Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
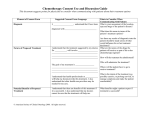
Chapter 3 Legal and Ethical Issues and Documentation Copyright (c) The McGraw-Hill Companies, Inc. Permission required for reproduction or display. 3-1 Objectives 3-2 The Legal System 3-3 Branches of Government • Legislative • Executive • Judicial 3-4 Government Legislative Branch • Made up of Congress and government agencies • Law made by this branch of government is called statutory or legislative law. 3-5 Government Executive Branch • President of the United States is the head of the executive branch • This branch includes: – Vice President – Cabinet members – State governors – State and federal administrative agencies 3-6 Government Executive Branch • Administrative agency – A governmental body responsible for implementing and enforcing a particular law passed by the legislature – Rules and regulations made by the executive branch are called administrative law. 3-7 Government Judicial Branch • Court system • Courts hear cases that challenge or require explanation of the law • Federal courts • State courts 3-8 Government Judicial Branch • Court levels – Trial courts – Appellate courts – Supreme courts 3-9 Lawsuit • Plaintiff • Defendant • Statute of limitations 3-10 Criminal Law • Area of law in which the federal, state, or local government prosecutes individuals on behalf of society for violating laws designed to safeguard society • Punishable by fine, imprisonment, or both 3-11 Civil Law • A branch of law that deals with complaints by individuals or organizations against a defendant for an illegal act or wrongdoing (tort) 3-12 Steps in a Lawsuit • Incident occurs • Investigation is conducted by plaintiff's representative • Complaint is filed in court and served on defendant • Complaint is answered by defendant 3-13 Steps in a Lawsuit • Discovery occurs • Depositions (oral) or interrogatives (written) are taken • Documents are gathered – Patient records – Prehospital care reports 3-14 Steps in a Lawsuit • Pre-trial conference – Narrows the issues to be decided during the trial – Attempt to persuade the attorneys to settle their case – Most cases are settled during this period 3-15 Steps in a Lawsuit • Trial is conducted • Decision is handed down by judge or jury – Decision may be appealed 3-16 Scope of Practice • The emergency care and skills an EMT is legally allowed and expected to perform when necessary • Also called the scope of care 3-17 Scope of Practice • May be modified by using standing orders and protocols 3-18 Standard of Care • You are expected to provide the same standard of care in an emergency as another EMT with similar training and experience in similar circumstances 3-19 Emergency Medical Technician Skills • Patient assessment • Insertion of oral and nasal airways • Assisting patients in taking their own prescribed mediations • Upper airway suctioning • Giving specific over-thecounter medications • Bag-mask (BM) ventilation • External hemorrhage control • Supplemental oxygen therapy • Bandaging wounds • Cardiopulmonary resuscitation (CPR) • Splinting • Automated external defibrillation (AED) • Pulse oximetry • Using a tourniquet • Assisting in childbirth • Assisting in lifting and moving patients • Mechanical patient restraint 3-20 Medical Oversight • Your legal right to function as an EMT depends on medical oversight – Physician must oversee your training and practice 3-21 EMT: Legal Duties • Provide for the well-being of the patient by giving emergency medical care as outlined in the scope of practice • Provide the same standard of care as another EMT with similar training and experience in similar circumstances • Before providing emergency care, make telephone or radio contact with your medical oversight authority (if required to do so) • Follow standing orders and protocols approved by medical oversight or the local EMS system • Follow instructions received from medical oversight 3-22 Ethics • Principles of right and wrong, good and bad, and the consequences of human actions – In other words, what a person ought to do 3-23 Ethical Responsibilities • Treat all patients with respect • Give each patient the best care you are capable of providing – Practice and master your skills – Take advantage of continuing education (CE) and refresher programs – Look for areas in which you can improve 3-24 Ethical Responsibilities • Be honest and accurate in your written and verbal communication • Respect your patient’s right to privacy – Protected health information (PHI) 3-25 Ethical Responsibilities • Have respect for and work cooperatively with other emergency care professionals 3-26 Competence • The patient’s ability to understand the questions you ask him and understand the result of the decisions he makes about his care 3-27 Competence • Legal competence • Mental competence • Medical/situational competence 3-28 Incompetence • An adult is generally considered incompetent if she: – Has an altered mental status – Is under the influence of drugs or alcohol, including legal or prescription drugs – Has a serious illness or injury that affects her ability to make an informed decision about her care – Has been declared legally incompetent related