Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Artificial gene synthesis wikipedia , lookup
Molecular cloning wikipedia , lookup
Comparative genomic hybridization wikipedia , lookup
Surround optical-fiber immunoassay wikipedia , lookup
Western blot wikipedia , lookup
Restriction enzyme wikipedia , lookup
Community fingerprinting wikipedia , lookup
Deoxyribozyme wikipedia , lookup
Cre-Lox recombination wikipedia , lookup
ADVANCED DIAGNOSTIC
TECHNIQUES IN
PERIODONTICS
INTRODUCTION
In light of advances in clinical and basic
science research,our understanding of the initiation
and progression of periodontal diseases and the
pathogenic process involved has expanded
enormously.
CONVENTIONAL PERIODONTAL
DIAGNOSIS - LIMITATIONS
Conventional diagnosis of periodontal diseases include
clinical evaluation of inflammation in gingivitis, clinical
attachment loss with radiographic assessment of bone
loss in periodontitis.
This
information provides only the evidence of past
periodontal destruction and its extent & severity.
This doesn't provide the information on
cause of the condition,
patients susceptibility to the disease,
disease progression or remission &
response to the therapy.
Hence many advances are made to include;
immunologic
Microbiologic
systemic
genetic
behavioral factors
in addition to the traditional clinical & radiographic parameters.
ADVANCES IN CLINICAL DIAGNOSIS
1.Gingival bleeding:
It is the sensitive indicator of early gingival
inflammation.
The severity of bleeding increases with an
increase in size of the inflammatory infiltrate.
It can be evaluated using periodontal probe or
a wooden interdental cleaner.
A force greater than 0.25N may evoke bleeding
in healthy sites with an intact periodontium.
The sites that bled on probing at several visits
has the higher probability of loosing attachment
than those that bled at one visit or did not bleed.
2.Gingival temperature:
• Active periodontitis can create
measurable rise in sulcular
temperature.
• Thermal probes like Periotemp
probe detects the temp differences
of 0.1*c from a referenced sub
gingival temperature.
• Higher temperature are signaled
with red indicator and has more
than twice the risk for future
attachment loss than did those of
green indicator.
3.Periodontal probe:
• The main disadvantage of traditional
periodontal probing is its lack of sensitivity
and reproducibility which is due to difference
in
Probing technique,
Force of probe,
Size of probe,
Angle of insertion of the probe and
Precision of the probe calibration.
• This contributes to deviation of about 0.51.3mm making detection of small changes
difficult.
Classification of periodontal probes:
Generation 1: conventional hand held
probe. WHO
Generation 2: pressure sensitive probe.
Vivadent
Generation 3: computerized probe. Florida,
Foster Miller
Generation 4: probes aimed at recording
sequential probing along the sulcus.
Generation 5: ultrasonic device attached to
the fourth generation probe.
NIDCR-National institute of cranio facial
research
Defined nine criteria for overcoming these limitations.
They are:
1.
2.
3.
4.
5.
6.
7.
8.
Precision
Range
Probing force
Applicability
Reach
Angulations
Security
Readout
- 0.1mm
-10mm
- constant and standardized
- non-invasive, light weight &easy to use
- easy to access
- a guidance system for proper
- complete sterilization and no biohazard
- direct electronic reading and digital
output.
Following these criteria
• Florida probe system was developedconsists of probe hand piece with coil
springs, digital readout, footswitch and
computer.
* Advantage - constant probing force
with precise electronic measurement and
computer storage of data
* Disadvantages – lack of tactile
sensitivity and predetermined insertion point
and angle producing inaccurate
measurement and patient discomfort.
PRESSURE
SENSITIVE
PROBE
FLORIDA PROBE
• Foster-Miller probe has coupling effect by
determining the pocket depth and CE junction
from which clinical attachment level is
automatically detected.
• Toronto automated probe: has 0.5mm
nickel-titanium wire that is extended under air
pressure with the mercury tilt sensor that
limits the angulations to +_30*
• The development of these probes will allow
more sensitive assessments of disease
progression.
ADVANCES IN RADIOGRAPHIC
ASSESSMENT
• The substantial amount of bone loss(>30%)at
alveolar crest must be there for a change in
bone height should be recognized on a
conventional radiograph.
LIMITATIONS:
•
projection geometry,
•
film processing, voltage and exposure time,
•
masking of osseous changes by other
anatomic structures.
1.DIGITAL RADIOGRAPHY:
• It enables the use of computerized images that can
be stored manipulated and corrected for under and
over exposures.
• There is important dose reduction obtained with
technique( 1/3 to 1/2).
• Based on the sensor, digital radiography can be
divided as the direct and indirect methods.
• Direct method-uses a charged coupled
device(CCD)sensor linked with a fiber optic to the
computer.The disadvantage being limited sensor
rigidity making sterility and image projection using
film holders is very difficult.
CONTD:…
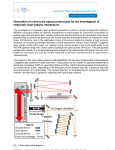
• Indirect
method(Digora
system)-uses
phosphor
luminescence plate
which is a flexible
film like sensor
placed intra-orally
and exposed to
conventional x-ray
tube. large scanner
reads the exposed
plate and reveals the
digital image.
3.COMPUTER-ASSISTED DENSITOMETRIC IMAGE
ANALYSIS SYSTEM (CADIA)
• In this system video camera measures the light
transmitted through a radiograph and the
signals are converted into gray-scale images in
a computer.
