Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
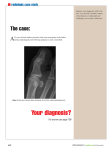
Holly Nieman ATR320 Term Paper 11/17/2014 Sesamoiditis of the Foot Anatomy of the injured area Sesamoid bones can be found in the hand, knee, and foot, and their unique structure works to protect the tendon, and to increase its mechanical effect. They are bones that develop in muscle tendon rather than being attached by ligaments to another bone. Therefore, the unique aspect of sesamoid bones is their free floating or free standing nature. Most people have five sesamoid bones in each hand. Two at the thumb metacarpophalangeal joint, one at the interphalangeal joint of the thumb, one at the metacarpophalangeal joint of the index finger on the radial side, and one at the metacarpophalangeal joint of the little finger on the ulnar side (VE, 1984). The patella is also anatomically a sesamoid bone and also the largest sesamoid in the body. The most commonly irritated sesamoid bones are located in the tendons of the flexor hallucis brevis on the plantar aspect of the foot, which help redistribute and dissipate force over the first metatarsal head during the toe-off portion of gait or propulsion. There are two sesamoid bones beneath the hallux, the tibial (medial) and fibular (lateral). Injuries to these sesamoid bones are usually transverse, however due to the increased weight-bearing role of the medial sesamoid, oftentimes injury to that individual bone will be seen. The sesamoid bones were designed to act as a fulcrum or a lever arm for the flexor tendons which surround them. They also serve as a prevention method against the flattening of the tendon when joint tension increases during certain movement (MedicMD, 2014). This paper will be focused strictly on the tibial and fibular sesamoids. Injury Pathology/Mechanisms of Injury Sesamoiditis is a broad term to categorize different pathologies affecting the sesamoids of the first MTP. Chronic pain at the hallucal sesamoids may clinically be described as “sesamoiditis”, a term that encompasses the symptoms from pathology at the hallux sesamoids complex. Chronic pain can be caused by stress fracture, stress reaction, osteoarthritis and osteonecrosis of the sesamoids, as well as tendinosis and capsular inflammation. Repetitive and excessive axial loading in plantar flexion, such as in ballet dancing, running and even wearing high-heeled shoes, have also been postulated as risk factors for sesamoiditis (O. Kenechi Nwawka, 2013). Pathology of the sesamoids can lead to a substantial loss of function if not treated appropriately. Evaluative Techniques Vital to Recognition Sesamoid pathology is varied and can be difficult to differentiate clinically from other forms of pathology at the level of the first MTP joint, making diagnosis difficult as it presents similarly in stress fracture syndrome or metatarsalgia. As sesamoiditisis a diagnosis of exclusion, other sesamoid pathologies must first be ruled out before the diagnosis can be confirmed. (Atiya S, 2013). Thorough evaluative techniques to rule out other pathology would include patient history of past and present injuries, history of activity, type of symptoms that the patient is experiencing, and type of pain. The clinician should examine several aspects of the individual’s stance and gait, as well as mechanical structure of the hip, leg, and foot. Palpation of the injured area to distinguish any edema or point tenderness as well as active and passive range of motion tests will be critical in making a differential diagnosis. First Aid/Treatment necessary Initial treatment in the acute stage involves ice massage, anti-inflammatory medications or cortisone injections, and rest. Pulsed phonophoresis and iontophoresis are alternative methods of combating the inflammatory response and may be of value in reducing symptoms. Definitive treatment must include relief of weight-bearing stress on the affected area. A custom-molded orthotic device with proximal elevation and a first ray cutout combined with a Morton extension or carbon fiber forefoot plate to reduce forefoot motion and eliminate loading in the dorsiflexed position can provide this relief (Andrews, 2012). Prior to the mid-1980s, excision of the sesamoids was the primary surgical treatment for all sesamoid pathology. Many authors still recommended excision as the primary surgical intervention for sesamoid pathology, including sesamoiditis that is not relieved by orthotic management of at least six months duration (Atiya S, 2013). Opinions are varied in regards to surgical treatment, as is the outcome for patients following surgery. Therefore, less invasive approaches to treating sesamoiditis are most commonly recommended while keeping surgical options reserved as a last resort. To improve long-term function and decrease the chances of reoccurrence of the injury a gel insert, pad, or orthotic to help redistribute weight and decrease motion of