Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
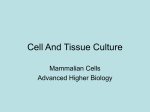
CLINICIAN’S CORNER Efficiency of a skeletonized distal jet appliance supported by miniscrew anchorage for noncompliance maxillary molar distalization Gero S. M. Kinzinger,a Norbert Gülden,b Faruk Yildizhan,c and Peter R. Diedrichd Homburg/Saar and Aachen, Germany Introduction: Conventional anchorage appliances rely exclusively on intraoral anchorage for noncompliance molar distalization. The partial coverage of the palate, in particular, often results in compromised oral hygiene. An innovative alternative combines a skeletonized distal jet appliance with 2 paramedian miniscrews for additional anchorage. The objectives of this study were to investigate the suitability of the skeletonized distal jet for translatory molar distalization and to check the quality of the supporting anchorage setup. Methods: Two paramedian miniscrews (length, 8-9 mm; diameter, 1.6 mm) were placed into the anterior area of the palate in 10 patients. Skeletonized distal jet appliances fitted with composite to the first premolars and the collars of the miniscrews were used for bilateral molar distalization, and the coil springs were activated with a distalization force of 200 cN on each side. Results: The study confirmed the suitability of the appliance for translatory molar distalization (3.92 6 0.53 mm) with slight mesial inward rotation (on average, 8.35 6 7.66 and 7.88 6 5.50 ). The forces acting reciprocally on the anchorage setup were largely absorbed by the anchorage unit involving 2 anchorage teeth and 2 miniscrews. Significant anchorage loss, in the form of first premolar mesialization of 0.72 6 0.78 mm, was found. Conclusions: The skeletonized distal jet appliance supported by additional miniscrew anchorage allows translatory molar distalization. Although the anchorage design combining 2 miniscrews at a paramedian location and the periodontium of 2 anchorage teeth does not offer the quality of stationary anchorage, it achieves greater molar distalization in total sagittal movement than conventional anchorage designs with an acrylic button. (Am J Orthod Dentofacial Orthop 2009;136:578-86) A s alternatives to the compliance-dependent headgear for maxillary molar distalization, appliances have been described that are worn only intraorally, are placed to remain fixed temporarily, and make treatment success independent of patient compliance. A major advantage for the patient, when comparing them with the extraorally anchored headgear, is the lack of esthetic impairment. One of these appliances is the distal jet (American Orthodontics, Sheboygan, Wis).1-3 The distal jet has, as its active components, 2 coil-spring systems that must be placed palatally. Loading the compression coil springs generates forces that preformed bands abduct a Professor, Department of Orthodontics, University of Saarland, Homburg/Saar, Germany. b Orthodontist, Department of Orthodontics, University of Saarland, Homburg/ Saar, Germany. c Orthodontist, Department of Orthodontics, RWTH Aachen, Aachen, Germany. d Professor and head, Department of Orthodontics, RWTH Aachen, Aachen, Germany. The authors report no commercial, proprietary, or financial interest in the products or companies described in this article. Reprint requests to: Gero Kinzinger, Department of Orthodontics, University of Saarland, Kirrberger Strabe 1, D-66421 Homburg/Saar, Germany; e-mail, [email protected]. Submitted, June 2007; revised and accepted, October 2007. 0889-5406/$36.00 Copyright Ó 2009 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2007.10.049 578 onto the permanent first molars and act distally. When it is accurately manufactured in the dental laboratory and anatomic relationships are favorable, the resultant lines of force are close to the centers of resistance of the molars. Therefore, as opposed to cervical headgear, which can achieve fractionated molar distalization only with combined coronal tipping and subsequent root uprighting, the biomechanics of the appliance should in theory enable it to perform almost translatory molar distalization.4 The reciprocally acting forces are therapeutically undesired and must be absorbed by intraoral anchorage. Conventionally, the anchorage setup of a distal jet appliance includes periodontal anchorage combined with further intraoral anchorage support: several teeth of the maxillary dentition are laced to an acrylic palatal button, by using bands or occlusal wire rests, to form an anterior anchorage unit. Because of the temporary partial coverage of the palate, in particular, which restricts hygiene capacity, this anchorage design has been the subject of critical discussion.5 Furthermore, certain dentition stages do not allow sufficient periodontal anchorage.6 As an alternative, a skeletonzed distal jet appliance supported by additional miniscrew anchorage could be used.5,7 It allows noncompliance molar