to a known mental disorder 3-29 Consent • Consent = permission • You must have consent before assessing or treating a patient • Any competent patient has the right to make up his own mind concerning his care 3-30 Expressed Consent • Patient gives specific authorization for care and transport – Must be obtained from every responsive, mentally competent adult before providing care – Patient must be of legal age and competent to give consent 3-31 Expressed Consent • To obtain expressed consent: – Identify yourself and your level of medical training – Explain all treatments and procedures to the patient – Identify the benefits of each treatment or procedure – Identify the risks of each treatment or procedure 3-32 Expressed Consent • Use words and phrases the patient can understand – Do not use confusing medical terms 3-33 Expressed Consent • A competent adult can withdraw consent at any time during care and transport 3-34 Implied Consent • Consent is assumed from a patient requiring emergency care who is mentally, physically, or emotionally unable to provide expressed consent – Effective only until the patient no longer requires emergency care or regains competence to make decisions 3-35 Implied Consent (1 of 2) • Applies to patients who are – Unconscious – Otherwise incapable of making informed decision Source: © Dan Myers Implied Consent (2 of 2) • Should never be used unless there is a threat to life or limb. • Principle of implied consent is known as the emergency doctrine. • Good to get consent from a spouse or relative. Consent: Implied Consent implied for unconscious patient Based on the assumption the patient would consent if conscious Special Situations • Children and mentally incompetent adults must have a parent or guardian give consent for treatment • If a life-threatening emergency exists, treat under implied consent 3-39 Medical Identification Devices Alert EMT to patient’s medical condition, such as: – Heart condition – Diabetes – Allergies – Epilepsy – Other information Medical Identifications Devices (Front) Medical Identification Devices (Back) Involuntary Consent • Applies to patients who are: – Mentally ill – In behavioral crisis – Developmentally delayed • Obtain consent from guardian – Not always possible, so understand local provisions Involuntary Transportation • Patient considered threat to self or others • Court order • Usually requires decision by mental health professional or police officer • If patient restrained, must not risk legal liability Refusals • If a patient refuses treatment or transport, you must inform her of the following: – Nature of her illness or injury – Treatment that needs to be performed – Benefits of that treatment – Risks of not providing that treatment – Any alternatives to treatment – Dangers of refusing treatment (including transport) 3-45 Refusals • Do not make a decision on your own not to treat or transport a patient. • Consult with medical direction or leave this decision to advanced medical personnel on the scene. 3-46 Examples of High-Risk Refusals • • • • • • • • • • Abdominal pain Chest pain Severe electrical shock Foreign body ingestion Poisoning Pregnancy-related complaints Water-related incidents Falls >20 feet Vehicle rollovers Head injury • High-speed auto crashes • Auto-pedestrian or auto-bicycle injury with significant (>5 mph) impact • Pedestrian thrown or run over • Motorcycle crash >20 mph or with separation of the rider from bike • Pediatric patient with a vague medical complaint 3-47 Refusal Documentation • • • • • • • • • • Patient’s name, age, and chief complaint Patient’s medical history Two complete sets of vital signs Patient’s mental status (including orientation) Patient’s behavior and cooperation Patient’s ability to follow instructions/commands Physical examination findings Patient’s reason for refusing treatment and/or transport Patient agrees to call 911 if the condition recurs, becomes worse, or if he/she changes their mind Patient’s signature 3-48 The Right to Refuse Treatment (1 of 2) • Conscious, alert adults with decisionmaking capacity: – Have the right to refuse treatment – Can withdraw from treatment at any time – Even if the result is death or serious injury • Places burden on EMT to clarify need for treatment The Right to Refuse Treatment (2 of 2) • Before you leave a scene where a patient, parent, or caregiver has refused care: – Encourage them again to allow care. – Ask them to sign a refusal of care form. – Document all refusals. – A witness is valuable in these situations. Refusal of Care • Patient may refuse care or transport – Legally able to consent – Mentally competent and oriented – Fully informed of risks – Sign release form • Despite all precautions, EMT may still be held liable If in Doubt About Refusal • • • • • • Discuss decision with patient Ensure patient understands risks Consult medical direction Ask to contact family member Contact law enforcement Listen to patient to determine why refusing care Pertinent Legal Documents 3-53 Durable Power of Attorney • Document that allows a patient to appoint a person or organization to handle affairs while they are unavailable or if they are unable to make decisions for themselves. • The person or organization appointed is referred to as an "Attorney-in-Fact" or "Agent." 