Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
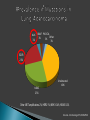
Amin Kay MD FRCPC Windsor Regional Cancer Center CME Support from Boehringer Ingelheim AstraZeneca Amgen Canadian Cancer Statistics 2014 Small Cell Lung Cancer Adenocarcinoma Non-Small Cell Squamous Cell Carcinoma Large Cell Carcinoma STAGE 4 Chemotherapy Targeted Therapies PD1 – PDL1 Pathway Anti-PD1 Antibody Improves survival Borghaei NEJM 2015 Borgahei NEJM 2015 Overall well-tolerated Autoimmune inflammation of any organ ◦ Managed with steroids and holding the drug Ou. Crit Rev Oncol Hematol 2012;83:407-21 ALK 3% BRAF PIK3CA Other 3% 3% 3% EGFR 23% Undetected KRAS 40% 25% Other: MET amplifications 2%; HER2 1%; MEK1 0.4%; NRAS 0.2% Kris et al. J Clin Oncology 2011;29:CRA7506 Non-Smoker Female Asian UP TO Squamous: Only 1%, so don’t bother checking. 1% 3% 2% 2% 1% 0% 0% Exon 21, N=13 L858R 40% 1% 0% 1% Del 19 L858R Exon 20 ins Exon 19 L858R + deletions T790M L861Q 49% G719X Pao et al. PNAS 2004;101:13306-11 Sequist et al. Presented at the 2012 Multidisciplinary Symposium in Thoracic Oncology, Chicago, IL; Sept 6-8 Can anyone name a first line EGFR inhibitor used in lung cancer? GEFITINIB ERLOTINIB AFATINIB Once daily pills Response ~ 1 year Survival: ~2 years vs 1 year “…patients with NSCLC who are being considered for first-line therapy with an EGFR TKI… should have their tumor tested for EGFR mutations to determine whether an EGFR TKI or chemotherapy is the appropriate first-line therapy.” PCR Keedy et al. J Clin Oncol 2011;29:2121-7 GEFITINIB CT scans before and after erlotinib therapy. Pan M et al. (2007) CNS response after erlotinib therapy in a patient with metastatic NSCLC with an EGFR mutation Nat Clin Pract Oncol 4: 603–607 doi:10.1038/ncponc0931 ERLOTINIB AFATINIB • • • • Irreversible More targets (EGFR subtypes) More potent More toxic AFATINIB GEFITINIB LUX-LUNG 7 Resistance develops within ~10 months OSIMERTINIB Janne NEJM 2015 ROCILETINIB Sequist NEJM 2015 • Moisturizer • Minimize sun, Sunscreen • Hydrocortisone 2.5% BID • Clindamycin 1% BID • Minocycline 100mg BID Correlation between rash severity and response • If severe: hold TKI, resume at lower dose Hirsh. Curr Oncol 2011;18:126-38 Inflammation/Infection of nail folds Avoid trauma, wear gloves when working with hands Emollient lotion Topical antibiotics (eg. Clinda 1%) Topical Steroid (Clobetasol) Vinegar Soak If severe: ◦ Oral Doxycycline ◦ Silver nitrate ◦ Removal of nail Plate • http://www.oncolink.org/experts/article.cfm?id=250 • Melosky & Hirsh, Frontiers in Oncology, 2014 Thinning Change in colour (Re-pigmentation) thickness Curling Fragility Eyebrows and lashes too Soft non-irritating foods Soft Toothbrush Normal saline or Sodium Bicarb (baking soda) rinse Miles Solution (steroid, lidocaine, nystatin) Assess for thrush and herpes GI tract epithelial cells express EGFR Secretory diarrhea Assess for other causes (laxatives, antibiotics, Stool Cx / C.diff, …) Assess volume status, electrolytes Diet Modification: ◦ BRAT diet ◦ Avoid milk products, fatty/spicy foods Keep hydrated Loperamide Admit to Hospital IV Hydration, Electrolyte repletion Continue Imodium Consider Octreotide Rule out other causes (eg. C.diff, Imaging, Scope) Hold drug ◦ Restart at lower dose when improves to grade 1. ◦ Watch out for flare when holding TKI. ALK 3% BRAF PIK3CA Other 3% 3% 3% EGFR 23% Undetected KRAS 40% 25% Other: MET amplifications 2%; HER2 1%; MEK1 0.4%; NRAS 0.2% Kris et al. J Clin Oncology 2011;29:CRA7506 FISH CRIZOTINIB Visual effects: • Visual persistence (trailer), halos • Self-limited, no intervention required • Pneumonitis • Bradycardia CERITINIB ALECTINIB More potent, better CNS response.