distalization in the maxilla even with limited dental anchorage quality American Journal of Orthodontics and Dentofacial Orthopedics Volume 136, Number 4 Kinzinger et al 579 and, by dispensing with an acrylic button, also achieves better hygiene of the palatal mucosa. In an in-vitro study, Kinzinger and Diedrich4 demonstrated that the distal jet coil-spring systems allowed almost translatory tooth movement in the sagittal plane with uprighting effects on the dental root over a simulated distalization section of 3 mm based on a constant distalization force of 200 cN, combined with a mesial tipping moment. In the transverse plane, a force constantly directed toward the buccal aspect and a mesially rotating moment resulted in combined buccal movement and therapeutically undesired mesial and inward rotation of the permanent first molar. The aims of this in-vivo study were to investigate clinically the efficiency of the skeletonized distal jet supported by additional miniscrew anchorage and to compare the outcomes with the in-vitro series of measurements. A review of the literature resulted in a discussion of the share of anchorage loss in the total movement in the sagittal plane, hence of the quality of the miniscrew-supported periodontal anchorage setup, when comparing it with other conventional intraorally anchored, noncompliance distalization appliances. MATERIAL AND METHODS A skeletonized distal jet appliance was placed for bilateral molar distalization in the maxilla in 10 patients (8 girls, 2 boys; average age, 12 years 1 month) with dentoalveolar Class II malocclusion and dental archlength discrepancies. The mean treatment duration was 6.7 months. Of the total of 20 second molars, 11 were germinating, and 5 were erupting. Only 4 had already reached the occlusal plane. For the distal jet used in this study, the palatal acrylic button was removed as a means of anchorage. Instead, the modified appliance was anchored skeletally to 2 miniscrews placed into the palate at a paramedian location and, additionally, dentally to 2 occlusal rests. In terms of laboratory technique, this meant that prefabricated telescope spring assemblies, whose wings were bent distally to form occlusal rests, were connected to each other by using a soldered or laser-welded transverse wire (Fig 1). Every patient’s bone supply in the anterior area of the palate was analyzed on lateral cephalographs to determine the length of the screw shaft. After a preoperative mouth rinse with 0.1% chlorhexidine gluconate solution and local terminal anesthesia with an adrenalin-free anesthetic, 2 miniscrews with neck and collar (length, 8-9 mm, diameter, 1.6 mm; Forestadent, Pforzheim, Germany; or System Dual Top, Jeil Medical Corporation, Seoul, South Korea) were placed at a paramedian location in the anterior area of the palate (at the line of the first Fig 1. Skeletonized distal jet appliance supported by additional miniscrew anchorage: treatment of a girl aged 11 years 1 month; duration of distal jet treatment, 5 months. A, Occlusal view immediately after skeletonized distal jet placement: in terms of laboratory technique, prefabricated coil-telescope systems, the wings of which are bent distally to form occlusal rests, are connected to each other with a wire soldered to them. This transverse connecting wire is fitted dorsally to the miniscrew necks. B, Occlusal view after molar distalization: clinical assessment shows bodily molar distalization and spontaneous second premolar dental drifting. premolars) with a manual screwdriver and adequate sodium chloride cooling. No predrilling was performed. All miniscrews were tested for primary stability by using a probe; they were loaded a week after placement. Skeletonized distal jet appliances were attached to the premolars by using occlusal wire rests and to the necks of the miniscrews with transverse wires fitted dorsally and secured with composite. The occlusal rests also resulted in transverse reinforcement of the appliances. Accordingly, the anchorage setup consisted of a periodontal 580 Kinzinger et al American Journal of Orthodontics and Dentofacial Orthopedics October 2009 A UR2 UL2 N S Ar mb cf UL6 db UR6 ANS-PNS´ ANS A PNS Go-Me´ MPR Fig 2. Cast analysis (changes in the horizontal plane): angular and linear measurements to determine changes in the transverse width of the dental arch and rotation of the first molars. footing with the added support of miniscrews. The wings of the arc sections, which represent a bayonet bend, were fitted into the palatal sheaths of the molar bands. Then the loaded coil systems, with superelastic compression springs, were activated by fitting attachment screws dorsally with a distalization force of 200 cN for each system and reactivated every 4 weeks. To verify molar movement in the horizontal plane, plaster dental casts were taken at the start of treatment (T1) and after distal jet appliance removal (T2). The changes near the molars were