3-54 Durable Power of Attorney Two main types 1.Power of Attorney for Health Care Purposes – Allows the Agent to make health care decisions on the patient’s behalf if they are unconscious, mentally incompetent, or otherwise unable to make such decisions. – Is void if the patient is mentally able to make their own decisions. 3-55 2. Power of Attorney for General Purposes – Authorizes the Agent to act on the patient’s behalf in a variety of different situations (finances, investments, buying/selling property, managing a business, etc.) – Usually used to allow the agent to handle affairs during a period of time when the patient is physically or mentally unable to do so themselves. 3-56 Guardianship • A legal relationship in which the Court gives a person (the guardian) the power to make personal and health care related decisions for another (the ward). • A family member or friend may initiate the proceeding by filing a petition in the county where the individual resides. • A medical examination by a licensed physician is necessary to establish the mental capacity of the individual. 3-57 Guardianship • If the judge finds that the person does not have the necessary mental capacity to care for his or her personal needs, the judge will appoint a guardian to make personal decisions for the individual. • Unless limited by the court, the guardian has the same rights, powers and duties over his ward as parents have over their minor children. • The guardian is required to report to the court on an annual basis. 3-58 Organ Donation An organ donor is a patient who has completed a legal document that allows for donation of organs in the event of his death. A patient’s driver’s license may also indicate that the patient wishes to donate organs upon his death. EMT Role in Organ Donation Organ donor patients are treated the same as other patients. Identify potential donors. Notify medical direction. Provide care to maintain vital organs. Organ Donor Form Advance Directives and Do Not Resuscitate (DNR) Orders 3-62 Advance Directives • Any competent patient can refuse resuscitation • Advance directive – Legal document that specifies a person’s healthcare wishes when she becomes unable to make decisions for herself 3-63 Advance Directives • If you arrive on the scene to find a patient is not breathing and has no pulse and an advance directive is present: – Make sure the form clearly identifies the person to whom the DNR applies – Make sure the patient is the person referred to in the document – Make sure that the document you are viewing is of the correct type approved by your state and local authorities – If the document is valid, follow the instructions outlined in the document 3-64 Do Not Resuscitate (DNR) Orders • Different types of DNR orders exist – May specify that the patient does not want CPR or a shock to the heart – May want (and expect) oxygen and/or medications to be given – Alternately, may specifically state the patient does not wish any resuscitative measures 3-65 Advance Directive • Some states recognize only a specific form of advance directive for EMS personnel • An individual may wear an identifying bracelet on the wrist or ankle 3-66 Comfort Care • Providing comfort care means giving care to ease the symptoms of an illness or injury. • Comfort care includes – Emotional support – Suctioning the airway – Giving oxygen – Controlling bleeding – Splinting – Positioning the patient for comfort. 3-67 Physician Orders for Life-Sustaining Treatment (POLST) • POLST programs exist in some states • POLST form – Summarizes advance directives – Does not replace an advance directive – Is not conditional on losing decisionmaking capacity 3-68 Advance Directive • Obtain consent from the patient as long as he is able to make decisions about his healthcare 3-69 Assault and Battery • Assault – Threatening, attempting, or causing a fear of offensive physical contact with a patient or other individual • Battery – Unlawful touching of another person without consent 3-70 Duty to Act • May be a formal, contractual duty or an implied duty • A legal duty to act may not exist, but a moral or an ethical duty to act may exist 3-71 Abandonment • Terminating patient care without making sure that care will continue at the same level or higher 3-72 Negligence • Negligence – Deviation from the accepted standard of care, resulting in further injury to the patient • Four elements must be present to prove negligence: 1. There was a duty to act 2. The healthcare professional breached that duty 3. Injury and/or damages (physical or psychological) were inflicted 4. The actions of the healthcare professional caused the injury and/or damage (proximate cause) 3-73 Breach of Duty • Performing skills or treatments outside your scope of care can lead to a breach of duty • A breach of duty may be proved if you failed to act or you acted inappropriately 3-74 Damages • Damages occur if the patient is injured, either physically or psychologically, by your breach of duty 3-75 Proximate Cause • Proximate cause is established when: – Your action or inaction was the cause of or contributed to the patient's injury – You could reasonably