Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
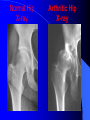
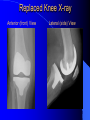
Hip and Knee Osteoarthritis dr n. med. Dariusz Mątewski Joint degeneration changes are the most frequent reason of joint diseases and affect @ 15% of human population It is characterized by: – Progression lesion initially mainly affected cartilage then another subchondral layers in final stage also bone tissue – Besides decayed changes quickly develop hypertrophic ones: formation of new bone tissue on borders of the joint (osteophytes) sclerosis of subchondral bone layer – Degenerative joint disease is also described as a disturbance of balance between cartilage degradation process and synthesis cartilage proces Normal cartilage structure Normal cartilage structure Initial degenerative joint changes Degenerative joint changes – cont. Advanced degenerative joint changes Most Common Types of Arthritis – Primary Osteoarthritis – Secondary Osteoarthritis – – – – – Dysplastic Arthritis Rheumatoid Arthritis Post-traumatic Arthritis Avascular Necrosis Others OA Symptoms – May develop suddenly or very slowly – Arthritis can cause pain and stiffness – Some types of arthritis may cause swelling – Growing deformity of joint – Joint disfunction with limitation of motion – Simple activities may be difficult to do Characteristics of primary degenerative joint disease – The most frequently occur in patients between 45- 60 years of life. – Frequently in women than men – Disease is characterized by: quite insidious, slow growing of symptoms which are accompanying by: – pain – joint deformity – joint disfunction disease is characterized intially by: – – – – local changes then can affect neibourgh joints, equal-nominal joints whole locomotor system Secondary Osteoarthritis Dysplastic Arthritis abnormal joint shape can lead to large wear Rheumatoid Arthritis inflamed joint tissue leading to cartilage lesion Post-traumatic Arthritis irregularities of cartilage joint surface lead to large wear Avascular Necrosis bone may collapse and damage cartilage The most frequent localization of osteoarthritis: Spine osteoarthritis ( intervertebral joints and deformative and degenerative changes of vertebra’s corpuses with intervertebral discopathy) Hip osteoarthritis Knee osteoarthritis – (femoralopatelar compartment, femoralotibial compartment) foot osteoarthitis – MTP I joint – ankle joint – subtalar joint shoulder osteoarthritis elbow osteoarthritis hand joints osteoarthritis The most frequent localization of osteoarthritis: Degenerative changes of IP joints in hand – Heberden tubercule Degenerative changes of cervical spine Degenerative changes of lumbar spine Hip osteoathritis Knee osteoarthritis Clinical examination we exam: – joint contour – joint movement – joint conracture – joint stability, – limb axis, – gait abnormalities (limping, walking distance), – posture abnormalities, – changing in way of doing some daily activities, The Orthopaedic Examination The physical examination enables surgeon to evaluate important aspects of joints, including: – Size and length – Strength – Range of motion – Swelling – Reflexes – Skin condition Typical posture indicates on limitation of flexion and rotation movement in hip joint Localization of pain in patient with hip osteoarthritis Knee position is frequently in flexion contacture with varisation of lower limb axis Obciążenie współistniejące Należy pamiętać, że choroba zwyrodnieniowa dotyczy głównie ludzi w wieku starszym, którzy dość często cierpią z powodu innych schorzeń: – – – – – choroba wieńcowa, nadciśnienie tętnicze, cukrzyca, choroby układu żylnego kończyn, przewlekłe choroby układu oddechowego i inne Leczenie choroby zwyrodnieniowej w wieku podeszłym jest utrudnione i ograniczone z uwagi na ogólną wydolność chorego. The Orthopaedic Evaluation X-ray Evaluation An abnormal X-ray may reveal: – Narrowing of the joint space – Cysts in the bone – Spurs on the edge of the bone – Areas of bony thickening called sclerosis – Deformity or incorrect alignment Normal Knee X-ray Arthritic Knee X-ray Normal Hip X-ray Arthritic Hip X-ray The Orthopaedic Evaluation Additional Diagnostic Tests may include: – – – – – Blood tests Urine analysis Analysis of joint fluid Magnetic Resonance Imaging (MRI) Bone scan Treatment Options – Medications – Physical therapy – Bracing – Injections (steroid or joint fluid supplements) – Arthroscopy – cleaning the joint – Partial joint replacement – Total joint replacement Medications – Aspirin-free pain relievers–acetaminophen – Nonsteroidal anti-inflammatories (NSAIDs) – Glucosamine / chondroitin sulfate – Corticosteroids–injection/pill