the MTP would be advised. In the case of athletes, certain shoe adjustments can be made to help limit the chances of irritation. For example, in football, the cleats and screw post that lay directly beneath the sesamoid can be removed to help with comfort, and in sprinting, it is possible to stiffen the shoe to reduce excessive flexion of the first MTP. Common and Unusual S/S That May Be Found Symptoms and signs arising from the sesamoids of the MTP include pain on direct palpation or on movement of the first MTP joint, restricted range of motion, swelling of the first MTP joint and decreased plantar/dorsiflexion strength. Synovitis of first MTP joint may be noted and sometimes a plantar callosity may be present under the sesamoids (R. Anwara, 2005). The onset is usually gradual and the pain may begin as a mild ache and will further increase to a more intense throbbing that will limit weight bearing if aggravation continues. There will usually be some swelling that will limit range of motion. Erythema and ecchymosis are rare in most cases of sesamoiditis. Predisposing factors Athletes most prone to medial sesamoid pathology are those with a rigid pes cavus, forefoot equinus, tight Achilles tendon, and plantar-flexed first ray. Sesamoid pain also occurs in athletes with normal foot structure but whose activities require repetitive maximal dorsiflexion of the first MTP joint, which results in excessive impact loading stress on the sesamoids (Andrews, 2012). Other predisposing factors could include hyperpronation, metatarsus varus, and hallux valgus. Diagnostic Tools A thorough history and physical examination would be highly valuable in early diagnosis of sesamoiditis. Additional diagnostic tools such as bone scan, computed tomography (CT), and magnetic imaging (MRI) may be useful to further evaluate the sesamoid complex (Douglas N. Beaman, 1999). A bone scan is a test that can find damage to bones and is used to diagnose the cause or location of unexplained bone pain. Computed tomography, also referred to as an x-ray, takes cross-sectional pictures of an area to be used in a variety of diagnostic or therapeutic purposes. Most commonly used in evaluation of a suspected sesamoid injury would be the MRI which uses a powerful magnetic field, radio frequency pulses and a computer to produce detailed pictures of organs, soft tissues, bone and virtually all other internal body structures. An important factor of the MRI is that it does not use ionizing radiation. Early and accurate diagnosis of sesamoid complex disorders can guide the clinician to the appropriate clinical management and prevent potentially harmful longstanding joint dysfunction. Prognosis and Outcome In most cases sesamoiditis has a good outcome if cared for properly. As mentioned in the Treatment section, padding or taping, immobilization or activity modification, physical therapy, steroid injections, and orthotic devices are all excellent options for the treatment of sesamoiditis. Education for the individual suffering with the inflammation will be important for their future activities=0 education on recognizing early signs and education on care will be very effective in lessening the frequency of the over-use. Therefore, a positive outcome is usually expected. Unfortunately there are the few individuals that struggle with the sesamoiditis resolving after the previously mentioned care. To again refer to the Treatments section, surgery is reserved as a last resort and outcomes do vary. In most cases surgical excision will produce significant relief of pain and improved functional outcome. However, there are some instances post-operative patients struggle with incomplete relief of pain, restricted range of motion, plantar-flexion weakness, or a mild drift of the hallux (Morsi, 2007). Figure 1. A depiction of the medial and lateral sesamoid bones in relation to the flexor hallucis brevis muscle and tendons. Figure 2. A before and after x-ray of a sesamoidectomy. Figure 3. A suggested method of padding to reduce pain and pressure on an inflamed sesamoid. References Andrews, J. (2012). PHYSICAL REHABILITATION OF THE INJURED ATHLETE. Rittenhouse Book Distributors, Inc. Atiya S, Q. C. (2013). Sesamoiditis of the metatarsophalangeal joint. OA Orthapaedics. Douglas N. Beaman, L. J. (1999). Hallucal sesamoid injury. Operative Techniques in Sports Medicine, 7-13. MedicMD. (2014, March 12). Retrieved from http://sesamoiditis.net/: http://sesamoiditis.net/ Morsi, E. (2007). Tibial sesamoidectomy of the great toe in heavy manual workers. The Foot, 21-24. O. Kenechi Nwawka, D. H. (2013). Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology. U.S. National Institutes of Health's National Library of Medicine, 581-593. R. Anwara, S. A. (2005). Sesamoids of the Foot. Current Orthopaedics, 40-48. VE, W. (1984, October 9). PubMed. Retrieved from The Sesamoid Bones of the Hand and their Pathology: http://www.ncbi.nlm.nih.gov/pubmed/6512360