Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
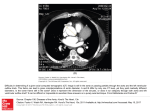
CTA for Pre TAVR Evaluation with Low Contrast Dose Tariq A Hameed, M.D. Indiana University School of Medicine Indianapolis, Indiana Co-authprs: Aashish Patel, M.D. Jonas Rydberg, Disclosures: No relevant financial disclosure Preprocedure Evaluation for TAVR • Aortic Valve Annulus – ECG gated Imaging • Aorta and Iliac arteries Contrast-Induced Nephropathy • The risk is higher – in patients with pre existing renal insufficiency – with higher contrast dose CTA with Low Contrast Dose 18 – 35 mL Goal • Achieve adequate contrast enhancement in aorta and iliac arteries Contrast Enhancement in Aorta X-Ray beam energy (KVp) 80 > 100 > 120 > 140 Need for 40% less iodine 120 kVp 80 kVp 240 HU 240 HU 100 ml 62 ml 80KVp technique (k-edge of Iodine) Iodine - relative attenuation relative mass attenuation coefficient Relative no. of photons and 1,0 K-edge 33.2 keV 0,8 80 kVp x-ray spectra 0,6 120 kVp x-ray spectra 0,4 0,2 0,0 20 40 60 80 100 120 Photon energy (keV) Courtesy: Ulf Nyman, MD, Trelleborg, Sweden • High noise • High noise High mAs Contrast Enhancement in Aorta • Iodinated Contrast – Volume – Concentration Contrast Enhancement in Aorta Iodinated contrast Injection rate Kyongtae T. Bae; Radiology 2010, 256, 32-61 Contrast Enhancement in Aorta Time of Imaging (scan delay) relative to arrival of contrast Figure 8a: Simulated contrast enhancement curves of the (a) abdominal aorta and (b) liver based on a hypothetical adult male (30 years old; weight, 70 kg; height, 170 cm) subjected to three volumes (75, 125, and 175 mL) of contrast medium (350 mg of iodine per milliliter) injected at the same rate of 2 mL/sec. A larger volume requires a longer duration to inject. Both the time to and the magnitude of the peaks of enhancement increase with the contrast medium volume (injection duration). Radiology, http://pubs.rsna.org/doi/abs/10.1148/radiol.10090908 Published in: Kyongtae T. Bae; Radiology 2010, 256, 32-61. DOI: 10.1148/radiol.10090908 © RSNA, 2010 One PowerPoint slide of each figure may be downloaded and used for educational, non-promotional purposes by an author for slide presentations only. The RSNA citationKyongtae line must appear in at least 10-point type on all256, figures32-61 in all T. Bae; Radiology 2010, presentations. Pharmaceutical and Medical Education companies must request permission to download and use slides, and authors and/or publishing companies using the slides for new article creations for books or journals must apply for permission. For permission requests, please contact the publisher at [email protected] Kyongtae T. Bae; Radiology 2010, 256, 32-61 Contrast Enhancement in Aorta • Patient size – Decreased enhancement with higher BMI/weight Bae et al, AJR 2008 190:3, 777-784 Contrast Enhancement in Aorta • Patient size – Decreased enhancement with higher BMI/weight • Cardiac Output – Higher enhancement with low cardiac output Cardiac Output Figure 7a: Simulated contrast enhancement curves of the (a) abdominal aorta and (b) liver based on a hypothetical adult male (30 years old; weight, 70 kg; height, 170 cm) who underwent injection of 125 mL of contrast agent (350 mg of iodine per milliliter) at 4 mL/sec. A set of aortic and hepatic contrast enhancement curves was generated by reducing the baseline cardiac output (CO) by 20%, 40%, and 60%. With a reduced cardiac output, contrast material bolus arrives slowly and clears slowly, resulting in delayed contrast material bolus arrival and delayed and elevated peak arterial and hepatic parenchymal enhancement. Radiology, http://pubs.rsna.org/doi/abs/10.1148/radiol.10090908 