Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Subventricular zone wikipedia , lookup
Human brain wikipedia , lookup
Environmental enrichment wikipedia , lookup
Metastability in the brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Aging brain wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Neuroanatomy wikipedia , lookup
Optogenetics wikipedia , lookup
Development of the nervous system wikipedia , lookup
Synaptogenesis wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Microneurography wikipedia , lookup
Central pattern generator wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Embodied language processing wikipedia , lookup
Circumventricular organs wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Channelrhodopsin wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Synaptic gating wikipedia , lookup
Muscle memory wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Motor cortex wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
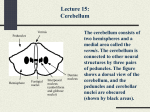
http://www.cogsci.bme.hu/~ktkuser/KURZUSOK/BMETE47MC23/2015_2016_2/ Kognitív idegtudomány Introduction to neurosciences for MSs. Motor system 3 Cerebellum Organization of the motor system Level 3 Cerebral cortex motor areas Basal Ganglia Level 2 Thalamus Brain Stem Cerebellum Spinal Cord Sensory receptors Muscles Contraction Level 1 Cerebellum Anatomy Two major fissures running mediolaterally divide the cerebellar cortex into three primary subdivisions: posterolateral fissure separates the flocculonodular lobe from the corpus cerebelli primary fissure separates the corpus cerebelli into a posterior lobe and an anterior lobe The cerebellum is also divided sagittally into three zones that run from medial to lateral: The vermis is located along the midsagittal plane of the cerebellum. Directly lateral to the vermis is the intermediate zone. lateral hemispheres are located lateral to the intermediate zone Cerebellar nuclei All outputs from the cerebellum originate from the cerebellar deep nuclei 1. fastigial nucleus: medially located. receives input from the vermis and from cerebellar afferents that carry vestibularproximal somatosensory, auditory, and visual information. projects to the vestibular nuclei and the reticular formation. 2. interposed nuclei: 3. dentate nucleus: 4. vestibular nuclei: emboliform nucleus and the globose nucleus. Situated lateral to the fastigial nucleus. receives input from the intermediate zone and from cerebellar afferents that carry spinal, proximal somatosensory, auditory, and visual information. project to the contralateral red nucleus. lateral to the interposed nuclei. receives input from the lateral hemisphere and from cerebellar afferents that carry information from the cerebral cortex. projects to the contralateral red nucleus and the ventrolateral (VL) thalamic nucleus. in the medulla. receive input from the flocculonodular lobe and from the vestibular labyrinth. project to various motor nuclei and originate the vestibulospinal tracts. Functional Subdivisions of the Cerebellum Vestibulocerebellum: Spinocerebellum: flocculonodular lobe oldest part of the cerebellum. vestibular reflexes and in postural maintenance. vermis and the intermediate zones major inputs from the spinocerebellar tract. output to rubrospinal, vestibulospinal, and reticulospinal tracts. integration of sensory input with motor commands to produce adaptive motor coordination. Cerebrocerebellum: largest functional subdivision, comprising the lateral hemispheres and the dentate nuclei. connections with the cortex. planning and timing of movements, cognitive functions of the cerebellum. Functions of cerebellum 1. Maintenance of balance and posture: 1. 2. Coordination of voluntary movements: 1. 3. coordinate the timing and force of muscles groups. Motor learning: 1. 2. 4. postural adjustments to maintain balance. adapting and fine-tuning motor programs to make accurate movements through a trial-and-error process (e.g., learning to hit a baseball). Cognitive functions: 1. language. 2. http://www.dailymotion.com/video/x1j0an_cerebellar-disease_news Citology Granule cells: Purkinje cells. receive input from mossy fibers and project to the Purkinje cells. the dendritic tree is flat, oriented in parallel. Golgi cell, the basket cell, and the stellate cell. Cerebellar Inputs and Outputs The cerebellum operates in 3’s: there are 3 routes in and out of the cerebellum there are 3 main inputs there are 3 main outputs from 3 deep nuclei. The 3 routes are the peduncles, or “stalks” - the rostral, middle and caudal cerebellar peduncles. Cerebellar Inputs and Outputs The 3 inputs are: mossy fibers from the spinocerebellar pathways and mossy fibers from the pons, carrying information from the contralateral cortex climbing fibers from the inferior olive Connectivity Mossy fibers: originate in the pontine nuclei, the spinal cord, the brainstem reticular formation, and the vestibular nuclei, excitatory projections onto