foresee that your action or inaction would result in the damage 3-76 Protection Against Negligence Claims • Maintain a professional attitude and conduct • Provide skills and treatments within your scope of care • Maintain mastery of your skills • Participate in CE and refresher programs • Follow instructions provided by medical oversight authority • Follow standing orders or protocols • Provide patients with a consistently high standard of care • Make sure your documentation is thorough and accurate 3-77 Good Samaritan Laws and Immunity (1 of 2) • If you reasonably help another person, you will not be held liable for error/omission • Good Samaritan actions to be met: – Good faith – Without expectation of compensation – Within scope of training – Did not act in grossly negligent manner Good Samaritan Laws and Immunity (2 of 2) • Gross negligence is conduct that constitutes willful or reckless disregard. • There is another group of laws that grants immunity from liability to official providers. – Laws vary; always consult with the medical director. Confidentiality • Health Insurance Portability and Accountability Act (HIPAA) – Provides patients with control over their health information – Sets boundaries on use and release of medical records – Ensures the security of personal health information – Establishes accountability for medical record use and release 3-80 Confidentiality • Protected health information (PHI) is information that: – Relates to an individual’s physical or mental health, treatment, or payment – Identifies the individual or gives a reasonable basis to believe that the individual can be identified – Is transmitted or maintained in any format 3-81 Confidentiality • You must keep confidential: – Any medical history given to you in a patient interview – Any findings you may discover during your patient assessment – Any care that you provide 3-82 Confidentiality • Situations in which patient consent/authorization to the release of PHI is not required: – When you are required by law to provide this information – For public health activities, such as injury/disease control and prevention – When the patient is a victims of abuse, neglect, or domestic violence – For judicial and administrative proceedings – For specific law enforcement purposes – To avoid a serious threat to health or safety 3-83 Confidentiality • You may discuss your patient’s medical condition, the treatment you gave, and the patient’s health information with others involved in the medical care of the patient. 3-84 Medical Identification Insignia • Used to alert others of a particular medical condition that the patient has – May be a bracelet, a necklace, or an ID card 3-85 Medical Identification Devices Safe Haven Laws • Allow person to drop an infant or child at any fire, police, or EMS station • States have different guidelines for ages of children included • Protect children who may otherwise be abandoned or harmed by parents unwilling or unable to care for them Crime Scenes • A crime scene is the responsibility of law enforcement personnel • As an EMT, your responsibilities are to: – Ensure your own safety – Provide care for the patient 3-88 Crime Scenes • Responsibilities of medical personnel: – Protect potential evidence – Leave holes in clothing from bullet or stab wounds intact, if possible – Do not disturb any item at the scene unless emergency care requires it – Observe and document anything unusual 3-89 Crime Scenes • Location where crime was committed or anywhere evidence may be found • Once police have made scene safe, EMT’s priority is patient care • Know what evidence is • Take steps to preserve evidence Examples of Evidence • • • • Condition of scene Patient Fingerprints and footprints Microscopic evidence Evidence Preservation • • • • Remember what you touch Minimize impact on scene Work with police If patient transported on your stretcher, stretcher sheet may be valuable source of evidence • Document thoroughly Special Reporting Requirements • Child abuse • Elder abuse • Spousal abuse • Infectious disease exposure 3-93 Mandatory Reporting Guidelines • • • • • Child, elderly, or domestic abuse Sexual assault Stab/gunshot wounds Animal attacks Check local laws and protocols Mass Casualty Incidents 3-95 Organ Donation • Organ donor – A person who has signed a legal document to donate his organs in the event of his death • Your responsibilities: – Provide any necessary emergency care – Notify EMS or hospital personnel that the patient is a potential organ donor when you transfer patient care 3-96 Documentation 3-97 Prehospital Care Report (PCR) The prehospital care report may also be called the: – Patient care report – Run report – Encounter form – EMS form – Run sheet – Trip sheet – Incident report – Ambulance report 3-98 Uses of the Prehospital Care Report • Medical uses • Continuity of care • Legal document • Administrative uses • Educational and research uses • Quality management 3-99 Characteristics of Good Documentation 3-100 Complete • “If it is not written down, it was not done.” • “If it was not done, do not write it down.” 3-101 Clear and Concise • Your report should be clear and to the point. • Include enough detail so that you will be able to recall the events that occurred long after they happened. 