Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
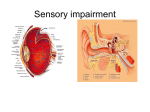
Visual impairment wikipedia , lookup
Corrective lens wikipedia , lookup
Vision therapy wikipedia , lookup
Keratoconus wikipedia , lookup
Corneal transplantation wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
Contact lens wikipedia , lookup
Dry eye syndrome wikipedia , lookup
9565 Weston Road #100 Vaughan, ON L4H 3A5 T: 905 303 9775 F: 905 303 9791 E: [email protected] PATIENT HISTORY FORM Name: _______________________________________________________ Birth date (month/day/year): ______ / ______ / ______ Address: ________________________________________City: ___________________________ Postal Code: __________________ ❑ Business # Home phone # ________________ ❑ Cell phone # ________________ E-‐mail: ___________________________________ How would you like to be contacted? ❑ E-mail ❑ Phone ❑ Text Message Occupation: ________________________ Who referred you to us?: __________________ Date of last eye exam: ____________ Family Doctor: ___________________________ Are you required to wear glasses or contacts to drive? ❑Yes ❑No ❑No license Are you allergic to any medications, eye drops, or contact lens solutions? ❑No ❑Yes, list:_____________________________________ YOUR MEDICAL HISTORY ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N Environment allergy Arthritis Autoimmune Disease Diabetes High blood pressure Heart disease High cholesterol Thyroid Eye injury Eye surgery Cataracts Glaucoma Other Please Specify ___________________ FAMILY MEDICAL / OCULAR HISTORY ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N Blindness Cataracts Diabetes Glaucoma High Blood Pressure Heart Disease Macular degeneration Other Please Specify ___________________ Are you interested in laser eye surgery? ❑Yes ❑No DO YOU EXPERIENCE: ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N ❑Y ❑N Blurry distance vision Blurry intermediate/computer vision Blurry close vision Double vision Sudden vision loss Flashes of light Floating spots Watery eyes Burning eyes Dry eyes Red eyes Frequent headaches Uncomfortable contact lenses Other: Please Specify _______________ FOR CONTACT LENS WEARERS: Is there ever a time that you wish you didn’t have to wear your glasses? ❑Y ❑N Do you currently wear contact lenses? ❑Y ❑N If yes? When?___________________________________ Hours per day? ___________________ How often do you throw them out? __________________ At what point do your contact lenses feel dry? _______________________________________ How often? ❑ 5-7 days per week ❑ 1-4 days per week ❑ < 1 day per week Hours worn per day? _________________ What kind? ❑ soft disposable ❑ soft non-disposable ❑ rigid gas-permeable ❑ hybrid lens ❑ scleral lens EYE HEALTH ❑Y ❑N Amblyopia (Lazy eye) ❑Y ❑N Burning Eyes ❑Y ❑N Cataracts ❑Y ❑N Corneal Transplant ❑Y ❑N Double / Distorted Vision ❑Y ❑N Drooping Eyelid ❑Y ❑N Eye Surgery ❑Y ❑N Eye Turn ❑Y ❑N Floaters / Spots ❑Y ❑N Fluctuating Vision ❑Y ❑N Glaucoma ❑Y ❑N Glare / Light Sensitivity ❑Y ❑N Headaches ❑Y ❑N Itchy Feeling ❑Y ❑N Keratoconus ❑Y ❑N Loss of Vision ❑Y ❑N Mucus Discharge ❑Y ❑N Redness ❑Y ❑N Tearing ❑Y ❑N Other Please Specify ____________________ MEDICATIONS List all the medications taken by the patient and note that condition it is for Medication Condition Medication Condition Please list all the names of the medications the patient is allergic to: __________________________________________________________________________________________________ __________________________________________________________________________________________________ __________________________________________________________________________________________________ Emergency Contact _____________________________________________ Phone Number:______________________ Relationship to Patient: ______________________________________ Alternate Number:________________________