ethanol , phenol , isopropyl alcohol , eugenol , creosote , chlorobutol , benzyl alcohol , menthol. ii)-alkyl halides : ethyl chloride and methyl chloride. 2- on the basis of duration of action . i)-ultra-short duration of action : duration of action brief,less than or equal to 15 minute: benoxinate , proparacaine ii)-short acting : duration of action upon an hour : procaine , chloroprocaine , cocaine iii)-intermediate acting : duration of action upon 1to4 hours. As lidocaine (lignocaine or xylocaine ) mepivacaine , prilocaine iv)-long acting : duration of action about 4-10 hours or may be longer // bupivacaine , ropivacaine , tetracaine , etidocaine , hexylcaine & cinchocaine. Factors affecting local anesthetic action: 5 1-type of nerve fiber : small (thinner) nerve fibers as thinner sensory and postganglionic sympathetic fibers (C-type) and preganglionic sympathetic fibers (B-type) are most sensitive to conduction blockade by local anaesthetics. Large (thicker) sensory fibers (A-delta type) are moderate sensitive . A-beta & A-gamma fibers (more thiker) subserving muscle tone and proprioception , are less sensitive while somatic motor fibers (A-alpha , thikest) are least sensitive to local anaesthetic action .myelination does not appear to affect nerve sensitivity to the blockade. Nerve membrane is more permeable to local anaesthetic molecules during depolarization state than during resting state . this renders sensory fibers in general and the pain fibersin particular more susceptible to blockade as they tend to generate long-duration action potential and at higher frequency while motor fibers generates short duration action potential and at lower frequency. 2-Ph & PKa : commonly used local anaesthetics are weak organic bases with pka in the range 8-9 . tissue ph (about 7.4) favours their ionization (protonation) such that more than 60% of the drug molecules exist in protonation form.unprotonated form is responsible for diffusion through lipid matrix. Protonated form is presumed to enter the membrane through ion channel (during depolarization state) and to bind specifically to binding sites. Tissue ph is definitely an important factor that would affect diffusion of the base across the membrane ; thus local anaesthetics with varying pka values are expected to diffuse the membranes at varying rate. Inability of local anaesthetics to block conduction from purulent site is related to the abnormal environment at purulent sites.such sites are relatively acidic and contain higher potassium levels as well as rich in anions (e.g proteins , organic phosphates and nucleotides) due to high cell destruction . acidic ph decreases hydrolysis of acid salt (i.e hydrochloride) thus reducing release of active organic base. Acidic ph would favour ionization and hence reduce diffusion of the active base.hydrogen ions are known to block sodium ion channels directly by occupying its anionic sites. 3-potentiators : Vasoconstrictor : adrenaline or any other vasoconstrictor reduces rate of absorption of local anaesthetic from the site od deposition . reduced rate of systemic availability tends to reduce 6 systemic toxicity. Duration of action is accordingly prolonged in presence of a vasoconstrictor . the effect is pronounced with local anaesthetics having pronounced vasodilator action as procaine and lidocaine . prilocaine has little vasoconstrictor action so can be used without adrenaline . cocaine is vasoconstrictor so adrenaline is not required. On the other hand use of adrenaline is contraindicated with cocaine as later tends to potentiate its sympathomimetic effects by preventing uptake of catecholamines at nerve terminals. Hyaluronidase : the enzyme hydrolyses ground substance (i.e hyaluronic acid) so increases area of diffusion and hence area of effect of local anaesthetics. increased diffusion tends to reduce duration of effect and increase chances of toxicity as the drug would reach systemic circulation faster. The benefits are discernible only when vasoconstrictor is also used along with the hyaluronidase ; duration and area of effect are nearly doubled . use of hyaluronidase in veterinary practice is not recommended i)-it is costly ii(-tends to interfere with local anaesthetic action especially when used alone. Iii)-chances of systemic toxicity by local anaesthetics are increased iv)-its use has limited applications i.e infiltration or