Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
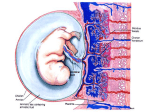
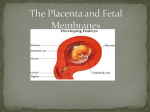
Development of the Placenta and Fetal Membranes Pregnancy is divided into 3 trimesters: First Trimester is called embryogenesis (organogenesis); the Second and Third Trimester are called fetal period Chorion, amnion, yolk sac, and allantois are fetal membranes that develop from zygote but do not form parts of embryo or fetus Placenta has fetal part (formed from chorion (synctiotrophoblast, cytotrophoblast, and extra-embryonic mesoderm)) and maternal part (formed from endometrium (decidua)) At end of 2nd week, cytotrophoblast cells of chorionic sac extend into synctiotrophoblast to form primary chorionic villi In 3rd week, mesenchyme (extra-embryonic mesoderm) grows into primary chorionic villi forming core of loose CT and thus becomes secondary chorionic villi Some of the mesenchyme differentiate into blood capillaries and blood cells thus becomes tertiary chorionic villi; these villi extend out to the cytotrophoblast shell and anchor chorionic sac to endometrium (these villi are stem villi (anchoring villi)); addnl branching from stem villi called free villi constitute main sites for gas exchange The rupture of maternal blood vessels and endometrial glands by the lacunae (spaces) of synctiotrophoblast marks the first stage of placental dvpt, thus maternal blood is surrounded by fetal synctiotrophoblast By the end of 3rd week, fetomaternal organ of placenta is established Implanting blastocyst and increasing progesterone levels in maternal blood cause decidual rxn in endometrial cells, which enlarge and become decidual cells (contain large amts of glycogen and lipids Decidua consists of three regions based on their relationship to implantation site: decidua basalis (maternal part of placenta; part of decidua that lies deep to embryo); deciduas capsularis (part of decidua overlying embryo); decidua parietalis (remaining endometrium) Up to the 8th week, villi cover entire chorion sac as the sac grows, the villi associated w/ decidua capularis (over top of embryo) becomes compressed with reduced blood supply and eventually degenerate leaving a bare area known as chorion leave (smooth chorion) the villi associate w/ decidua basalis increase rapidly in size and number making chorion frondosum (bushy or villous chorion), which becomes fetal part of placenta the decidua basalis forms maternal component of placenta By the 4th month, decidua basalis is almost completely replaced by chorion frondosum the decidua basalis forms a number of septa (decidua (placental) septa) which project into intervillous spaces but do NOT make contact w/ chorionic plate; septa have core of maternal tissue but surface is covered by layer of trophoblast cells (cytotrophoblast and synctiotrophoblast) thus maternal blood and fetal blood are separated at all times; decidual septa divide fetal part of placenta into a number of irregular compartments or cotyledons (each cotyledon has two or more stem villi (w/ their branches) endometrial arteries (spiral arteries) fill intervillous spaces w/ maternal blood and these spaces are drained by endometrial veins 2 placental circulations: fetal and maternal Fetal circulation deoxygenated blood leaves fetus in 2 umbilical arteries (these arteries branch freely in chorionic plate before entering villi; w/in villi they form an extensive capillary network, bringing fetal blood extremely close to maternal blood but there is NO mixing of maternal and fetal blood—always a barrier btw blood supply of mother and fetus) and passes to placenta via umbilical cord after passing through the placenta, the umbilical vein (only 1) collects oxygenated blood and returns it to fetus via umbilical cord umbilical vein is true vein and had all characteristics of vein (it is the only vein in the fetus to carry oxygenated blood—all other veins carry deoxygenated blood) Placental membrane always present but varies in thickness during gestation 10-20 wks consists of synctiotrophoblast, cytotrophoblast, connective tissue (mesenchyme), and endothelium of fetal capillary final placental membrane towards full term consists of synctiotrophoblast and endothelium of fetal capillary Maternal circulation maternal blood enters intervillous space through 80-100 spiral arteries which penetrate endometrium (decidua basalis) blood flow is pulsatile and under very high pressure which spurts toward roof of chorionic plate once here, pressure dissipates and blood flows slowly around surfaces of branched/free villi thus allowing gas and nutrient exchange to occur across placental membrane gaseous and metabolic waste products are in high concentration in fetal blood relative to maternal blood and so diffuse down their concentration gradient into maternal blood across placental membrane – conversely, oxygen and nutrients are in high concentration in maternal blood relative to fetal blood and so diffuse down their concentration gradient into fetal blood across placental membrane when blood reaches floor of intervillous space, it is drained by spiral veins and is returned to maternal circulation Three Placental functions Metabolism: especially during early pregnancy, placenta synthesizes glycogen, cholesterol, and fatty acids, which serve as sources of nutrients and energy for developing embryo/fetus Transport of nutrients and wastes by simple diffusion, facilitated diffusion, active transport, pinocytosis gases transported: O2, CO2, CO (interruption of O2 transport for even a few minutes will endanger fetal survival) nutrients transported: aas, carbohydrates (glucose), free fatty acids, vitamins, electrolytes (there is little or no transfer of maternal cholesterol, triglycerides, or