assessed by measuring corresponding casts with a digital sliding caliper. Objects of analysis were changes in length of the supporting zone, increase or decrease of the transverse width of the dental arch at the line of the first molars, and extent and kind of tooth rotation. For every cast, the distance from the distal point of contact of the lateral incisor to the mesial point of contact of the first molar and, bilaterally, the distance from the lowest point of the central fossa to the mesiobuccal and the distobuccal cusps of the first molar were registered. In addition, the angles between a line running through the mesiobuccal and distobuccal cusps and the midpalatal raphe were measured (Fig 2). The cephalographs taken at T1 and T2 were analyzed to determine changes in the following parameters (Fig 3). 1. 2. 3. SNA: the angle between the anterior cranial base and the deepest point of the ventral concavity of the maxilla. SNB: the angle between the anterior cranial base and the deepest point of the ventral concavity of the mandible. S-N/ANS-PNS: the angle between the anterior cranial base and the palatal plane. Go B Me B N S P Pt PNS Or ANS Fig 3. Cephalometric analysis (changes in the sagittal plane): angles and distances registered on the lateral cephalograph before and after molar distalization: A, skeletal angular and linear values; B, dental angular and linear values. 4. 5. ANS-PNS/Go-Me: the angle between the palatal plane and the mandibular plane. Björk’s summation angle: the sum of the saddle angle (NSAr), the articular angle (SArGo), and the gonial angle (ArGoMe). Kinzinger et al American Journal of Orthodontics and Dentofacial Orthopedics Volume 136, Number 4 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. S-Go:N-Me: the facial height ratio (posterior face height to anterior face height). U1-CEJ/PTV: the distance from the maxillary central incisor to the pterygoid vertical. U4-CEJ/PTV: the distance from the maxillary first premolar to the pterygoid vertical. U5-CEJ/PTV, the distance from the maxillary second premolar to the pterygoid vertical. U6-CEJ/PTV: the distance from the maxillary first molar to the pterygoid vertical. U1/ANS-PNS: the angle between the maxillary central incisor and the palatal plane. U1/SN: the angle between the maxillary central incisor and the anterior cranial base. U4/ANS-PNS: the angle between the maxillary first premolar and the palatal plane. U4/SN: the angle between the maxillary first premolar and the anterior cranial base. U5/ANS-PNS: the angle between the maxillary second premolar and the palatal plane. U5/SN: the angle between the maxillary second premolar and the anterior cranial base. U6/ANS-PNS: the angle between the maxillary first molar and the palatal plane. U6/SN: the angle between the maxillary first molar and the anterior cranial base. U1-CEJ/ANS-PNS: the distance from the maxillary central incisor to the palatal plane. U4-CEJ/ANS-PNS, the distance from the maxillary first premolar to the palatal plane. U5-CEJ/ANS-PNS: the distance from the maxillary second premolar to the palatal plane. U6-CEJ/ANS-PNS: the distance from the maxillary first molar to the palatal plane. SNA, SNB, S-N/ANS-PNS, ANS-PNS/Go-Me, Björk’s summation angle, and the facial height ratio were measured or computed to verify any skeletal changes. In the sagittal plane, the relative incisor and first premolar mesial movement, hence the anchorage loss, and the relative second premolar and first molar distal movement in relation to the pterygoid vertical (U1-CEJ/PTV, U4-CEJ/PTV, U5-CEJ/PTV, and U6-CEJ/PTV) were determined. The respective points of reference for the measurements were the cementoenamel junction (CEJ) on the longitudinal axis of the teeth. Growthinduced changes (increase of 1 mm per year) were taken into account. The amounts of labial tipping of the incisors and first premolars and distal tipping of the second premolars and first molars were determined based on the angles between the longitudinal tooth axis and, respec- 581 tively, the palatal plane or the anterior cranial base (U1/ ANS-PNS, U1/SN; U4/ANS-PNS, U4/SN; U5/ANSPNS, U5/SN; U6/ANS-PNS, U6/SN). Potential tooth intrusions and extrusions were verified in the palatal plane (U1-CEJ/ANS-PNS, U4-CEJ/ ANS-PNS, U5-CEJ/ANS-PNS, and U6-CEJ/ANSPNS). Statistical analysis Statistical computations were performed with SPSS software (version 14, SPSS, Chicago, Ill). Casts and lateral cephalographs were traced twice at a 4-week interval. If values deviated, the means of both measurements were fed into the statistical analysis. Then the arithmetic mean and the standard deviation were computed for every variable used in the in-vivo measurements, and the changes of each variable from T1 to T2 were statistically analyzed with a 1-sample t test. Thereby, we determined which effective changes were therapeutically induced by the treatment as evidence against the null hypothesis. Differences with a probability