subcutaneous anaesthesia. Toxicity and complication of local anaesthetics Local effects : local damage consists of transient or permanent injury to tissues due to the irritancy . recommended concentrations are practically non-irritant. Tetracaine is more irritant , 8-10 fold more than procaine. Nerve damage can be result if high concentrations are deposited into nerves or very close to the nerve. Proparacaine causes a transient corneal roughening for 30-60 minutes. Systemic effects : is determined by balance of rate of absorption to the rate of destruction of local anaesthetics.the toxicity is primarily due to CNS stimulation presumably due to inhibition of GABA ergic synaptic function leading to restlessness , muscle tremors , convulsive seizures Death occurs rarely due to respiratory failure. Neurostimulation is followed by depression of all CNS functions. 7 Cardiovascular , respiratory and skeletal muscle functions may be affected following epidural and or spinal anaesthesia as a complication of the particular route. Allergic reactions : allergic dermatitis or topical asthmatic attack has been observed in humans with exclusively ester type local anaesthetics , some ester metabolite acting as a hapten.the occurance is , however is rare. Factors affecting systemic toxicity of local anaesthetics : 1-type of drug : toxicity potential of a drug appears to be related to anaesthetic potential,thus highly potent drugs are also highly toxic . Cocaine induced CNS stimulation is primarily related to potentiation of central biogenic amines as cocaine prevents reuptake of released biogenic amines at presynaptic sites. Hyaluronidase can potentiate toxicity by increasing area of absorption and hence rate of diffusion of local anaesthetic into systemic circulation . adrenaline reduced toxicity by reducing absorption rate. It may lead to cardiac arrhythmias if used in higher concentrations and is particularly dangerous to use with cocaine. 2-species : susceptibility to convulsions is related to degree of CNS development , primates are more sensitive than domestic animals.horses are more sensitive than swine.ruminants particularly cattle appear to be least sensitive . among birds, parakeets are extremely sensitive to lethal effects of procaine. 3-route : the toxicity is obviously greater if drug goes inadvertently into vein while it is intended for local deposition or if tourniquet is loosely applied while attempting retrograde intravenous regional anaesthesia.MLD of procaine , cocaine and cinchocaine on subcutaneous use are respectively about 1/10 , 1/8 , ¼ of intravenous amounts. 4-ambient temperature : avoid infiltration of local anaesthetics into the tissues under high ambient temperature , excessive absorption follows due to cutaneous vasodilation this is particularly true with thin skinned and very young animals as puppies. Classical local anaesthetic : 8 Organic bases are poorly water soluble except cocaine and tetracaine which show little water solubility. Hydrochlorides are quite soluble in water. Aqueous solution of hydrochlorides are acidic except tetracaine and benoxinate salts that are neutral.aqueous solution of dyclonine Hcl is acidic to neutral. The esters are a class less stable than amides . the aqueous solutions are sterilized by autoclaving or by filtration cocaine & tetracaine are less stable to heat so their solutions are sterilized by controlled heat in the presence of bactericide. It is recommended to keep aqueous solution of local anaesthetics in air-tight containers and away from light. Cocaine : local anaesthetic potency is 3 times that of procaine. Onset of action is about 5 minutes and duration of action 20-45 minutes (topical) and up to 2hours (spinal). It is vasoconstrictor and mydriatic agent. The drug was once choice anaesthetic for all uses. Its now exclusively recommended for topical anaesthesia ; 2-4% solution for ophthalmic anaesthesia, and 5-10% for other mucosal uses. Vasoconstrictor potential restricts its prolonged ophthalmic use as it favour ischemia and coroneal ulceration. It is advantageous on other mucosal uses as it reduces operative bleeding . high tissue irritancy disfavours its use as infiltration agent. Systemic toxicity potential is at least 4 times of procaine . it is a scheduled drug so not freely available for use , there is high abuse (addiction) potential to its psychomitic action (i.e euphoria).