Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
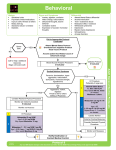
Patient Monitoring and Documentation Interaction Level 1: patient should be able to communicate presence of pain or anxiety. This should correspond approximately to a VICS interaction score of at or above 24/30. If the patient is agitated but is unable to communicate presence of pain or anxiety call MD to assess patient for delirium. Documentation: 1) VICS q4h on ALL patients 2) VICS pre and post intervention to treat pain, agitation/delirium or anxiety 3) Pain Intensity with Numeric Rating Scale (0-10) pre and post intervention to relieve pain 4) In patients who cannot communicate presence of pain, document clearly in the SAD record perceived signs of pain that trigger intervention. Analgesia Administer 5 MIN prior to procedures that may cause pain (to allow time for drug to act; 80% of peak effect is reached in approx 5 MIN) To relieve pain in patients who communicate need for intervention To treat signs of pain in patients who cannot communicate but pain is suspected given clinical situation. Review signs of inferred pain with MD q4h. Bolus morphine 0.5 mg, 1 mg, 2mg, 4mg, 6mg Q 5 MIN prn until effect or adverse event seen (e.g. hypotension) Assessment: 1) Assess patient’s response 5 MIN following each dose. Goal is to reduce patient’s pain intensity rating to 3/10 (NOT 0 / 10) or as patient directs 2) If administering analgesia to patients who cannot communicate presence of pain but pain is suspected given clinical situation Review with MD signs of perceived pain that trigger intervention Q4H or earlier if signs are not corrected. Call MD if infusion considered necessary after 6 hrs of bolus therapy At this time discuss with MD role of: 1) Non-narcotic analgesia: Tylenol or NSAID 2) Whether epidural analgesia is appropriate Peri-procedural sedation Explain procedure to patient as fully as possible Administer 3 MIN prior to procedure Find minimal effective dose Bolus midazolam 0.5 mg, 1mg, 2mg, 4 mg, 6 mg IV Q 3 MIN prn Anxiety Patient must be able to confirm that they are anxious Enquire into source of anxiety and provide reassurance Lorazepam 0.5 mg to 1mg SL/IV Q4H PRN x 24h Delirium Delirium is characterized by: Inattention & fluctuating interaction WITH EITHER disorientation OR agitation OR withdrawn; hallucinations may be present Physician should rule out agitation due to: withdrawal from alcohol, sedatives, analgesics or nicotine; or other reversible causes (e.g. suboptimal ventilator settings or metabolic disturbances). For delirium that is not associated with alcohol or other withdrawal states: Discontinue opioids and benzodiazepines if possible Reassure and re-orientate patient to environment (ensure access to eyeglasses/ hearing aids if applicable) Use the pre-printed orders “ICU orders for delirium” Physician to order either: Haloperidol 2.5 mg to 10 mg IV Q 20 to 30 MIN prn Dose may also be on a fixed schedule e.g. 1 mg to 5 mg IV/NG bid. If it is ordered on a prn schedule a maximum dose should be specified over a 12 hr interval e.g. 40 mg. If maximum dose is reached medical team needs to review and justify continuation OR Methotrimeprazine 5 mg to 25 mg IV Q 20 to 30 MIN prn If ineffective (dosing level 5 reached) or symptoms worsening call MD to reassess reassess with MD if patient received 150 mg in a 12 hr interval ESCALATING REGIMEN FOR HALOPERIDOL AND METHOTRIMEPRAZINE (NOZINAN) Dosing level 1 to 3 can be given 20 mins apart if needed . Dosing Level Haloperidol IV Q 30 MIN (mg) Methotrimeprazine (Nozinan ) IV Q 30 MIN (mg) 1 2.5 5 2 5 12.5 3 5 12.5 4 10 25 5 10 25 If at any time agitation is dangerous to patient or caregiver call MD for a midazolam bolus order ADVERSE EVENT MONITORING 1) Measure QT and RR interval from rhythm strip before first dose of haloperidol 2) Use Table 1 to determine QTc. 3) Measure QT and RR interval from rhythm strip before each dose successive of haloperidol. 