3-102 Objective • Document facts – Facts should be supported by what you see, hear, feel, and smell. – Assessment findings such as vital signs, audible wheezing, guarding, restlessness, contusions, etc. – Observations of the surroundings such as during an MVC or suicide attempt. 3-103 Subjective • Document – The patient’s response to treatment. Such as “I’m breathing better now.” – The patient’s own description of their complaint. Such as “I’m having a hard time catching my breath.” – The patient’s own description of their pain. Such as “It feels like an elephant is sitting on my chest.” – The patient’s abnormal behavioral response. Such as “I just want to die.” 3-104 Timely 3-105 Accurate 3-106 Legible • Write neatly – Some interpret a sloppy report as a reflection of sloppy care. • Print if necessary. • When completing a paper report, use a ballpoint pen with black or blue waterproof ink. 3-107 Documentation “Red Flags” • It is incomplete • It is inaccurate • It is vague • It is illegible • Opinions are included • It has been altered • Labeling is used • The report is missing • It is late 3-108 Elements of the Prehospital Care Report • Administrative Information – Time incident reported to 9-1-1 – Time unit notified – Time of arrival at patient – Time unit left scene – Time of arrival at destination – Time of transfer of care 3-109 Elements of the Prehospital Care Report • Patient Information – Chief complaint – Mechanism of injury or nature of illness – Level of consciousness – Breathing rate and effort – Heart rate – Skin perfusion (capillary refill) for patients younger than 6 years old – Skin color and temperature – Systolic blood pressure for patients older than 3 years old 3-110 Administrative or Dispatch Information Section 3-111 Patient and Scene Information 3-112 Patient Assessment Section 3-113 Documentation General Guidelines 3-114 General Guidelines • Document important observations about the scene. • Document events in chronological order. • Document pertinent positives and pertinent negatives. • Use abbreviations only if they are standard and approved by your EMS system. 3-115 General Guidelines • Documentation of sensitive information • Document the emergency care delivered. – Time of each intervention – Who performed the skill – Patient’s response 3-116 General Guidelines • Document orders from medical direction. • Document changes in the patient’s condition. • Do not intentionally leave spaces blank. – Use “N/A” if information does not apply 3-117 Confidentiality 3-118 Confidentiality • The PCR and the information on it are considered confidential. – Patient confidentiality laws (HIPAA) • Distribute copies of the form per local and state protocol and procedures. 3-119 Falsification • Falsification of information on the PCR may: – Lead to suspension or revocation of certification/license – Lead to other legal action – Harm the patient 3-120 Error Correction 3-121 Documentation Formats 3-122 SOAP • Subjective findings • Objective findings • Assessment • Plan 3-123 CHART • • • • • Chief complaint History Assessment Rx (Treatment) Transport 3-124 Narrative • Short story in chronological order – Assessment findings – Pertinent historical information – Treatment – Patient responses – Transport data 3-125 Questions? 3-126 Review Questions 1. Define scope of practice, negligence, duty to act, abandonment, and confidentiality. 2. List several steps that must be taken when a patient refuses care or transportation. 3. List several types of evidence and ways you may act to preserve it at a crime scene. Street Scenes Was it appropriate not to include the information that the patient has AIDS during the radio report to the hospital? What is the obligation of these EMTs concerning the confidentiality of patient information? (cont.) Street Scenes Would you have handled the transfer of information differently? Would it be appropriate to tell all the hospital staff so they would know to take infection precautions? (cont.) Street Scenes Should the information that this patient has AIDS be shared with other EMS providers in case they get a call for this patient? (cont.) Street Scenes What are the principles for confidentiality that EMTs should always maintain? Chapter Review Chapter Review • Medical, legal, ethical issues part of every EMS call. • Morals are how a person expresses beliefs of right and wrong. • Consent may be expressed or implied continued Chapter Review • If a competent patient refuses care or transport, you should make every effort to persuade him, but you cannot force him to accept care or go to the hospital. • Negligence is failing to act properly when you have a duty to act. continued Chapter Review • Abandonment is leaving a patient after you have initiated care and before you have transferred the patient to a person with equal or higher training. Remember • EMTs must use good judgment and decisionmaking skills when dealing with patient consent and refusal. • Avoiding negligence implies using good judgment; critical thinking is an essential component for avoiding liability. continued Remember • EMTs hold responsibility for patients’ protected health information; exercising