of error less than 5% (P \0.05) were considered statistically significant. RESULTS Metrical assessment of the maxilla casts before and after molar distalization with a skeletonized distal jet appliance showed the following dental position changes of the permanent first molars (Table I). The supporting zones increased by 4.01 6 0.63 mm in the first quadrant and 3.64 6 0.69 mm in the second quadrant. The transverse widths of the dental arch increased by means of 1.79 6 1.08 mm between the mesiobuccal cusps, 2.58 6 0.69 mm between the central fossae, and 3.03 6 0.68 mm between the distobuccal cusps; this indicates both expansion and mesial inward rotation of the permanent first molars. When we looked more closely, the permanent first molars of the first quadrant had rotated mesiopalatally and distobuccally by a mean 8.35 6 7.66 and those of the second quadrant, by 7.88 6 5.50 . All position changes of the permanent first molars were significant. Skeletal assessments showed that the cranial base remained constant, with changes of the SNA angle of only a mean 0.19 6 0.80 and the SNB angle of only a mean 0.13 6 0.82 . The positional relationships of the palatal plane to the anterior cranial base and to the mandibular plane were virtually unchanged. Björk’s summation angle changed by only 0.73 6 1.26 during molar distalization, and the facial height ratio changed by 0.58% 6 1.51%. All registered skeletal changes during treatment were not significant (Table II). 582 Kinzinger et al Table I. American Journal of Orthodontics and Dentofacial Orthopedics October 2009 Changes in permanent first molar position induced by distal jet therapy in the horizontal plane Cast analysis n T1 mean T1 SD T2 mean T2 SD DT1-T2 mean DT1-T2 SD Significance UR2 distal-UR6 mesial (mm) UL2 distal-UL6 mesial (mm) Mesiobuccal cusp tips UR6-UL6 (mm) Central fossa UR6-UL6 (mm) Distobuccal cusp tips UR6-UL6 (mm) Tooth UR6 rotation ( ) Tooth UL6 rotation ( ) 10 10 10 10 10 10 10 20.80 21.17 50.80 45.80 53.06 12.86 13.43 2.04 1.90 2.16 2.36 1.70 6.15 4.29 24.81 24.81 52.59 48.39 56.09 21.21 18.93 2.34 2.08 1.28 2.04 1.49 6.28 5.94 –4.01 –3.64 –1.79 –2.58 –3.03 –8.35 –7.88 0.63 0.69 1.08 0.69 0.68 7.66 5.50 ‡ ‡ † ‡ ‡ * * Determination of type of molar rotation: angle between midpalatal raphe and a line running through the mesiobuccal and distobuccal cusps of the molars; for DT1-T2 (value before distalization) – (value after distalization): positive value 5 mesiobuccal and distopalatal rotation, negative value 5 mesiopalatal or distobuccal rotation. *P \0.05; †P \0.01; ‡P \0.001. Table II. Skeletal angular and linear measurements Cephalometric analysis Skeletal-angular SNA ( ) SNB ( ) S-N/ANS-PNS ( ) ANS-PNS/Go-Me ( ) Björk’s summation angle ( ) Skeletal-linear S-Go:N-Me (%) n T1 mean T1 SD T2 mean T2 SD D T1-T2 mean D T1-T2 SD Significance 10 10 10 10 10 83.55 79.83 5.56 24.20 389.61 2.63 3.42 1.92 4.31 3.29 83.36 79.70 5.18 25.08 390.34 2.78 3.27 1.53 4.14 3.49 0.19 0.13 0.38 –0.88 –0.73 0.80 0.83 1.18 1.09 1.26 NS NS NS NS NS 10 67.49 2.79 66.91 2.60 0.58 1.51 NS NS, Not significant. In the area of the CEJ, the permanent first molars were distalized by a mean of 3.92 6 0.53 mm and intruded by a mean of 0.16 6 0.26 mm. At the same time, they experienced distal tipping of 2.79 6 2.51 in relation to the palatal plane and 3.00 6 2.31 in relation to the anterior cranial base. The second premolars, which were not part of the anchorage setup, drifted distally after the molars by 1.87 6 0.74 mm, elongating by 0.42 6 0.41 mm and tipping, in relation to the respective reference planes, by 3.00 6 2.69 and 3.21 6 2.86 . The first premolars, included in the anchorage setup, mesialized by 0.72 6 0.78 mm, extruded by 0.14 6 0.14 mm, and, at the same time, tipped by 1.15 6 2.98 in relation to the palatal plane and by 0.79 6 2.23 in relation to the anterior cranial base. The central incisors were protruded by 0.36 6 0.32 mm and extruded by 0.14 6 0.29 mm, and showed slight labial tipping of 0.57 6 0.79 in relation to the palatal plane and 0.64 6 0.75 to the anterior cranial base. All linear dental movements in relation to the pterygoid vertical, the extrusion of the premolars, and the angular dental position changes of the second premolars and first molars were significant (Table III). The total movement in the sagittal plane was 4.28 6 0.51 mm (cumulating molar distalization and central incisor protrusion) or 4.64 6 1.06 mm (cumulating molar distalization and first premolar mesialization). Based on the values obtained for the permanent first molars— distalization length of a mean 3.92 6 0.53 mm—molar distalization represents 91.71% 6 7.32% and 86.56% 6 13.21%, respectively, of the total sagittal movement (Table IV). DISCUSSION The outcomes confirm the efficiency of the distal jet in clinical applications. Cast registrations showed that the supporting zone had increased, and that a therapeutically desired widening of the dental