Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
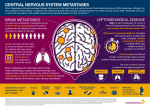
BRAIN IMAGING PRIOR TO LUNG CANCER RESECTION Dr Z Hudson Dr A Addeo Bristol Cancer Institute Bristol 24/05/16 Background 1.3.26 Consider MRI or CT of the head in patients selected for treatment with curative intent, especially in stage III disease. [new 2011] 1.3.27 Offer patients with features suggestive of intracranial pathology, CT of the head followed by MRI if normal, or MRI as an initial test. [new 2011] NICE 2011; Lung Cancer: Diagnosis and Management CG121 Hudson et al; 2015; Clinical radiology; 610-613 Methods • List of patients generated from pathology database • Search of ICE, including OpenNet for brain imaging • When patient out of area additional local searches • • • • • undertaken in Bath, Cheltenham and Gloucester for brain imaging Documentation of whether brain metastases present Documentation of date of radiological diagnosis with brain metastases Data subset created of patients with brain metastases identified and further analysis undertaken Data analysis using Microsoft Excel Poster presentation at BTOG Results (1) • 585 patients underwent lung resection between Jan 2012 and December 2014 • 471 with accessible radiology records • 25 patients had radiological evidence of brain metastases • 5 diagnosed concurrently with primary tumour and treated radically • 1 patient dual malignancies with brain metastases from bowel cancer more likely • 1 patient with clinical diagnosis of cerebral abscess Results (2) • 18 patients with radiological evidence of brain metastases that presented after their primary lung surgery • Appearance of brain metastases by days post resection Mean 371 days Range 14-1032 days Median 295 days • Date of metastases not available in two patients Results (3) • 4 presented within 6-12 months of resection • 2 no evidence of systemic relapse • 1 received SRS and is alive • 1 no information available • 2 local and nodal relapse • Both died after palliative chemotherapy • 5 presented within 6 months of resection • 2 no evidence of systemic relapse • 1 received SRS but died of pneumonia 1/12 later • 1 no outcome available • 3 no information available • 2 died • 1 alive Results (4) • Overall patients had 5.3% (25/471) chance of having radiological evidence of brain metastases • 3.8% (18/471) chance of having radiological evidence of brain metastases after surgery • 2% (9/471) of patients had radiological evidence of brain metastases within 12 months of their surgery • 1% (5/471) of patients had radiological evidence of brain metastases within 6 months of their surgery Brain metastases following radical surgical treatment of non-small cell lung cancer: Is preoperative brain imaging important? Lung Cancer ,November 2014 Volume 86, Issue 2, Pages185–189 • Methods • We performed a retrospective analysis of 646 patients who underwent surgery for lung • • • • • cancer with curative intent at a regional thoracic surgical centre in the United Kingdom. We identified those who developed brain metastases in the postoperative period and, by using volume doubling times, estimated the size of the metastasis at the time of surgery. We then determined the proportion of metastases that would have been seen on preoperative MR brain at detection thresholds of 2 and 5 mm diameter. Results There was a 6.3% incidence of postoperative brain metastases, with the majority occurring within 12 months of surgery. Those who developed metastases were more likely to have adenocarcinoma and the majority had early stage malignancy (73% stage I or stage II). We estimate that 71% of those who developed cerebral metastases might have been detected had they undergone MR brain as part of their staging (4.4% of all patients). Conclusion Based on our findings we suggest that, in addition to standard staging investigations, patients have brain imaging (MR or equivalent) prior to curative surgery in NSCLC regardless of preoperative stage. Discussion points • Is it time for a change? y/n • Which scan? • MRI/CT? • New PET-CT changes it?