care when dealing with this information is a legal and ethical obligation. Questions to Consider • Define scope of practice, negligence, duty to act, abandonment, and confidentiality. • What steps must you take when a patient refuses care or transportation? • What types of evidence may be found at a crime scene? How should you act to preserve evidence? Critical Thinking • You respond to a motor vehicle crash and find a seriously injured patient. He has no pulse and you are about to begin CPR when someone says, “Don’t do that! He’s got cancer and a DNR!” No one has the DNR at the scene. Do you start CPR and transport the patient? Summary (1 of 8) • Consent is generally required from a conscious adult before care can be started. • Never withhold lifesaving care unless a valid DNR order is present. Summary (2 of 8) • A parent or legal guardian must give consent for treatment or transport of a minor. • Conscious, alert adults have the right to refuse treatment or withdraw from treatment. Summary (3 of 8) • Patient communication is confidential. • Advance directives, living wills, or health care directives are often used when a patient becomes comatose. • There are both definitive and presumptive signs of death. Summary (4 of 8) • A donor card or driver’s license indicates consent to organ donation. • Standard of care is established in many ways. • When your ambulance responds to a call or treatment is begun, you have a legal duty to act. Summary (5 of 8) • Negligence is based on duty, breach of duty, damages, and causation. • Abandonment is termination of care without the patient’s consent or provisions for transfer of care. • Assault is unlawfully placing a person in fear of immediate bodily harm. Summary (6 of 8) • Battery is unlawfully touching a person, which includes providing emergency care without consent. • Good Samaritan laws protect persons who stop to render aid. Summary (7 of 8) • Records and reports are important, particularly if a case goes to court. • You should know the special reporting requirements for abuse of children, the elderly, and others; injuries related to crimes; drug-related injuries; and childbirth. Summary (8 of 8) • You must meet legal and ethical responsibilities while caring for the patient’s physical and emotional needs. • As an EMT, a number of situations might cause you to end up in court. Review 1. You arrive at the scene of an elderly lady complaining of chest pain. In assessing her, she holds her arm out for you to take her blood pressure. This is an example of: A. implied consent. B. informed consent. C. expressed consent. D. emergency consent. Review Answer: C Rationale: Expressed consent (also called actual consent) is when the patient authorizes you to provide treatment and transport, either verbally or nonverbally. For example, a patient who holds out his or her arm to allow you take a blood pressure is nonverbally giving you expressed consent. Review (1 of 2) 1. You arrive at the scene of an elderly lady complaining of chest pain. In assessing her, she holds her arm out for you to take her blood pressure. This is an example of: A. implied consent. Rationale: Implied consent is limited to lifethreatening emergencies and is appropriate when a person is unconscious and/or delusional. B. informed consent. Rationale: Informed consent is when the patient has been told of the specific risks, benefits, and alternative treatments. Review (2 of 2) 1. You arrive at the scene of an elderly lady complaining of chest pain. In assessing her, she holds her arm out for you to take her blood pressure. This is an example of: C. expressed consent. Rationale: Correct answer. It is also known as actual consent. D. emergency consent. Rationale: This does not exist as a form of consent. Review 2. Which of the following is an example of abandonment? A. An EMT leaves the scene after a competent adult has refused care. B. An EMT transfers care of a patient to an emergency department nurse. C. An AEMT transfers care of a patient to a Paramedic. D. An EMR is transferred patient care from an AEMT. Review Answer: D Rationale: Abandonment occurs when patient care is terminated without the patient’s consent or when care is transferred to a provider of lesser training and level of certification. Review (1 of 2) 2. Which of the following is an example of abandonment? A. An EMT leaves the scene after a competent adult has refused care. Rationale: Mentally competent adults have the right to refuse treatment or withdraw from treatment at any time. B. An EMT transfers care of a patient to an emergency department nurse. Rationale: An EMT can transfer care to someone of equal or higher medical authority. Review (2 of 2) 2. Which of the following is an example of abandonment? C. An AEMT transfers care of a patient to a Paramedic. Rationale: An AEMT can transfer care to someone of equal or higher medical authority. D. An EMR is transferred patient care from an AEMT. Rationale: Correct answer Review 3. The unauthorized confinement of a person is called: A. assault. B. battery. C. false imprisonment. D. slander. Review Answer: C Rationale: False imprisonment is defined as the confinement of a person without legal authority or the person’s