Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
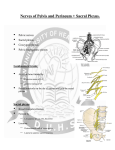
Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 1 of 12 All pelvic viscera receive dual innervation, meaning both sympathetic and parasympathetic contributions (visceral efferent fibers). When thinking about the autonomic innervation of the pelvic viscera, what should instantly spring to mind is the inferior hypogastric plexus. It is here, where all sympathetic and parasympathetic signals converge and are redistributed either directly to target organs within the pelvis or via smaller subsidiary plexuses. To use an analogy, the inferior hypogastric plexus can be compared in many ways to a main branch post office. A post office is responsible for taking in many types of correspondence from distant locations and redistributing them either directly to their final destinations, or to small branch post offices who then deliver them to their final destinations. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 2 of 12 In addition to parasympathetic and sympathetics, visceral afferent (sensory) fibers are often included during a discussion of autonomics because of their similar pathways of distribution. Visceral afferent (sensory) fibers also need to reach all organs within the pelvis. These fibers, originating within the spinal cord, accompany visceral efferent fibers throughout their pathways. Afferent fibers, important in reflex and visceral function, are also important in conducting visceral pain impulses. We are usually unaware of the sensory input of these fibers, which provides the central nervous system information about the condition of the body's internal environment. Conscious visceral sensation is usually categorized as pain and is poorly localized. (For more information, please see the introduction to autonomics module.) Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 3 of 12 In order to understand the autonomic innervation of the pelvis, one must recall that the sympathetic outflow of the autonomic nervous system (ANS) originates in the lateral or intermediolateral column of gray matter within the thoracolumbar region of the spinal cord (T1 through L2). Some sympathetic fibers travel in the sympathetic chain into the pelvis, while other sympathetic fibers enter the pelvis from the superior hypogastric plexus, which passes over the common iliac arteries. Recall that the different regions of the sympathetic chain are named according to the portion of the vertebral column along which the chain lies. So, there is a cervical, thoracic, lumbar, and a sacral portion of the sympathetic chain. Therefore sympathetics ultimately reaching the pelvis have descended into the inferior hypogastric plexus from the lumbar region. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 4 of 12 The inferior hypogastric plexus, the hub of all autonomic control within the pelvis, is a paired meshwork of nerves located on either side of the rectum lying medial to the internal iliac vessels. The sympathetic contributions into the inferior hypogastric plexuses stem from two sources. The largest sympathetic contribution is from the superior hypogastric plexus. The superior hypogastric plexus contains no parasympathetic fibers, so it is a purely sympathetic plexus. The superior hypogastric plexus itself receives upper lumbar contributions from the intermesenteric plexus, as well as contributions from L3 and L4 splanchnic nerves. Located within the abdomen at the bifurcation of the aorta, the superior hypogastric plexus descends into the pelvis and bifurcates as the right and left hypogastric nerves. Please note these "nerves" aren’t really what is traditionally thought of as a nerve, they are more like meshworks than solid nerve trunks. These nerve meshworks diverge lateral to the rectum on either side and curve outward and backward as they make their way down about 7.5 – 10 centimeters into the pelvis. They interconnect the superior and inferior hypogastric plexuses and contain no ganglia. The hypogastric nerves convey the majority of the sympathetic contribution from the superior hypogastric plexus into the inferior hypogastric plexuses. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 5 of 12 The second, much smaller, contribution of sympathetics to the pelvic viscera comes from the sacral splanchnic nerves. (Recall that a splanchnic nerve is a nerve, parasympathetic OR sympathetic, that brings innervation to viscera.) The sacral splanchnic nerves are very small, and are anteriorly directed branches from the sacral portion of the sympathetic chain. Just like the other splanchnic nerves in the thorax and abdomen, they leave the chains (on each side of the vertebral column) and course anteromedially into the inferior hypogastric plexus. These small, mostly postganglionic**, fibers are collected together, with the contribution from the respective hypogastric nerve, into the inferior hypogastric plexuses, from which postganglionic fibers are distributed to either smaller plexuses or directly to pelvic viscera. **Sympathetic outflow originates within the thoracic and upper lumbar region. The further a fiber travels away from this region, the less likely that it would remain preganglionic. For example, thoracic splanchnic nerves, coming directly off the sympathetic trunk, are primarily preganglionic and will synapse in a prevertebral ganglion. As one proceeds to lower level splanchnics, such as lumbar or sacral, the proportion of pre- to postganglionic fibers change. For this reason lower lumbar splanchnics will have a much higher proportion of postganglionic fibers than preganglionic fibers. By the time sacral splanchnics arise, they are mostly postganglionic fibers and have already synapsed prior to reaching the inferior hypogastric plexus. In all diagrams within this module sacral splanchnics will be represented as postganglionic fibers that are coming into the inferior hypogastric plexus. ***Don't forget gray rami communicantes. They travel laterally from the sacral sympathetic trunk to reach the sacral ventral primary rami. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 6 of 12 Now that the sympathetic contribution is accounted for within the inferior hypogastric plexuses, the parasympathetics can be considered. The pelvic splanchnic nerves represent the sacral contribution of the parasympathetic (craniosacral) outflow of the ANS. The pelvic splanchnic nerves contribute parasympathetic supply for the pelvic viscera, along with the parasympathetic supply to the hindgut, which begins at the distal third of the transverse colon (see abdomen module). Pelvic splanchnic nerves are preganglionic parasympathetic fibers whose cell bodies are located in a small lateral horn of gray matter in spinal cord levels S2, 3, and 4. These preganglionic fibers leave the lateral horn, and subsequently pass through the ventral horn, ventral root, spinal nerve, and ventral ramus associated with S2, 3, and 4. These fibers then directly branch off the ventral rami as pelvic splanchnic nerves and join the inferior hypogastric plexus. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 7 of 12 After all the parasympathetics and sympathetics have successfully reached the inferior hypogastric plexus they must still find their way to their final destinations and synapse in the correct locations. Recall that both sympathetics and parasympathetics are each two neuron systems, but that the location of synapses in each of these systems is very different. Most of the sympathetic fibers reaching the inferior hypogastric plexus are postsynaptic, having synapsed within the lower lumbar or sacral portions of the sympathetic trunk prior to leaving it. Those preganglionic sympathetic fibers that reach the inferior hypogastric plexus synapse within small, diffuse ganglia within this plexus and then send out postganglionic fibers to their target organs. Parasympathetics, on the other hand, travel through the plexuses, but wait to synapse until they reach the wall of their target organ and then send out very short postganglionic fibers. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 8 of 12 Sympathetics reaching the inferior hypogastric plexuses have several options for reaching their final destination. Most of these sympathetics are already postsynaptic, having synapsed within the sympathetic trunk before leaving it. They can proceed directly to their target organ. Sympathetic fibers that haven’t synapsed already will synapse in diffuse ganglion cells (not identifiable ganglia) within the inferior hypogastric plexus or its subsidiary plexuses and then travel on to their target viscera. Parasympathetics do the same, except as you know, they don’t synapse until reaching their target organ, so they simply travel through the inferior hypogastric plexus and its subsidiary plexuses. Subsidiary plexuses (which are really just extensions of the inferior hypogastric plexus) help the autonomics to more easily become distributed to pelvic viscera and as a whole are referred to as the pelvic plexuses. These subsidiary plexuses include the rectal, vesical, and the uterovaginal plexus in the female, and the prostatic plexus in the male. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 9 of 12 Autonomic Innervation of the Rectum: The rectal plexus is an offshoot of the posterior portion of the inferior hypogastric plexus. Nerves run from the inferior hypogastric plexus and penetrate the walls of the rectum providing enteric plexuses like those found in other parts of the intestines. Pelvic splanchnics (parasympathetics) innervate the internal anal sphincter that surrounds the upper twothirds of the anal canal. During most times the internal anal sphincter is tonically contracted to prevent leakage of feces. Following distention of the rectal ampulla, the sphincter relaxes and then it is the job of the external anal sphincter, which is under voluntary control and supplied by the inferior rectal branches of the pudendal nerve, to prevent defecation. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 10 of 12 Autonomic Innervation of the Bladder: The vesical plexus, the anterior portion of the inferior hypogastric plexus, forms loops around the end portion of the ureter and terminates within the bladder wall. Parasympathetic fibers (derived from pelvic splanchnics) travel through this plexus to provide motor innervation to the detrusor muscle and inhibitory signals to the internal sphincter. Therefore when the sensory fibers (visceral afferent) are stretched, the bladder contracts reflexively and the internal sphincter relaxes so urine can flow to the urethra. Sympathetics, on the other hand, cause vasoconstriction of renal vessels to slow urine formation and maintain contraction of the internal sphincter of the bladder to allow for urinary continence. The fibers of the vesical plexus, which also supply the fundus of the bladder, have offshoots to the seminal vesicle, the ductus deferens and the ejaculatory duct in the male. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 11 of 12 Autonomic Innervation of the Uterus: The uterovaginal plexus of the female stems from the intermediate part of the inferior hypogastric plexus. Its branches innervate the uterus, uterine tube, cervix and upper vagina. Sympathetic innervation originates in segments of the lower thoracic spinal cord and passes through lumbar splanchnics and the inferior mesenteric/hypogastric series of plexuses and finally to the uterovaginal plexus. Parasympathetic innervation originates in the S2 through S4 spinal cord segments and passes through pelvic splanchnics to the inferior hypogastric plexus and then into the uterovaginal plexus. (Remember that the pudendal nerve (S2-S4) does not carry parasympathetic fibers.) Visceral afferent fibers originating in the fundus and body of the uterus travel retrograde with sympathetics along the hypogastric nerves and superior hypogastric plexus to reach the lower thoracic segments of the spinal cord. Afferent fibers of the upper vagina and cervix travel back along the pelvic splanchnics (S2-S4) and on the pudendal nerve. Clinical Sidenote: There are several ways in which pain is regionally managed during childbirth. 1. A spinal block, in which anaesthetic agent placed into the L3/L4 subarachnoid space numbs everything inferior to the waist. In this case a mother would not be conscious of anything below her waist and would need to rely on electronic monitoring of uterine contractions to help deliver the baby. 2. Pudendal nerve block involves direct administration of anaesthetic agent into the nerve as it exits the greater sciatic foramen. This type of anaesthetic provides a nerve block over the S2 through S4 dermatomes only, which includes the perineum and the lower one-fourth of the vagina. It does not block pain felt from the body or fundus of the uterus because those afferent fibers travel retrograde along sympathetics heading to the thoracic region. By not numbing these regions, a mother can still feel contractions and play an active role in labor. 3. A caudal epidural block can be administered via an in-dwelling catheter into the sacral canal. Within the sacral canal, the agent bathes the sacral nerve roots, which reach the cervix, upper vagina and form the pudendal nerve. Copyright© 2002 The University of Michigan. Unauthorized use prohibited. Learning Modules - Medical Gross Anatomy Autonomics of the Pelvis - Page 12 of 12 Autonomic Innervation of the Prostate: The prostatic plexus of the male is derived from the larger nerves of the anterior portion of the inferior hypogastric plexus and lies alongside the prostate gland. It supplies the prostate gland, the prostatic urethra and the ejaculatory duct. The prostatic plexus also gives rise to the cavernous nerves of the penis, which are mainly parasympathetic and responsible for relaxation of smooth muscle allowing blood to flow into cavernous spaces in the corpora of the penis resulting in erection. Sympathetic stimulation causes ejaculation and vasoconstriction resulting in remission of an erection. An easy way to keep this straight is to remember that P arasympathteics = Point and Sympathetics = Shoot Copyright© 2002 The University of Michigan. Unauthorized use prohibited.