the cerebellar nuclei and onto granule cells, each mossy fiber innervates hundreds of granule cells. Climbing fibers originate in the inferior olive make excitatory projections onto the cerebellar nuclei and onto the Purkinje cells Each Purkinje cell receives input from a single climbing fiber,extremely powerful, excitatory input onto Purkinje cells. Cerebellar Efferent Pathways To medullary and pontine regions of the brain stem – posture and equilibrium To thalamus (VL & VA), to cortex, to thalamus (midline), to basal ganglia, red nucleus, & reticular formation – coordination between agonists and antagonists To thalamus (VL & VA) to cortex – coordination of sequential motor actions Cerebellar Circuits Inputs to the cerebellar cortex (mossy and climbing fibers) excite the deep nuclei cells as they enter. The output of the CBL cortex (Purkinje cell axons) inhibits the deep nuclei cells. Climbing fibers excite Purkinje cell dendrites. Mossy fibers excite granule cells, whose axons (parallel fibers) excite Purkinje cell dendrites. Deep nuclei cells and Purkinje cells fire tonically. Cerebellar Circuits Cerebellar circuits Basket cell Stellate cell 4. Paralell fibers Golgi cell 3. 6. 5. Purkinje cell 2. Granulate cell Deep cerebellar nuclei cells Mossy fibers Climbing fibers 1. Spinal ch.,Vest. nuclei, cerebrum Motor output nucl. olivaris inferior kollaterals The Cerebellum - Claude Ghez W. Thomas Thach SZENTÁGOTHAI JÁNOS ÉS A KISAGYKUTATÁS Hámori József Cerebellum anatomy The Cerebellum - Claude Ghez W. Thomas Thach SZENTÁGOTHAI JÁNOS ÉS A KISAGYKUTATÁS Hámori József Diseases of the motor system Lower syndrome Upper motor syndrome Damages of the Basal ganglia Cerebellar damages Lower motor syndrome 1. 2. 3. 4. 5. 6. lower motor neurons refer to alpha motor neurons in the spinal cord and brain stem arises from certain diseases that selectively affect alpha motor neurons (such as polio) Muscle atrophy. (decrease in the mass of the muscle) Weakness. Fasciculation. spontaneous action potentials, visible twitch (called a fasciculation) Fibrillation. generate spontaneous action potentials; causing individual muscle fibers to contract, called a fibrillation. Hypotonia. (low muscle tone) Hyporeflexia. (below normal reflexes) Upper syndrome 1. 2. 3. 4. above the level of alpha motor neurons stroke, tumors, and blunt trauma Weakness. graded weakness of movement (paresis), which differs from the complete loss of muscle activity caused by paralysis (plegia). Hypertonia:. increased firing rate of alpha and/or gamma motor neurons. Hyperreflexia: Clonus: stretch reflex is so strong that the muscle contracts a number of times in a 5-7 Hz oscillation when the muscle is rapidly stretched and then held at a constant length. 5. Initial contralateral flaccid paralysis: contralateral side of the body shows a flaccid paralysis. 6. Spasticity: velocity dependent resistance to passive movement of the limb, 7. Babinski sign. normal in infants for the first 2 years of life. Paralysis: damage occurs at the cervical level, all four limbs will be paralyzed (quadriplegia). If the damage occurs below the cervical enlargement, then only the legs are paralyzed (paraplegia). Other terms used to describe patterns of paralysis are hemiplegia (paralysis to one side of the body) monoplegia (paralysis of a single limb). Disorders of the basal ganglia Dyskinesias 1. Resting tremors: Parkinson’s disease. 4-7 Hz tremor “pill-rolling tremor.” The tremor stops when the body part engages in active movement. https://www.youtube.com/watch?v=0-t4RTQ0EsM 2. Athetosis: is characterized by involuntary, writhing movements, especially of the hands and face. https://www.youtube.com/watch?v=J_wIDm1_ax4 3. Chorea: continuous, writhing movements of the entire body Huntington’s disease. 4. Ballismus: involuntary, ballistic movements of the extremities. http://www.dailymotion.com/video/x1j0an_cerebellar-disease_news 5. Tardive dyskinesia: involuntary movements of the tongue, face, arms, lips, and other body parts; https://teddybrain.wordpress.com/2013/01/18/differences-between-choreaathetosis-and-ballismus/ Disorders of the basal ganglia II. Akinesias 1. Rigidity: resistance to passive movement of the limb, does not depend on the speed of the passive movement. 2. Dystonia: involuntary adoption of abnormal postures, as agonist and antagonist muscles both contract and become so rigid that the patient cannot maintain normal posture. 