consent. Review (1 of 2) 3. The unauthorized confinement of a person is called: A. assault. Rationale: Assault is unlawfully placing a person in fear of bodily harm. B. battery. Rationale: Battery is touching a person or providing care without consent. Review (2 of 2) 3. The unauthorized confinement of a person is called: C. false imprisonment. Rationale: Correct answer. D. slander. Rationale: Slander is false and damaging information about a person that is communicated by the spoken word. Review 4. Failure of the EMT to provide the same care as another EMT with the same training is called: A. libel B. slander C. negligence D. abandonment Review Answer: C Rationale: An EMT could be held liable for negligence if he or she fails to provide the same care as another EMT with the same training would provide in the same situation. For example, if an EMT fails to give oxygen to a patient with shortness of breath (an intervention that is clearly indicated), he or she may be held liable for negligence. Review 4. Failure of the EMT to provide the same care as another EMT with the same training is called: A. Libel Rationale: Libel is making a false statement in a written form that injures a good person’s name. B. Slander Rationale: Slander is verbally making a false statement that injures a good person’s name. C. Negligence Rationale: Correct answer D. Abandonment Rationale: Abandonment is the abrupt termination of contact with a patient. Review 5. An 8-year-old boy was struck by a car, is unconscious, and is bleeding from the mouth. A police officer tells you that he is unable to contact the child’s parents. You should: A. continue to treat the child and transport as soon as possible. B. cease all treatment until the child’s parents can be contacted. C. continue with treatment only if authorized by medical control. D. only provide airway management until the parents are contacted. Review Answer: A Rationale: The child in this scenario is critically-injured and requires immediate treatment and transport; waiting until his parents are contacted wastes time and increases his chance of a negative outcome. If you are unable to contact a minor’s parents or legal guardian, you should proceed with care based on the law of implied consent. Review (1 of 2) 5. An 8-year-old boy was struck by a car, is unconscious, and is bleeding from the mouth. A police officer tells you that he is unable to contact the child’s parents. You should: A. continue to treat the child and transport as soon as possible. Rationale: Correct answer B. cease all treatment until the child’s parents can be contacted. Rationale: If a true emergency exists, then consent is implied. Review (2 of 2) 5. An 8-year-old boy was struck by a car, is unconscious, and is bleeding from the mouth. A police officer tells you that he is unable to contact the child’s parents. You should: C. continue with treatment only if authorized by medical control. Rationale: If a true emergency exists, then consent is implied. D. only provide airway management until the parents are contacted. Rationale: If a true emergency exists, then consent is implied. Review 6. An advance directive is: A. a set of specific guidelines that clearly defines the different types of consent. B. a formal list that defines by state law whether a patient has decision-making capacity. C. a written document that specifies the care you should provide if the patient is unable to make decisions. D. a verbal order given to you by a dying patient's family regarding whether treatment should be provided. Review Answer: C Rationale: An advance directive is a written document signed by the patient and a witness that specifies the medical care that should be provided if the patient loses decision-making capacity (ie, he or she is no longer deemed competent). Review (1 of 2) 6. An advance directive is: A. a set of specific guidelines that clearly defines the different types of consent. Rationale: An Advance Directive specifies the specific care a patient will receive and does not address any type of consent. B. a formal list that defines by state law whether a patient has decision-making capacity. Rationale: An Advance Directive document has already determined that a patient was competent to make decisions when the document was created and signed. Review (2 of 2) 6. An advance directive is: C. a written document that specifies the care you should provide if the patient is unable to make decisions. Rationale: Correct answer D. a verbal order given to you by a dying patient's family regarding whether treatment should be provided. Rationale: An Advance Directive is a written order that defines the patient’s medical decisions. Review 7. Which of the following patients is competent and can legally refuse EMS care? A. A confused young female who states that she is the president B. A man who is staggering and states that he only drank three beers C. A conscious and alert woman who is in severe pain from a broken leg D. A diabetic patient who has slurred speech and is not aware of the date Review Answer: C Rationale: A patient who is of legal age (18 in most states), is conscious, and is alert to person, place, time, and event, likely has decision-making capacity and can