Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
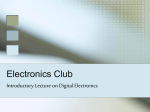
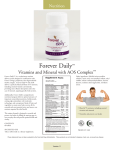
Storyboard Entry Form 2014 Main author: Hilary Williams Email: [email protected] Telephone: 02920316202 Follow the detailed instructions in this template for writing your storyboard. Add your information in each section below and save this completed storyboard document. Please not amend this template. Follow the instructions in the Information Guide for Authors to submit your storyboard. The word limit is 1100 words including references. Your storyboard will not be accepted if you exceed the word limit. 1. Storyboard title: a clear concise title which describes the work Working together across health boards to streamline services for emergency cancer care in SE Wales. 2. Brief outline of context: where this improvement work was done; what sort of unit/department; what staff/client groups were involved Our entry is a collaboration between Velindre Cancer Centre (VCC), Aneurin Bevan University Health Board (ABUHB) and the SE Wales Cancer Network (SEWN). Patients in SE Wales benefit from the internationally recognised cancer expertise of VCC. However there is increasing recognition that unscheduled care is frequently provided by acute teams in local LHB’s. Clinicians (ABUHB and VCC) were worried by patient’s experiences of variable care and in particular the lack of robust & timely links between the cancer centre and teams in ABUHB 3. Brief outline of problem: statement of problem; how you set out to tackle it; how it affected patient/client care Acute oncology (AOS) is a key priority for improvement in UK cancer care (ref 1). 3 groups of patients particularly benefit from early specialist cancer input following acute admission; patients with new a diagnosis of cancer (usually metastatic disease), those with complications of treatment (e.g. neutropenic sepsis), and those with complications of cancer (e.g. spinal cord compression). 4. Assessment of problem and analysis of its causes: quantified problem; staff involvement; assessment of the cause of problem; solutions/changes needed to make improvements The problem - baseline data The first collaborative step was demonstrating the local need for an AOS service in SEWN. Our ‘headline ’figures demonstrated a clear need, 10% of acute admissions in ABuHB have active cancer (e.g.6000 patients a year), lengths of stay were long; a mean of 12 days. Audits of key emergencies raised significant concern about patient safety (Life threatening Neutropenic Sepsis and Cord Compression). ABUHB Acute Admissions for Cancer Site of Colorectal Cancer Emergency Admissions This demonstrates complex pathways in unscheduled cancer care General surgery Gastroenterology Geriatric medicine Endocrinology General medicine Thoracic medicine Gynaecology Cardiology Infectious diseases Urology Accident and emergency Clinical haemotology Baseline audit against key AOS metrics Results of staff survey to demonstrate pre- AOS understanding of acute cancer related issues. Teams reported they regular cared for cancer patients but training in cancer emergencies was lacking. . The solution - hub and spoke model of acute cancer care. VCC developed a daily acute oncology meeting (the hub), supported by the VCC on call team, with teleconferencing to facilitate interaction with local hospitals. In parallel, we proposed a nurse led ‘in reach team’ who would ‘bridge the gap’ between ABUHB unscheduled care and VCC, and so fulfil requirements for AOS in Welsh Government Cancer strategy. Direct Clinical Role Support management complications of treatment Patient focused care Appropriate rapid decision making Rapid focused pathway cancer unknown primary Benefit- Patient Predict 5 patients admitted every 24 hours to ABH with known or likely cancer Benefit- Cost Reduced length stay Reduced investigations Reduced admissions Rapid liaison VCC & rapid access clinics 7day Service at RGH & NHH Costs Engage Palliative care Radiology Current pathways Education Admitting & A & E teams Link with Visiting Consultants 3 Specialist nurse Admin Office & Clinic space IT Protocols e. g. Unknown primary Spinal Cord Compression Education junior doctor teams Developmental Role - - 5. Strategy for change: how the proposed change was implemented; clear client or staff group described; explain how you disseminated the results of the analysis and plans for change to the groups involved with/affected by the planned change; include a timetable for change Proving the need. (Sep 2011- 12 months). The first challenge, was to prove a clear ‘invest to spend’ case. Local data was pivotal. We confirmed areas of concern; lengths of stays were long and patients underwent excessive diagnostic tests (ref 2). Pilot agreed. (March 2013, team started August 2013). A 1 year pilot, funding 3 senior cancer nurses