• It has shown a higher sensitivity, high degree
of reproducibility and accuracy.
ADVANCES IN MICROBIOLOGIC ANALYSIS:
Micobiologic analysis have the potential
• To support the diagnosis,
• To serve as indicator of disease activity
• To determine the site at higher risk and
• To monitor periodontal therapy.
BACTERIAL CULTURING:
They are still considered reference method (gold
standard).
Advantage: the relative and absolute count and antibiotic
susceptibility of the microbes are obtained.
Disadvantage: 1. media can grow only live bacteria
needing strict sampling and transport,
2..sensitivity is rather low and
3..it requires sophisticated
equipments,experienced personnel, is relatively time
consuming and expensive.
DIRECT MICROSCOPY:
The morphology and motility of bacteria can be directly
assessed, however the main putative organism are nonmotile.
IMMUNODIAGNOSTIC METHODS:
This employs antibodies that recognize specific
bacteria to detect the target microorganism
1)Direct immunofluroscent microscopic assay :
•
This employs florescent marked antibody to
form a complex with bacteria,which is
detectable under microscope.
•
Studies shows 82% to 100% sensitivity for
A.actinomycetemcomitans.
2) ELISA: {Enzyme linked immunosorbant
assay}:
•
Here enzyme derived colour reaction is used
as label. The intensity of the colour depends
on the concentration of the antigen and is read
photo metrically.
• Used primarily to detect serum antibodies for
periodontopathogens.
ENZYMATIC METHODS OF BACTERIAL
IDENTIFICATION:
P.Gingivalis, Treponema denticola, B.forsythus have in
common a trypsin like enzyme. The activity of this
enzyme can be measured with the hydrolysis of
BANA(N-benzoyl-l-arginine-2-naphthylamide) –
releases chromophore –turns orange red with fast
garnet. Perioscan- diagnostic kit.
It is 80%-90% positive in 7mm deep pocket.
Disadvantage:
• It may be positive in healthy sites.
• It detects limited no. of pathogens.
PERIO SCAN:
DEOXYRIBONUCLEIC ACID PROBE
TECHNOLOGY:
1) NUCLEIC ACID PROBES:
The probe is prepared by labeling the single strand
DNA of specific organism with the radioisotope.
The plaque sample is prepared by lyses and
denaturation and single strand is attached to specific filter
paper and exposed to DNA library.
If complementary base pair hybridized isotope will be
fixed to the filter paper and is read with a densitometer.
The darkness and size indicate conc. of
microorganism.
It can rapidly test A.a, P.g, Fusobacterium nucleatum.
DNA PROBE
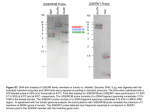
2)RESTRICTION ENDONUCLEASE ANALYSIS:
Restriction endonucleases recognize
and cleaves the double stranded DNA to
single stranded DNA,which is then separated
by electrophoresis and stained & visualized
with UV light.
These fragment pattern constitute a
specific finger print to each strain. Thus it is a
powerful tool for determining specific
pathogen.
3.POLYMERASE CHAIN REACTION:
• It involves the amplification of a region
of DNA by a selected primer of specific
specious. the specific amplification
product indicates its presence.
• It has best detection limits, as few as 510 cells.
• It has no cross reactivity.
• Drawback- it uses small quantity of
plaque sample hence negative results
should be reconsidered.
ADVANCES IN CHARACTERISING THE
HOST RERSPONSE:
This refers to the study of mediators like
– antibodies which are specific to infection &
- the less specific
inflammatory mediators,
host derived enzymes &
tissue breakdown products.
Sources of Sample:
• saliva,
• Gingival crevicular fluid,
• blood serum &
• urine.
GCF SAMPLING:
PERIO PAPER
1.Inflammatory mediators and
products
Research on GCF has focussed on search
of potent mediators like
• Cytokines- TNF, interleukins which
produce metalloproteinase stimulation
and bone resorption.
• Prostoglandin E2-which induces bone
resorption. Therefore they marks the
disease progression.
2.Host-derived enzymes:
•
Aspartate amino transferase -released from
dead cell. It is increased in GCF from sites with
severe gingival inflammation and a progressive
attachment loss. Chair side kit(Periogard)is
available to detect this.
•
Alkaline phosphatase -found in
osteoblast,fibroblast and neutrophils.It is significantly
higher in diseased sites,showing the progression of
periodontitis.
•Beta glucorinidase, elastase are the enzymes found in
neutrophils are elevated in periodontitis.
•Elastase- is a protease stored in azurophilic granules of
neutrophils.Periocheck is a chairside kit to detect
neutral proteases in GCF.
•
Matrix metalloproteinases released from fibroblast
and macrophages, increased in destructive periodontitis.
3.Tissue break down products:
Periodontitis is the destruction of
collagen and extracellular matrix, producing
hydroxyproline and glycosaminoglycans
respectively. Alveolar bone loss can be
correlated with osteocalcin.
• GCF from these sites shows elevated level
of these products.
• However no rapid chair side kit has been
developed for clinical use.
•
CONCLUSION
After all these years of intensive
research, we still lack a proven diagnostic tests
that has demonstrated high predictive value for
disease progression, has a proven impact on
disease incidence & prevalence and is simple &
cost effective.
THANK YOU