legally refuse EMS care. However, patients who are confused, possibly intoxicated, or delusional are not capable of making a rationale decision; therefore, you should provide care based on the law of implied consent. Review (1 of 2) 7. Which of the following patients is competent and can legally refuse EMS care? A. A confused young female who states that she is the president Rationale: You must assess whether this patient’s mental condition is impaired. B. A man who is staggering and states that he only drank three beers Rationale: You must assess whether this patient’s mental condition is impaired. Review (2 of 2) 7. Which of the following patients is competent and can legally refuse EMS care? C. A conscious and alert woman who is in severe pain from a broken leg Rationale: Correct answer D. A diabetic patient who has slurred speech and is not aware of the date Rationale: You must assess whether this patient’s mental condition is impaired. Review 8. You are treating a patient with an apparent emotional crisis. After the patient refuses treatment, you tell him that you will call the police and have him restrained if he does not give you consent. Your actions in this case are an example of: A. assault. B. battery. C. negligence. D. abandonment. Review Answer: A Rationale: Unlawfully placing a person in fear of immediate bodily harm (ie, having him restrained) without his consent constitutes assault. Unlawfully touching a person without his or her consent constitutes battery. Review (1 of 2) 8. You are treating a patient with an apparent emotional crisis. After the patient refuses treatment, you tell him that you will call the police and have him restrained if he does not give you consent. Your actions in this case are an example of: A. assault. Rationale: Correct answer B. battery. Rationale: Battery is unlawfully touching a person. This includes care without consent. Review (2 of 2) 8. You are treating a patient with an apparent emotional crisis. After the patient refuses treatment, you tell him that you will call the police and have him restrained if he does not give you consent. Your actions in this case are an example of: C. negligence. Rationale: Negligence is failure to provide the same care that a person with similar training would provide. D. abandonment. Rationale: Abandonment is the unilateral termination of care without the patient’s consent. Review 9. The EMT has a legal duty to act if he or she is: A. off duty and witnesses a major car accident. B. a volunteer, is on duty, and is dispatched on a call. C. paid for his or her services, but is not on duty. D. out of his or her jurisdiction and sees a man choking. Review Answer: B Rationale: The EMT—paid or volunteer—has a legal duty to act if he or she is on duty and is dispatched on a call, regardless of the nature of the call. If the EMT is off duty and/or out of his or her jurisdiction, he or she has a moral obligation to act, but not necessarily a legal one. Review 9. The EMT has a legal duty to act if he or she is: A. off duty and witnesses a major car accident. Rationale: This is a moral obligation to act and not a legal one. B. a volunteer, is on duty, and is dispatched on a call. Rationale: Correct answer C. paid for his or her services, but is not on duty. Rationale: Whether paid or volunteer, the EMT must be on duty. D. out of his or her jurisdiction and sees a man choking. Rationale: This is a moral obligation to act, and not a legal one. Review 10. Which of the following statements about records and reports is FALSE? A. Legally, if it wasn't documented, it was not performed B. A complete, accurate report is an important safeguard against legal problems C. An incomplete or untidy patient care report is evidence of incomplete or inexpert emergency medical care D. Your patient care report does not become a part of the patient’s hospital record because your treatment was provided outside the hospital Review Answer: D Rationale: One of your most important safeguards against legal problems is a complete, accurate report; if it wasn’t documented, it wasn’t done! Furthermore, an incomplete or untidy patient care report (PCR) suggests incomplete or inexpert medical care. The PCR becomes a part of the patient’s hospital medical record; even though your treatment was provided outside the hospital, the PCR ensures continuity of care in the hospital. Review (1 of 2) 10. Which of the following statements about records and reports is FALSE? A. Legally, if it wasn't documented, it was not performed Rationale: True. If it was not written, then it was not performed. B. A complete, accurate report is an important safeguard against legal problems Rationale: True. The most important safeguard against legal problems is a complete, accurate report. Review (2 of 2) 10. Which of the following statements about records and reports is FALSE? C. An incomplete or untidy patient care report is evidence of incomplete or inexpert emergency medical care Rationale: True. An incomplete or untidy report equals incomplete or inexpert emergency care. D. Your patient care report does not become a part of the patient’s hospital record because your treatment was provided outside the hospital Rationale: Correct answer