was agreed. The key roles for the nursing team is to ensure rapid decision making (linking to VCC where necessary), compliance with AOS pathways and support for patients and families. Challenge – identifying patients admitted via multiple routes (March 2013 – ongoing) . One of key challenges of the pilot was to reduce length of stay and so improve patient experience and reduce cost. We developed 2 novel mechanisms to ensure rapid recognition of patients (first in Wales). All cancer patients in ABUHB are now flagged on the PAS system. This is cross linked daily with patient admissions to identify patients requiring review. Secondly we worked with radiology, to link patients with a new diagnosis of metastatic cancer directly to the nursing team, via alerts on radiology reports. Challenge – Education & 24/7 advise for acute teams (Jan – March 2013 ongoing). VCC set up an acute oncology intranet page, based on UK standards, with a linked page on ABUHB PAS. Our principal is advice must be ‘user friendly’ (e.g. available in ‘1 click’ and maximum of 2 pages). AOS teams have secured regular training programmes in ABUHB & VCC AOS Webpage This links to protocol flowcharts for common cancer-related emergencies Challenge – working more closely with the community. We have linked with the local community teams (GP and palliative care) to enable rapid assessment of patients. For example a patient with back pain was referred directly to AOS, had appropriate imaging of spine to exclude cord compression and was discharged within 24 hours. Developing this further is a key goal for 2014. 6. Measurement of improvement: details of how the effects of the planned changes were measured We have analysed results in terms of patient safety, resource use, and patient experience. Patient safety outcomes have been agreed using key metrics of AOS in and in line with English Peer Review measures. ABUHB measured their compliance with these standards before and after the implementation of the AOS service and showed marked improvements Neutropenic sepsis Metastatic Spinal Cord Compression Use of resource. We demonstrated both reduced length of stay and reduce number of investigations. Patient experience Feedback on the service:- Wife of patient (Ex Nursing Sister) called on Monday bank holiday stating that everything had been excellent on arrival to A&E on the previous Wednesday– Her husband had been seen swiftly in A&E – AOS nurse had met them on arrival as promised by the VCC chemo pager. Treatment was started immediately – “they already knew everything about my husband’s case, I didn’t have to explain anything – they were brilliant” 7. Effects of changes: statement of the effects of the change; how far these changes resolve the problem that triggered the work; how this improved patient/client care; the problems encountered with the process of changes or with the changes Analysis of the first 3 months of the service has shown marked improvement in key safety measures and objective improvements in LOS for all acute cancer patients. Interestingly, the service has become a central forum for development of care of acute cancer patients in ABUHB; increasingly teams, beyond those directly involved with the pilot, are working on finding solutions which are right for the patient rather than feeling frustrated with outdated pathways. 8. Lessons learnt: statement of lessons learnt from the work; what would be done differently next time One of the most positive outcomes has been flexible cross organisation and cross department working. For example, creative use of IT at both sites has led to new sustainable ways of working at minimal cost (Patient flag and radiology flag). Improving door to antibiotic time in neutropenic sepsis is challenging; having now used 1000 lives methodology in other areas of AOS, it would have been useful to use quality improvement methodologies earlier. 9. Message for others: statement of the main message you would like to convey to others, based on the experience described The Hub and Spoke pilot of the AOS service is a proven, cost effective model leading to real improvements in patient safety and experience by ensuring rapid access to treatment and care. This is a model that could transferred to other health boards, which would link in to VCC as the central hub. Key to the success has been honest analysis of the ‘baseline’ service, and real focus on developing service around the patient across organisational boundaries. We are now working with cancer teams throughout SEWN to support this critical development in all LHB’s. 1. 2. NCAG Chemotherapy services in England ensuring quality and safety Audit of Liver Biopsy of Patients with Malignancy of Undefined Primary Origin (ABUHB). Poster RCR 2013. The NHS Wales Awards are organised by the 1000 Lives Improvement Service in Public Health Wales. www.1000livesi.wales.nhs.uk