3. Bradykinesia: slowness, or poverty of movement. Direct and indirect pathways The direct pathway travels from the striatum (GABA) directly to the internal segment of the globus pallidus or the substantia nigra pars reticulata.The isgp and the snpr project inhibitory (GABA) synapses to the thalamus. Result: Excitation of the thalamus -> excitation of the motor cortex -> movement excitation ((-1)+(-1)=+1)) The indirect pathway takes a detour from the striatum, (GABA) first to the external segment of the globus pallidus (GABA) and then to the subthalamic nucleus (Glu), before finally reaching the internal segment of the globus pallidus or the substantia nigra pars reticulata. The isgp and the snpr project inhibitory (GABA) synapses to the thalamus. Result: Inhibition of the thalamus -> inhibition of the motor cortex -> movement inhibition. ((–1)(–1) (+1) (–1) = –1). Direct- and indirect pathways Disorders of the basal ganglia Parkinson disease: 1. Slowness or absence of movement (bradykinesia or akinesia) 2. Difficulty in initiating a movement 3. Rigidity 4. Resting tremor Loss of dopaminerg neurons in the substantia nigra pars compacta projects to both direct pathway and indirect pathways neurons in the striatum; excites the direct pathway - to excite motor cortex, inhibits the indirect pathway- to inhibit motor cortex. The loss of the nigrostriatal dopaminergic pathway upsets the fine balance of excitation and inhibition in the basal ganglia and reduces the excitation of motor cortex. Treatement: L-dopa: precursor of dopamin; temporary, and typically symptoms return after a number of years lesions to the globus pallidus internal segment (pallidotomy) deep brain stimulation of the subthalamic nucleus https://www.youtube.com/watch?v=_L_WF6gv5BI Huntington disease: genetic disorder that is caused by an abnormally large number of repeats of the nucleotide sequence CAG on chromosome 4 effect of the mutation: loss of the indirect pathway neurons in the striatum, particularly in those of the caudate nucleus. Removal of inhibition from the external segment of the globus pallidus, allowing it to inhibit the subthalamic nucleus. Inhibition of the subthalamic nucleus produces a situation similar to a lesion of the subthalamic nucleus. Symptoms: 1. Choreidoform movements (involuntary, continous movements) 2. advanced stages is associated degeneration of both pathways and with dementia the excitatory effect of the direct pathway is no longer kept in check by the inhibition of the indirect pathway. Motor cortex gets too much excitatory input from the thalamus, sending involuntary movement commands to the brain stem and spinal cord. Inappropriate motor programs are not inhibited normally. No treatment https://www.youtube.com/watch?v=HOalYWvVLU8 Hemiballismus: unilateral lesion to the subthalamic nucleus, usually caused by a stroke (problems just on the contralateral side) Symptoms: involuntary, ballistic movements Treatment: surgical https://www.youtube.com/watch?v=hqg2GTUq1k4 Cerebellar syndrome 1. Ataxia: general impairments in movement coordination and accuracy Disturbances of posture: lesions to the vestibulocerebellum. difficulty in maintaining posture. Decomposition of movement: loss of the cerebellum’s ability to coordinate the activity and timing of many muscle groups to produce smooth, fluid movements. 2. Dysmetria: inappropriate force and distance that characterizes target-directed movements. 3. Dysdiadochokinesia: inability to perform rapidly alternating movements, such as rapidly pronating and supinating the hands and forearms. 4. Scanning speech: staccato nature of speech, difficulty in coordinating these muscle groups appropriately, speech is slow and disjointed. 5. Hypotonia: Cerebellar syndrome II. 1. Intention tremor: increasingly oscillatory trajectory of the limb in a target-directed movement Note that this tremor contrasts with the resting tremor of Parkinson’s disease. 2. Nystagmus: Vestibulocerebellum damage https://www.youtube.com/watch?v=phpe_RVGqcA 3. Delay in initiating movements: take longer to initiate movements, often because they must actively plan sequences of movements that are performed effortlessly by normal individuals. 4. Cognitive deficits: impaired ability to estimate time intervals. Born without cerebellum - The woman’s (24) condition was discovered after she sought medical attention due to nausea and vertigo. CT scans and MRI images revealed the missing cerebellum, which readily explains why those symptoms would be present. - wasn’t able to speak until she was six - wasn’t able to walk until age seven. She had never been able to play and jump like normal kids due to this defect. - had been unable to walk steadily without support - No trouble understanding vocabulary, but the missing cerebellum caused her to have difficulties with pronunciation. Her voice trembles, words are slurred, and the doctors described her voice tone as “harsh. - pons appeared underdeveloped http://brain.oxfordjournals.org/content/early/2014/08/22/brain.awu239 Over-Simplified Summary Motor cortex – initiation of movements Brain stem centers – balance of excitation and inhibition of antigravity muscles; integration of vestibular information Basal ganglia – posture and planning and coordination of motor action Cerebellum – equilibrium; coordination of motor action based on sensory information and feedback Literature Fonyó: Élettan orvosoknak Ádám – Fehér szerk.: Élettan biológusoknak James Knierim’s notes, Johns Hopkins University