phospholipids) hormones transported: steroidal hormones (protein hormones do not reach embryo/fetus) antibodies (many of the IgG class of abs are readily transported from maternal to fetal circulation; these maternal abs confer fetal immunity to such diseases as diphtheria, smallpox, measles—no immunity is acquired to pertussis or chicken pox) fetus does NOT produce its own abs until well after birth some blood may cross over and mix through microscopic breaks in the placental membrane most drugs and their metabolites cross placenta by simple diffusion (any drug taken by mother can affect embryo/fetus directly or indirectly; fetal drug addiction may occur after maternal use of drugs such as heroine and cocaine) thalidomide causes major congenital malformations specifically, limb and ear defects if taken during critical period of limb devpmt -24-36 days after fertilization viruses such as measles, rubella, and poliomyelitis may pass through placental membrane and cause fetal infection and thus congenital abnormalities and/or death (bacteria do NOT cross placental membrane) waste products transported: CO2, urea, uric acid, and bilirubin pass through placental membrane from fetus to maternal circulation by simple diffusion Endocrine secretion: placenta synthesizes human chorionic gonadotrophin (HCG) which maintains corpus luteum until placenta itself begins to produce its own estrogen and progesterone (HCG hormone used for pregnancy test in early development (2nd week)) other hormones synthesized include human placental alctogen (somatomammotropin) which promotes breast milk production and gives fetus priority on maternal blood glucose, human chorionic adrenocortocotropin (hACT), prolactin, relaxin, prostaglandins, progesterone, and estrogen Amnion forms fluid-filled sac that surrounds embryo and later fetus attached to margins of embryonic disc and hence its junction w/ the embryo (future umbilicus) is located on the ventral surface after embryonic folding as amnion increases in size, it fuses w/ chorionic membrane (serves two functions: 1) forms amniochorionic membrane, which ruptures upon initial stages of labor when “water breaks” 2) obliterates the chorionic cavity and enfolds the umbilical cord which connects the embryo/fetus to placenta w/ subsequent growth, amniochorionic membrane will fuse w/ decidua parietalis and thus obliterate the uterine cavity (decidua capularis thins and eventually degenerates) Amniotic fluid derived primarily from maternal blood and exchanged every 3 hrs indicating enormous exchange btw amniotic cavity and maternal circulation amniotic fluid increases gradually w/ a maximum of ~700-1000 mL at 37 wks fetus swallows its own amniotic fluid after 5th month the fetus swallows 400 mL per day fetus also contributes to amniotic fluid about 500 mL of urine in late pregnancy and about 400 mL from respiratory tract Function of Amniotic fluid: - permits symmetrical external growth of embryo/fetus - prevents adhesion of embryo/fetus to amnion - cushions embryo/fetus against jolts - helps control embryo’s/fetus’s body temperature - enables embryo/fetus to move freely - permits normal fetal lung development Oligohydramnios: condition defined by low volume of amniotic fluid (~400 mL 3rd trimester) can occur from placental deficiency caused by diminished placental blood flow, preterm ruptureof amniochorionic membrane which occurs in about 10% of cases and is most common cause, or renal agenesis (absence of kidneys) can cause pulmonary hypoplasia (small lungs), facial defects, and limb defects, mainly caused by the uterine compression of fetus these defects are symptoms of potter syndrome which also displays prominent infraorbital creases, a flattened nose, and excessive skin folds Polyhydramnios (hydramnios): condition defined by high volume of amniotic fluid, usually in excess of 2 liters can occur when fetus does not swallow usual amount of amniotic fluid can be associated w/ severe anomalies of CNS eg meroanencephaly and anencephaly and congenital anomalies of digestive system eg esophageal atresia all of these conditions prevent fetus from swallowing amniotic fluid Yolk sac connected to midgut by narrow yolk stalk very small and although it is nonfunctional as far as yolk storage is concerned, it is essential for 1) transfer of nutrients during 2nd and 3rd weeks before uteroplacental circulation established 2) blood cell development begins in its wall 3) part of the sac is incorporated into the wall of the gut 4) primordial germ cells arise here by 3rd week and then they migrate to developing gonads (once there they differentiate into germ cells (spermatogonia in males and oogonia in females) yolk stalk usually detaches from gut by end of 6th wekk and later the yolk stalk and sac atrophies persistence of yolk stalk occurs in about 2% of adults as an ileal divericulum known clinically as Meckel’s diverticulum Allantois appears on about day 16 as a small sausage shaped diverticulum (outpouching) from caudal wall of yolk sac that extends into connecting stalk (which later forms umbilical cord) allantois is large sac-like structure in embryos of reptiles, birds, and some mammals it has respiratory function and/or acts as a reservoir for urine during embryonic life in humans allantois remains very small and is not functional b/c placenta and amniotic sac take over its functions however it does have several important functions 1) blood cell formation occurs in its wall during 3rd to 5th week 2) its blood vessels become the umbilical vein and arteries 3) allantois forms first a thick tube called the urachus which after birth becomes a fibrous cord called the medial umbilical ligament this ligament extends from apex of urinary bladder to umbilicus