form Quick, effective pain relief Max 3-4 times per year – Viscosupplementation = Joint Fluid Replacement Bracing and Assistive Devices A cane in the opposite hand decreases joint forces by 50% ! “Unloader” braces can take pressure off the painful side of the knee and stabilize the joint Physical Therapy Passive range-of-motion exercises may help: – Reduce stiffness – Keep joints flexible 4-5 times bodyweight through knee climbing stairs! Quadriceps strengthening Transition from high to low-impact exercises – Cycling, elliptical, swimming – Avoid deep knee bends against resistance What is Arthroscopy? Arthroscopy is a surgical procedure used to visualize, diagnose and treat problems inside a joint. • A small incision is made in the patient's skin and then pencil-sized instruments are inserted that contain a small lens and lighting system to magnify and illuminate the structures inside the joint. Partial Joint Replacement Surgical procedure in which only the damaged or diseased surfaces of the joint are replaced, leaving much of the natural bone and soft tissue in place. – Post-operative pain may be reduced – Recovery period may be shorter than total knee replacement Total Joint Replacement Surgical procedure in which certain parts of an arthritic or damaged joint are removed and replaced with an artificial joint. The artificial joint is designed to move just like a healthy joint. Joint Replacement Joint replacement is a treatment option when pain: – Is severe – Interferes with daily activities – Interferes with work Joint Surgery May be suitable for patients who: – Have a painful, disabling joint disease of the joint resulting from a severe form of arthritis – Are not likely to achieve satisfactory results from less invasive procedures, medication, physical therapy, or joint fluid supplements – Have bone stock that is of poor quality or inadequate or other reconstructive techniques Total Joint Replacement Goals of total joint replacement are to help: Relieve pain Restore motion and function Hip Joint The hip must bear the full force of body weight and consists of two main parts: – A ball (femoral head) at the top of your thigh bone (femur) – A rounded socket (acetabulum) in your pelvis How’s this for an endorsement? “The Operation of the Century: Total Hip Replacement” The Lancet, October 2007 Total Hip Replacement Replaced Hip X-ray Knee Joint Femur – thigh bone Cartilage – tissue between bones that provides cushioning Patella – knee cap Tibia – shin bone Synovium – tissue surrounding the joint that provides lubricating fluid Ligament – flexible tissue that holds knee joint together Total Knee Replacement – End surface of femur replaced with metal – End surface of tibia replaced with metal – Plastic liner is inserted between femur and tibia – Patella is resurfaced with plastic Replaced Knee X-ray Anterior (front) View Lateral (side) View Knee Replacement: Total versus Unicompartmental Majority of patients predominantly affected in one compartment only Relatively easier recovery Less surgery Maintain cruciate ligaments – “feels more natural” Does not preclude TKA later – Most do not need to be converted Computer Navigation No benefit in skilled hands for the average patient May help surgeon who do less joint replacements, but need to know when not to trust it… Definitely helpful in outliers: – Significant deformity or malalignment – Old hardware Total knee replacement is primarily a Soft Tissue Procedure. Recovery Recovery Every individual is different and every treatment plan is different. “You’ll be mad at me for two weeks” Estimated Recovery Schedule: – In-hospital: 2 – 5 days – Significant Functional Improvement: 2 wks – 3 mos – Maximal Improvement: 6 – 12 months Recovery Directed exercise program The physical therapist or another member of the staff works with you to help you: – Regain muscle strength – Increase range of motion Start with home PT and progress to outpatient therapy General Guidelines to get back to your Routine – You'll practice stair-climbing in the hospital and should be able to do this by the time you leave – You should have no restrictions on leaving your home as long as your safety and comfort are assured. A good balance of exercise, rest, and relaxation is best for helping your body heal and gain strength – When to resume driving a car, going to work, and/or participating in sports activities are all highly individualized decisions. Limitations After Surgery Athletic activities that place excessive stress on the joint replacement should be avoided. Examples include: – Difficult Skiing (snow or water) – Contact sports – Regular running – Frequent jumping Patients don’t listen to me…