arch, as well as mesial inward and distal outward rotations of the molars, had occurred. The biomechanical explanation of this effect is that force is applied palatally from the center of resistance of the molars. In theory, a toe-in bend would be appropriate to compensate for this effect, but it results in friction in the guide tubes of the appliance. This effect was verified with the casts used and by an in-vitro registration. The resultant adhesive effect expressing this friction reduced the distalization force substantially and, accordingly, would be an obstacle for distalization of the molars. Therefore, a toe-in bend should not be used, although it would be therapeutically desirable.4 After the distal jet treatment, the molars Table III. 583 Kinzinger et al American Journal of Orthodontics and Dentofacial Orthopedics Volume 136, Number 4 Dental angular and linear measurements Cephalometric analysis Dental-angular U1/AN-PNS ( ) U1/SN ( ) U4/AN-PNS ( ) U4/SN ( ) U5/ANS-PNS ( ) U5/SN ( ) U6/ANS-PNS ( ) U6/SN ( ) Dental-linear U1-CEJ/PTV (mm) U4-CEJ/PTV (mm) U5-CEJ/PTV (mm) U6-CEJ/PTV (mm) U1-CEJ/ANS-PNS (mm) U4-CEJ/ANS-PNS (mm) U5-CEJ/ANS-PNS (mm) U6-CEJ/ANS-PNS (mm) n T1 mean T1 SD T2 M T2 SD D T1-T2 M D T1-T2 SD Significance 10 10 10 10 10 10 10 10 107.93 101.86 91.86 85.86 82.29 76.50 75.36 69.71 4.80 5.28 6.01 7.61 4.71 5.37 3.82 4.79 108.50 102.50 90.71 85.07 79.29 73.29 72.57 66.71 4.94 5.45 6.11 7.37 5.62 5.26 4.04 4.35 –0.57 –0.64 1.15 0.79 3.00 3.21 2.79 3.00 0.79 0.75 2.98 2.23 2.69 2.86 2.51 2.31 NS NS NS NS * * * * 10 10 10 10 10 10 10 10 52.54 38.47 31.21 22.59 17.96 15.79 14.59 13.16 2.94 3.37 3.11 3.31 2.62 1.53 2.06 1.78 52.90 39.19 29.34 18.67 18.10 15.93 15.01 13.00 2.98 3.78 3.00 3.11 2.44 1.55 1.97 1.65 –0.36 –0.72 1.87 3.92 –0.14 –0.14 –0.42 0.16 0.32 0.78 0.74 0.53 0.29 0.14 0.41 0.26 * * † ‡ NS * * NS *P \0.05; †P \0.01; ‡P \0.001; NS, not significant. Proportion of maxillary molar distalization in total movement in the sagittal plane Table IV. Cephalometric analysis Dental-linear (mm) U1-CEJ/PTV (mm) U4-CEJ/PTV (mm) U6-CEJ/PTV (mm) Total sagittal movement 1-6* Total sagittal movement 4-6† Calculation of ratio (%) Proportion of molar distalization in total sagittal movement 1-6‡ Proportion of molar distalization in total sagittal movement 4-6§ n D T1-T2 mean D T1-T2 SD 10 10 10 10 10 –0.36 –0.72 3.92 4.28 4.64 0.32 0.78 0.53 0.51 1.06 10 91.71 7.32 10 86.56 13.21 *Total movement in the sagittal plane 1-6 5 [U1-CEJ/PTV] 1 [U6CEJ/PTV]; †Total movement in the sagittal plane 4-6 5 [U4-CEJ/ PTV] 1 [U6-CEJ/PTV]; ‡Calculation: proportion of molar distalization in total sagittal movement 1-6 5 100 3 (U6-CEJ/PTV)/([U1CEJ/PTV] 1 [U6-CEJ/PTV]); §Calculation: proportion of molar distalization in total sagittal movement 4-6 5 100 3 (U6-CEJ/PTV)/ ([U4-CEJ/PTV] 1 [U6-CEJ/PTV]). should be derotated with an appropriate appliance, such as a transpalatal bar or a bi-helix. We found, during lateral cephalograph analysis, unlike the results of the in-vitro analysis, that the permanent first molars experienced slight dental crown tipping in the sagittal plane rather than root uprighting.4 The cause of this might be that the patients’ palatal vaults were not deep enough to enable placement of the loaded coil systems at the level of the center of resis- tance of the molars. Also, the location of the center of resistance can be determined only by approximation. Moreover, the respective development stages of the second molars might influence the extent of distal tipping of the first molars. In most patients in this study, the second molars were germinating or erupting. In a clinical study with pendulum appliances, Kinzinger et al8 showed that the extent of distal tipping is relatively greater when the second molars are only germinating. This phenomenon can be explained as follows: a germinating second molar has the same effect as a lever pivot point on the permanent first molar to be distalized; the first molar, when reacting to distalization, tips over the second molar germ. As its root is developing and the permanent second molar is erupting, the point of contact between the 2 molars gradually moves coronally. The tendency for the first molar to tip thereby decreases. Conventionally, the anchorage setup of exclusively intraorally anchored appliances for noncompliance molar distalization combines an acrylic button on the palatal mucosa with using the periodontium of anchorage teeth. The disadvantages of this kind of anchorage include, in particular, restrictions to hygiene5 and contraindications based on certain dentition stages and local situations.7 Moreover, it must be discussed how far the anchorage effect of an anteriorly placed Nance button potentially relies only on hydrodynamic interactions due to the resilient mucosa. Thereby it would be a disqualifying design for stationary anchorage designs, and hence must not be overestimated in terms of anchorage quality.5 584 