4) Discontinue haloperidol if QTc increases by 25% from baseline. 5) Observe and assess patients for any signs of stiffness or parkinsonian-like effect or hypotension ( with methotrimeprazine ). MAINTENANCE REGIMEN For escalating haloperidol or methotrimeprazine regimen, the following applies: If a patient’s target symptoms are corrected call MD to write a maintenance regimen. Add up first 24-hour dose requirement. Give 50% of this dose over the next 24 hours in 4 divided doses i.e. Q6H Reduce maintenance dose by 25% each day if patient’s symptoms remain controlled. Continue prn regimen as needed for breakthrough agitation that is presumed due to delirium . Sedation for physiologic goals Monitoring Document VICS score q4h Infusion rates must be reassessed q 6h and adjusted accordingly; reduce by 25% if clinical goals are met Medical team must perform daily review and justify continued need for sedation goals Sedation goals 1) O2 demand during shock state 2) prevent patient movement 3) other as specified on order OR OR Midazolam 1 mg, 2 mg, 4mg, 6mg IV Q3 MIN prn Refer to table on infusion titration to determine if an infusion should be started To suppress respiratory drive (that is associated with O2 sat) Morphine 1 mg, 2mg, 4mg, 6mg Q 3 MIN prn With Midazolam 1 mg, 2 mg, 4mg, 6mg IV Q3 MIN prn If ineffective or if BP falls call MD If effective refer to table on infusion titration to determine if an infusion should be started Sedation and analgesia in patients with elevated ICP 1. Ensure that Head Injury Protocol has been instituted. 2. Start morphine and midazolam infusions at rate ordered. ICP IS ELEVATED (>20mmHg) IS IT RELATED TO NOXIOUS STIMULI? a)YES b)NO 1) Remove stimulus 2) Pre-medicate patient with midazolam prior to future planned non-painful stimuli (use morphine if painful) 3) If ordered and ICP remains elevated despite removal of stimulus follow guidelines for procedural boluses of midazolam to treat this episode of ICP elevation 4) If ICP >20 for > 5 MIN 1. Open drain and leave open x 5 minutes. 2. Review head injury protocol >20 for < 5 MIN 5) Do not increase infusion rates based on procedural boluses. NO ACTION c) NO >20 for > 5 MIN 1) Open drain and leave open x 5 minutes. 2) Call MD to determine management 3) Review head injury protocol Sedation and analgesia prior to initiation of neuromuscular blockade Titrate analgesia to achieve pain relief prior to starting neuromuscular blockade. Ensure patient is deeply sedated so that they are unarousable, with in addition, no physiologic (HR/BP) response to stimuli. Midazolam bolus 1, 2mg, 4mg, 6 mg IV Q 3 MIN to achieve unarousable state and no response to physiologic stimuli then start midazolam infusion 5 to 10 mg/hr as needed (refer to table on infusion titration). Maintenance protocol for titration of morphine and midazolam infusions TO DETERMINE INITIAL RATE OF MORPHINE OR MIDAZOLAM INFUSIONS AND SUBSEQUENT RATE INCREASES: TO START FIRST 6 HOURS: Total amount of drug patient responded to (not including procedural boluses): <6mg 6-12mg 13-18mg 19-30mg >30mg Initial rate - mg/hr No infusion No infusion 1 2 3 SUBSEQUENT ADJUSTMENT Total bolus doses given in last 6 hours (not including procedural boluses) <6mg 6-12mg 13-18mg 19-25mg >25mg For physiologic goals, may start an infusion (if ordered) within 6 hours 1) 2) 3) 4) Titrate to minimal effective dose Infusion rates must be reassessed q 6h Reduce by 25% if clinical goals are met. If infusion rate is 1mg/h discontinue infusion and use bolus prn. Rate increase – mg/hr 0 1 2 3 4 Vancouver General Hospital ICU Protocols for sedation, analgesia and delirium Last revision date: May 2006