Published in: Kyongtae T. Bae; Radiology 2010, 256, 32-61. DOI: 10.1148/radiol.10090908 © RSNA, 2010 One PowerPoint slide of each figure may be downloaded and used for educational, non-promotional purposes by an author for slide presentations only. The RSNA citation line must appear in at least 10-point type on all figures in all presentations. Pharmaceutical and Medical Education companies must request permission to download and use slides, and authors and/or publishing companies using the slides for new article creations for books or journals must apply for permission. For permission requests, please contact the publisher at [email protected] Bolus triggering - wasting of CM Up to 6 seconds of bolus train can be wasted! TIMING RUN replaces bolus triggering Determine the exact time it takes for the contrast media to reach a certain anatomical location. Contrast media Volume: Injection rate: Saline Push Volume: Injection rate: 1 ml – 2 ml 3.5 ml / sec 30 ml 3.5 ml / sec CT Imaging Protocol 1. CT scanner with capability for high tube current and fast imaging 2. Retrospective ECG gated imaging of Thoracic Aorta. - Run the scan to the groins! 3. Routine helical CTA imaging of abdominal aorta and iliac arteries (This scan may not be necessary if first scan is successful) Case 1 - 35 mL • • • • • • 80 KVp mAs 1500 Total contrast media volume 35 mL 2 Timing runs Chest-Abdomen scan (cardiac gated) Pelvic scan (not cardiac gated) Timing Run 1 1 ml @ 3.5 mL/sec + saline chase 16 sec 35 Timing Run 2 2 ml @ 3.5 mL/sec + saline chase 16 sec 35 22 sec Chest-Abdomen 20 mL Contrast Media 370 mg/mL 1. 10 mL @ 3.5 ml/sec 2. 10 mL @ 2.0 ml/sec - 3 sec bolus train - 5 sec bolus train Total bolus train 8 sec Saline chaser 20 mL @ 2.0 mL/sec 35 Start scan near back end of bolus train 16 sec + 8 sec = 24 sec Start scan from above arch at 22 sec 35 Ascending Aorta and Iliac arteries 35 Postprocessing for annulus size + distance to coronary arteries 35 Pelvic imaging 12 ml Contrast Media 370 mg/mL 1. 10 ml @ 3.5 mL/sec 2. 2 ml @ 2.0 mL/sec Saline chaser 25 ml @ 2.0 mL/sec 35 Case 2 - 31 mL (1+2+15+13) TIMING RUNS 31 Contrast media Timing run 1 (Asc aorta): Timing run 2 (Groin): Injection rate: 1 mL 2 mL 3.5 mL / sec Saline chaser Volume: Injection rate: 30 mL 3.5 mL / sec Chest-Abdomen • KVp 80 • mAs 1500 – 15 mL 5 ml @ 3.5 mL/s 10 ml @ 2.0 mL/s BOLUS TRAIN 6.4 sec • Saline 25 ml @ 2 mL/s 31 Adequate enhancement of the aorta 171 HU 31 Chest-Abdomen • • • KVp 80 mAs 1500 – 15 mL 5 mL @ 3.5 mL/s 10 mL @ 2.0 mL/s BOLUS TRAIN 8.3 sec Saline 25 mL @ 2 mL/s Pelvis CTA 13 mL CM 370 mg/mL 5mL @ 3.5/s 8mL @ 2.0/s 25 mL saline @ 2.0/s 31 Aortic valve measurements 31 Centerline stack images 31 Case 3 - 28 mL (1+2+25) • • • • • 80 KVp mAs 1525 Main scan 25 mL 2 Timing runs (1 + 2 mL) Chest-Abdomen-pelvis scan (cardiac gated) Timing Bolus 18 sec 22 sec 25 mL Scan Length: 42.2 cm Scan Time: 8 sec Injection: 10mL @ 3.5 mL/s 15 mL @ 2mL/s Injection Duration: 10 sec 333 HU Case 4 - 22 mL • KVp 80 mAs 1500 • 1mL each for 2 timing runs • Main scan 20 mL: – 10 mL injected at 3 mL/s (3.3 s) – 10 mL @2 mL/s (5.0 s) • BOLUS TRAIN 8.3 sec • Saline 20 mL @ 2 mL/s. 22 Case 4 - 22 mL Arterial attenuation > 250 HU 22 Noise reduction with Iterative Reconstructions 15 ml thoracic aorta scan Ascending aorta = 280 HU Improved noise reduction with Model Based Iterative Reconstructions Regular IR Moderate Heavy SD = 20 SD = 15 Model Based IR SD = 8 Summary Goal: Achieve adequate arterial enhancement for the preoperative evaluation. Scanner - 80kV technique - Retrospective cardiac gating - IR or MBIR Contrast media technique - Timing run - Saline chaser