Kinzinger et al Table V. American Journal of Orthodontics and Dentofacial Orthopedics October 2009 Studies using different conventionally intraorally anchored appliances for maxillary molar distalization Author/reference 31 Distalization appliance Angelieri et al Hilgers pendulum with uprighting activation Bolla et al32 Bondemark and Kurol33 Bondemark et al34 Bondemark and Kurol35 Bondemark36 Distal jet Magnets Magnets/supercoils Magnets/supercoils Magnets/NiTi coils Brickman et al37 Bussick and McNamara38 Byloff and Darendeliler39 Byloff et al40 Chaques-Asensi and Kalra41 Chiu et al42 Fortini et al43 Fuziy et al44 Jones jig Hilgers pendulum Hilgers pendulum Hilgers pendulum with uprighting activation Hilgers pendulum Distal jet/Hilgers pendulum FCA Hilgers pendulum Gosh and Nanda45 Gulati et al46 Haydar and Üner47 Joseph and Butchart48 Kinzinger et al50 Kinzinger et al8 Kinzinger et al50 Kinzinger et al51 Mavropoulos et al52 Ngantung et al53 Nishii et al54 Papadopoulos et al55 Hilgers pendulum Jones jig Jones jig Hilgers pendulum Pendulum K Pendulum K Pendulum K Pendulum K Jones jig Distal jet Distal jet Modified jig Treatment Soft-tissue subjects (n) support* Dental anchorage† 22 NP 20 10/10 18/18 18/18 21/21 NP NP NP NP NP 2 B PM1 2 OW PM2 2 B PM1 2 B PM2 2 B PM2 2 B PM2 2 B PM2 72 101 13 20 NP NP NP NP 2 B PM2 4 OW 4 OW 4 OW 26 32/32 17 31 NP NP NP NP 41 10 10 7 50 36 30 10 66 33 15 14 NP NP NP NP NP NP NP NP NP NP NP NP 2 B PM1 2 B PM2/4 OW 2 B PM2 2 B PM1 2 OW PM2 4 OW 4 B PM1 and PM2 2 B PM2 4 OW 4 OW 4 OW 4 OW 4 OW 2 B PM2 2 B PM2 2 B PM2 2 B PM2 Share of molar distalization in total movement (%) 35.7 PM1, 45.4 I 71.1 PM1 70 I 53.7 I/62.7 I 55 I/59 I 59.1 PM1, 57.8 I/67.6 PM1, 61.9 I 55.7 PM1 76.0 PM1 70.9 PM1 64.2 PM1 70.6 PM1; 71.8 I 51.8 PM1/81.3 PM 70.2 PM1; 76.9 I 63.5 PM1 56.9 PM1 55.0 PM1 45.0 PM1 57.9 I 72.5 I 70.2 I 76.3 PM1; 74.2 I 73.5 I 47.8 PM2; 51.3 I 44.9 PM2 63.1 PM1; 61.5 I 35 PM1, 37.8 I NiTi, Nickel-titanium; FCA, first-class appliance. * Intraoral anchorage designs: NP, Nance pad; B, premolar bands anchored to the Nance pad with connecting wires; OW, occlusal wire rests anchored to the Nance pad; PM1, first premolars; PM2, second premolars. † With specific reference: PM1, first premolar; PM2, second premolar; I, central incisor. Alternative anchorage components for molar distalization appliances include titanium miniscrews of small diameter and orthodontic implants of short length. In clinical application, short endosseous titanium implants provide quality stationary anchorage.9-13 So-called miniscrews, placed at a location paramedian to the palatal suture in the patients in this study, are less costly and, compared with short implants, can be placeed and removed with minimal invasion. Most clinical and experimental studies as well as case reports on anchorage with miniscrews deal with primary stability, rate of loss, and patient comfort of these implants.14-27 Only a few studies provide information on position stability of these anchorage components during orthodontic treatment. Liou et al28 and Kinzinger et al29 examined the anchorage quality of miniscrews subjected to orthodontic forces and concluded that, although they allowed stable anchorage, they did not fully maintain their positions under continuous loading. According to Park et al,30 some mobility in orthodontic screw implants does not necessarily mean that the outcome is compromised. Rather, even minimally mobile miniscrews can provide sufficient anchorage quality. Our results show that the described miniscrew-supported periodontal anchorage does not allow anchorage of stationary quality. Nevertheless, it offers essential advantages compared with conventional anchorage designs; by limiting the number of occlusal rests to 2, treatment is possible even with fewer teeth, with lower anchorage quality in the supporting zone. Spontaneous distal drifting of the second premolars, which were not part of the anchorage setup, reduced the length of the subsequent treatment phase. In this study, the second premolars drifted distally after the molars almost bodily American Journal of Orthodontics and Dentofacial Orthopedics Volume 136, Number 4 by 1.87 6 0.74 mm. In the subsequent active distalization of the anterior dentition, the molars can be anchored to the miniscrews. Various studies, in which different intraoral appliances with conventional anchorage designs (acrylic button and 2-4 anchorage teeth) were used for molar distalization, give the share of molar distalization in the total movement as 35% to 81.3% (Table V).8,31-55 The miniscrew-supported periodontal anchorage of the skeletonized distal jet used in this study, on the other hand, allows greater molar distalization in the total movement—91.71% and 86.56%; this is a reason that this innovative anchorage design makes sense as a treatment alternative. CONCLUSIONS In the sagittal dimension, the miniscrew-supported distal jet appliance allows almost