Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
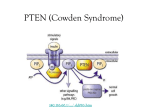
PTEN gene Associated Syndrome Name: PTEN Hamartoma Tumor syndrome (PHTS) PTEN Summary Cancer Risk Table CANCER GENETIC CANCER RISK Female Breast High Risk Colorectal High Risk Endometrial High Risk Melanoma High Risk Other High Risk PTEN gene Overview PTEN Hamartoma Tumor syndrome (PHTS) 1, 2, 3, 4 Individuals with PTEN mutations have PTEN Hamartoma Tumor Syndrome (PHTS). Women with PHTS have a risk for breast cancer that is significantly increased over the 12.5% lifetime risk for women in the general population of the United States. Individuals with PHTS also have a significantly increased risk for colorectal, endometrial, thyroid, renal and melanoma cancers. These cancers are often diagnosed at relatively young ages. A recent study has demonstrated that patients have a high risk for developing a second primary PHTSassociated cancer following their first diagnosis, and the risk may be particularly high for a second primary breast cancer. Patients with PHTS often have a wide variety of other, non-malignant features of the condition, some of which may require medical attention. Examples are macrocephaly, colorectal polyps of various types, Lhermitte-Duclos disease (a hamartomatous brain tumor), and distinctive skin findings such as trichilemmomas, acral keratoses and papillomatous papules. Developmental delay and/or autism spectrum disorders may also be present. A subset of patients with PHTS may have a diagnosis of other syndromes, such as Cowden Syndrome (CS), Bannayan-Riley-Ruvalcaba Syndrome (BRRS), PTEN-related Proteus Syndrome or Proteus-like Syndrome, based on other clinical features. Some of these conditions have features that may require intervention in infancy or childhood. Although there are high risks for cancer in patients with PHTS, these risks can be reduced with appropriate medical management. Guidelines from the National Comprehensive Cancer Network (NCCN) are listed below. Management of patients with PHTS poses challenges due to the complexity of the condition and it is recommended that patients with PTEN mutations and a diagnosis of PHTS be managed by a multidisciplinary team with expertise in medical genetics and the care of patients with hereditary cancer syndromes. 1 PTEN gene Cancer Risk Table CANCER TYPE AGE RANGE Overall cancer risk (male and female) To age 70 Female Breast To age 70 Endometrial To age 70 Thyroid To age 70 Colorectal To age 70 Renal To age 70 Melanoma To age 70 Other - Non-malignant features of PHTS All ages 6, 7 1, 6, 7, 8 1, 6, 8 1, 6, 7, 8 1, 6, 8 1, 6, 8 1, 7, 8 1, 2, 3 CANCER RISK RISK FOR GENERAL POPULATION 85%-89% 20.9% 77%-85% 7.3% 19%-28% 1.6% 21%-38% 0.8% 9%-16% 1.9% 15%-34% 0.8% Up to 6% 1.1% As described in the Overview above, PHTS is associated with nonmalignant clinical features, some of which may require medical intervention as early as infancy. NA PTEN Cancer Risk Management Table The overview of medical management options provided is a summary of professional society guidelines as of the last Myriad update shown on this page. The specific reference provided (e.g., NCCN guidelines) should be consulted for more details and up-to-date information before developing a treatment plan for a particular patient. This overview is provided for informational purposes only and does not constitute a recommendation. While the medical society guidelines summarized herein provide important and useful information, medical management decisions for any particular patient should be made in consultation between that patient and his or her healthcare provider and may differ from society guidelines based on a complete understanding of the patient's personal medical history, surgeries and other treatments. CANCER TYPE Overall cancer risk 2 PROCEDURE Comprehensive physical examination and general education about the signs and symptoms of cancer, with particular 1 attention to thyroid cancer. AGE TO BEGIN 18 years or 5 years before the youngest age of a PHTSrelated cancer in family FREQUENCY Annually CANCER TYPE Female Breast PROCEDURE AGE TO BEGIN Breast awareness - Women should be familiar with their breasts and promptly report changes to their healthcare provider. Periodic, consistent breast self-examination 1 (BSE) may facilitate breast awareness. 18 years NA Clinical breast examination 25 years, or 5 to 10 years younger than the earliest diagnosis in the family, whichever comes first. Every 6 to 12 months Mammography and breast MRI with contrast 30 to 35 years, or 5 to 10 years younger than the earliest diagnosis in the family, whichever comes first Annually Consider risk-reducing mastectomy. Individualized NA Patient education about endometrial cancer 1 symptoms. Individualized NA Consider endometrial sampling and 1 transvaginal ultrasound. 30 to 35 years Annually After completion of childbearing NA At time of PHTS diagnosis Annually 35 years, or 5 to 10 years younger than the earliest diagnosis in the family if a family member was diagnosed under age 40 Every 5 years 40 years Every 1 to 2 years 1 1 1 Endometrial Consider hysterectomy. 1 1 Thyroid Thyroid ultrasound Colorectal Colonoscopy Renal Consider renal ultrasound Melanoma Currently there are no specific medical management guidelines for melanoma risk in mutation carriers other than tailored dermatologic management as indicated by 1 skin findings. Individualized NA Other - Nonmalignant features of PHTS Comprehensive physical examination. Dermatologic management may be indicated for some patients. Consider psychomotor assessment in children and 1 brain MRI if there are symptoms. 18 years or earlier if symptoms are present Annually 1 Information for Family Members 3 FREQUENCY 1 The following information for Family Members will appear as part of the MMT for a patient found to have a mutation in the PTEN gene. A major potential benefit of myRisk genetic testing for hereditary cancer risk is the opportunity to prevent cancer in relatives of patients in whom clinically significant mutations are identified. Healthcare providers have an important role in making sure that patients with clinically significant mutations are informed about the risks to relatives, and ways in which genetic testing can guide lifesaving interventions. This patient's relatives are also at risk for the complications associated with Cowden Syndrome (CS), Bannayan-RileyRuvalcaba Syndrome (BRRS), PTEN-related Proteus syndrome and Proteus-like Syndrome, some of which may require medical attention in infancy or childhood. References 1. Daly M et al. NCCN Clinical Practice Guidelines in Oncology®: Genetic/Familial High-Risk Assessment: Breast and Ovarian. V 1.2017. September 19. Available at http://www.nccn.org. 2. Eng C. PTEN Hamartoma Tumor Syndrome (PHTS). 2016 June 2. In: Pagon RA, et al., editors. GeneReviews® [Internet]. Available from http://www.ncbi.nlm.nih.gov/books/NBK1488/ PMID: 20301661. 3. Pilarski R. Cowden syndrome: a critical review of the clinical literature. J Genet Couns. 2009 18:13-27. PMID: 18972196. 4. Ngeow J, et al. Second Malignant Neoplasms in Patients With Cowden Syndrome With Underlying Germline PTEN Mutations. J Clin Oncol. 2014 32:1818-24. PMID: 24778394. 5. Surveillance Research Program, National Cancer Institute SEER*Stat software (seer.cancer.gov/seerstat) V 8.0.1, Nov 19, 2012. 6. Riegert-Johnson DL, et al. Cancer and Lhermitte-Duclos disease are common in Cowden syndrome patients. Hered Cancer Clin Pract. 2010 8:6. PMID: 20565722. 7. Bubien V, et al. High cumulative risks of cancer in patients with PTEN hamartoma tumour syndrome. J Med Genet. 2013 50:255-63. PMID: 23335809. 8. Tan MH, et al. Lifetime cancer risks in individuals with germline PTEN mutations. Clin Cancer Res. 2012 18:4007. PMID: 22252256. Last Updated on 10-Jan-2017 4