translatory molar distalization. Because of the palatal force application from the center of resistance of the molars, the teeth experience therapeutically undesired mesial inward and distal outward rotation. The incorporation into the anchorage setup of 2 miniscrews at paramedian locations has the following advantages compared with conventional anchorage designs: by dispensing with an acrylic button that covers the palate, hygiene of the palatal mucosa improves. Additional dental anchorage requires only 2 teeth. The second premolars, which are not part of the anchorage, can drift distally spontaneously under the pulling effect of the transseptal fibers. Although a miniscrew-supported periodontal anchorage of a skeletonized distal jet appliance does not offer stationary anchorage quality, it allows a greater percentage of molar distalization in the total movement than do conventional anchorage designs with an acrylic palatal button. REFERENCES 1. Carano A, Testa M. The distal jet for upper molar distalization. J Clin Orthod 1996;30:374-80. 2. Bowman SJ. Modifications of the distal jet. J Clin Orthod 1998; 32:549-56. 3. Carano A, Testa M, Bowman SJ. The distal jet simplified and updated. J Clin Orthod 2002;36:586-90. 4. Kinzinger GSM, Diedrich PR. Biomechanics of a distal jet appliance. Theoretical considerations and in vitro analysis of force systems. Angle Orthod 2008;78:676-81. 5. Kinzinger G, Wehrbein H, Byloff KF, Yildizhan F, Diedrich P. Innovative anchorage alternatives for molar distalization—an overview. J Orofac Orthop 2005;66:397-413. 6. Kinzinger GSM, Wehrbein H, Gross U, Diedrich PR. Molar distalization with pendulum appliances in the mixed dentition: effects on the position of unerupted canines and premolars. Am J Orthod Dentofacial Orthop 2006;129:407-17. Kinzinger et al 585 7. Kinzinger GSM, Diedrich PR, Bowman SJ. Upper molar distalization with a miniscrew-supported distal jet. J Clin Orthod 2006;40:672-8. 8. Kinzinger GSM, Fritz UB, Sander FG, Diedrich PR. Efficiency of a pendulum appliance for molar distalization related to second and third molar eruption stage. Am J Orthod Dentofacial Orthop 2004;125:8-23. 9. Creekmore TD, Eklund MK. Possibility of skeletal anchorage. J Clin Orthod 1983;17:226-30. 10. Douglass JB, Killiany DM. Dental implants used as orthodontic anchorage. J Oral Implantol 1987;13:28-38. 11. Wehrbein H, Glatzmaier J, Mundwiller U, Diedrich P. The Orthosystem—a new implant system for orthodontic anchorage in the palate. J Orofac Orthop 1996;57:142-53. 12. Wehrbein H, Merz BR, Hämmerle CHF, Lang NP. Bone-toimplant contact of orthodontic implants in humans subjected to horizontal loading. Clin Oral Implants Res 1998;9:348-53. 13. Wehrbein H, Feifel H, Diedrich P. Palatal implant anchorage reinforcement of posterior teeth: a prospective study. Am J Orthod Dentofacial Orthop 1999;116:678-86. 14. Bae SM, Park HS, Kyung HM, Kwon OW, Sung JH. Clinical applications of micro-implant anchorage. J Clin Orthod 2002;36:298-302. 15. Böhm B, Fuhrmann R. Clinical application and histological examination of the FAMI screw for skeletal anchorage—a pilot study. J Orofac Orthop 2006;67:175-85. 16. Cheng SJ, Tseng IY, Lee JJ, Kok SH. A prospective study of the risk factors associated with failure of mini-implants used for orthodontic anchorage. Int J Oral Maxillofac Implants 2004;19:100-6. 17. Costa A, Raffaini M, Melson B. Miniscrews as orthodontic anchorage: a preliminary report. Int J Adult Orthod Orthognath Surg 1998;13:201-9. 18. Fritz U, Ehmer A, Diedrich P. Clinical suitability of titanium microscrews for orthodontic anchorage—preliminary experiences. J Orofac Orthop 2004;65:410-8. 19. Giancotti A, Arcuri C, Barlattani A. Treatment of ectopic mandibular second molar with titanium miniscrews. Am J Orthod Dentofacial Orthop 2004;126:113-7. 20. Herman RJ, Currier GF, Miyake A. Mini-implant anchorage for maxillary canine retraction: a pilot study. Am J Orthod Dentofacial Orthop 2006;130:228-35. 21. Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod 1997;31:763-7. 22. Kuroda S, Sugawara Y, Degushi T, Kyung HM, TakanoYamamoto T. Clinical use of miniscrew implants as orthodontic anchorage: success rates and postoperative discomfort. Am J Orthod Dentofacial Orthop 2007;131:9-15. 23. Lee JS, Park HS, Kyung HM. Micro-implant for lingual treatment of a skeletal Class II malocclusion. J Clin Orthod 2001;35:643-7. 24. Melson B, Costa A. Immediate loading of implants used for orthodontic anchorage. Clin Orthod Res 2000;3:23-8. 25. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano-Yamamoto T. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop 2003;124:373-8. 26. Park HS, Bae SM, Kyung HM. Micro-implant anchorage for treatment of skeletal Class I bialveolar protrusion. J Clin Orthod 2001; 35:417-22. 27. Wilmes B, Rademacher C, Olthoff G, Drescher D. Parameters affecting primary stability of orthodontic mini-implants. J Orofac Orthop 2006;67:162-74. 28. Liou EJW, Pai BCJ, Lin JCY. Do miniscrews remain stationary under orthodontic forces? Am J Orthod Dentofacial Orthop 2004;126:42-7. 586 Kinzinger et al 29. Kinzinger G, Gülden N, Yildizhan F, Hermanns-Sachweh B, Diedrich P. Anchorage efficacy of palatally inserted miniscrews in molar distalization with periodontally/miniscrew-anchored distal jet. J Orofac Orthop 2008;69:110-20. 30. Park HS, Jeong SH, Kwon OH. Factors affecting the clinical success of screw implants used as orthodontic anchorage. Am J Orthod Dentofacial Orthop 2006;130:18-25. 31. Angelieri F, Almeida RR, Almeida MR, Fuziy A. Dentoalveolar and skeletal changes associated with the pendulum appliance followed by fixed orthodontic treatment. Am J Orthod Dentofacial Orthop 2006;129:520-7. 32. Bolla E, Muratore F, Carano A, Bowman SJ. Evaluation of maxillary molar distalization with the distal jet: a comparison with other contemporary methods. Angle Orthod 2002;72:481-94. 33. Bondemark L, Kurol J. Distalization of maxillary first and second molars simultaneously with repelling magnets. Eur J Orthod 1992;14:264-72. 34. Bondemark L, Kurol J, Bernhold M. Repelling magnets versus superelastic nickel-titanium coils in simultaneous distal movement of maxillary first and second molars. Angle Orthod 1994;64:189-98. 35. Bondemark L, Kurol J. Class II correction with magnets and superelastic coils followed by straight-wire mechanotherapy. J Orofac Orthop 1998;59:127-38. 36. Bondemark L. A comparative analysis of distal maxillary molar movement produced by a new lingual intra-arch NiTi coil appliance and a magnetic appliance. Eur J Orthod 2000;22:683-95. 37. Brickman CD, Sinha PK, Nanda RS. Evaluation of the Jones jig appliance for distal molar movement. Am J Orthod Dentofacial Orthop 2000;118:526-34. 38. Bussick TJ, McNamara JA Jr. Dentoalveolar and skeletal changes associated with the pendulum appliance. Am J Orthod Dentofacial Orthop 2000;117:333-43. 39. Byloff FK, Darendeliler MA. Distal molar movement using the pendulum appliance. Part 1: clinical and radiological evaluation. Angle Orthod 1997;67:249-60. 40. Byloff FK, Darendeliler MA, Clar E, Darendeliler A. Distal molar movement using the pendulum appliance. Part 2: the effects of maxillary molar root uprighting bands. Angle Orthod 1997;67:261-70. 41. Chaques-Asensi J, Kalra V. Effects of the pendulum appliance on the dentofacial complex. J Clin Orthod 2001;35:254-7. 42. Chiu PP, McNamara JA Jr, Franchi L. A comparison of two intraoral molar distalization appliances: distal jet versus pendulum. Am J Orthod Dentofacial Orthop 2005;128:353-65. American Journal of Orthodontics and Dentofacial Orthopedics October 2009 43. Fortini A, Lupoli M, Giuntoli F, Franchi L. Dentoskeletal effects induced by rapid molar distalization with the first class appliance. Am J Orthod Dentofacial Orthop 2004;125:697-704. 44. Fuziy A, Rodrigues de Almeida R, Janson G, Angelieri F, Pinzan A. Sagittal, vertical, and transverse changes consequent to maxillary molar distalization with the pendulum appliance. Am J Orthod Dentofacial Orthop 2006;130:502-10. 45. Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofacial Orthop 1996; 110:639-46. 46. Gulati S, Kharbanda OP, Parkash H. Dental and skeletal changes after intraoral molar distalization with sectional jig assembly. Am J Orthod Dentofacial Orthop 1998;114:319-27. 47. Haydar S, Üner O. Comparison of Jones jig molar distalization appliance with extraoral traction. Am J Orthod Dentofacial Orthop 2000;117:49-53. 48. Joseph AA, Butchart CJ. An evaluation of the pendulum distalization appliance. Semin Orthod 2000;6:129-35. 49. Kinzinger G, Fuhrmann R, Gross U, Diedrich P. Modified pendulum appliance including distal screw and uprighting activation for non-compliance therapy of Class II malocclusion in children and adolescents. J Orofac Orthop 2000;61:175-90. 50. Kinzinger GSM, Gross U, Fritz UB, Diedrich PR. Anchorage quality of decidious molars versus premolars for molar distalization with a pendulum appliance. Am J Orthod Dentofacial Orthop 2005;127:314-23. 51. Kinzinger GSM, Wehrbein H, Diedrich PR. Molar distalization with a modified pendulum appliance—in vitro analysis of the force systems and in vivo study in children and adolescents. Angle Orthod 2005;75:558-67. 52. Mavropoulos A, Karamouzos A, Kiliaridis S, Papadopoulos MA. Efficiency of noncompliance simultaneous first and second molar distalization: a three-dimensional tooth movement analysis. Angle Orthod 2005;75:532-9. 53. Ngantung V, Nanda RS, Bowman SJ. Posttreatment evaluation of the distal jet appliance. Am J Orthod Dentofacial Orthop 2001; 120:178-85. 54. Nishii Y, Katada H, Yamaguchi H. Three-dimensional evaluation of the distal jet appliance. World J Orthod 2002;3:321-7. 55. Papadopoulos MA, Mavropoulos A, Karamouzos A. Cephalometric changes following simultaneous first and second maxillary molar distalization using a non-compliance intraoral appliance. J Orofac Orthop 2004;65:123-36.