Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
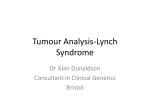
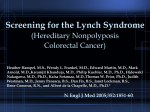
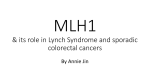
Reviews Clinical Chemistry 60:1 111–121 (2014) Lynch Syndrome Presenting as Endometrial Cancer Laura J. Tafe,1 Eleanor R. Riggs,2 and Gregory J. Tsongalis1* BACKGROUND: Lynch syndrome (LS) is the most common form of the hereditary colon cancer syndromes. Because of its high prevalence, a nationwide campaign has begun to screen all colorectal cancers for the genetic abnormalities associated with LS. CONTENT: Next to colorectal cancer, endometrial cancer is the most common form of malignancy found in women with LS. Identifying individuals who harbor the well-characterized mismatch-repair gene mutations via immunohistochemistry, microsatellite instability analysis, or direct gene sequencing is critical to managing the LS patient and to surveillance for the development of other associated tumor types. SUMMARY: Although many institutions have begun screening all colorectal tumors for LS, the evidence is sufficient to warrant the testing of all endometrial cancers for LS as well. Various testing algorithms, along with genetic-counseling efforts, can lead to a costefficient and beneficial screening program. © 2013 American Association for Clinical Chemistry In 2013, more than 1.6 million new cases of cancer will be diagnosed in the US, and more than 500 000 individuals will succumb to their disease (1 ). Colorectal cancer (CRC)3 and endometrial cancer (EC) represent 100 000 and 50 000 new cases, respectively, with corresponding 50 000 and 8000 cancer-related deaths (1 ). CRC is the second leading cause of cancer-related mortality in the US (2 ). Up to 30% of CRCs are recognized as having a familial component that can manifest as one of the well-characterized hereditary colon cancer susceptibility syndromes. One of these diseases, Lynch 1 Departments of Pathology and 2 Medicine, Geisel School of Medicine at Dartmouth, Hanover, NH, and Dartmouth-Hitchcock Medical Center and Norris Cotton Cancer Center, Lebanon, NH. * Address correspondence to this author at: Geisel School of Medicine at Dartmouth and Dartmouth-Hitchcock Medical Center, One Medical Center Dr., Lebanon, NH 03756. Fax 603-650-6120; e-mail gregory.j.tsongalis@ hitchcock.org. Received June 26, 2013; accepted October 17, 2013. Previously published online at DOI: 10.1373/clinchem.2013.206888 3 Nonstandard abbreviations: CRC, colorectal cancer; EC, endometrial cancer; LS, Lynch syndrome; MMR, mismatch repair; MSI, microsatellite instability; MSI-H, high MSI; FIGO, Fédération Internationale de Gynécologie et d’Obstétrique (score); IHC, immunohistochemistry; NCCN, National Comprehensive Cancer Network; PGM™, Ion Torrent Personal Genome Machine. syndrome (LS), accounts for 3%–5% of all CRCs (2– 4 ) and 2%–3% of ECs (5, 6 ). LS, also known as hereditary nonpolyposis colorectal cancer, was originally described by Warthin in 1913 in a kindred showing predisposition to cancers of the colon, stomach, and endometrium (7 ). In 1966, Lynch described similar findings for 2 large kindreds (8 ). LS is an autosomal dominant disorder caused by germ line–inactivating mutations in one of the 4 DNA mismatch-repair (MMR) genes: MLH14 (mutL homolog 1), MSH2 (mutS homolog 2), MSH6 (mutS homolog 6), and PMS2 [postmeiotic segregation increased 2 (S. cerevisiae)] (9, 10 ). Deletion of the 3⬘ end of the EPCAM (epithelial cell adhesion molecule) gene, which resides upstream of MSH2, is also thought to cause LS, through epigenetic silencing of MSH2 (3, 4 ). Lack of or faulty MMR mechanisms can lead to increasing microsatellite instability (MSI) due to errorprone DNA replication. CRC is the most common form of cancer seen in LS patients, and the high prevalence has prompted universal screening of all CRCs for LS (10 ). LS is also characterized by extracolonic cancers, of which cancers of the endometrium and ovary are the most common (3, 10 ). Women with LS have a 40%– 60% chance of developing EC as their first malignancy and have a greater overall lifetime risk of developing EC than CRC (9 –11 ). The incidence of LS in unselected populations of EC patients is 2%–3%; however, that is possibly an underestimate, because some populations may have different mutation frequencies and because the clinical importance of some mutations remains uncertain (5 ). The frequency of mutations in MMR genes for EC is 50%– 66% in MSH2, 24%– 40% in MLH1, 10%–13% in MSH6, and ⬍5% in PMS2 (10 ). This high prevalence, along with the implementation of universal screening of CRCs for LS, has heightened awareness of the consequences of identifying EC as an LS-related cancer. We review the pathologic features, screening approaches, and genetic-counseling aspects of LSrelated EC. 4 Human genes: MLH1, mutL homolog 1; MSH2, mutS homolog 2; MSH6, mutS homolog 6; PMS2, postmeiotic segregation increased 2 (S. cerevisiae); EPCAM, epithelial cell adhesion molecule; BRAF (v-raf murine sarcoma viral oncogene homolog B; PMS2CL, PMS2 C-terminal like pseudogene. 111 Reviews Histopathology of EC in LS CRC in LS patients is well recognized to be associated with several histopathologic features, including an origin in the right colon, a poorly differentiated or medullary histology with mucinous or signet ring cells, abundant tumor-infiltrating lymphocytes, and peritumoral lymphoid follicles—the so-called Crohn-like lymphocytic reaction (12 ). Screening algorithms based on histologic observations (which are susceptible to intraobserver variability) and family/clinical history alone are not sufficient, however, to identify patients who should undergo further testing for LS. For this reason, several organizations have recently proposed recommendations for universal screening of CRC patients (13–16 ). In a 2005 series of 117 women with LS and a personal history of CRC and either EC or ovarian cancer, 14% had synchronous cancers at diagnosis. Of the remaining patients, 51% were diagnosed first with a gynecologic malignancy (17 ). The histopathologic features of EC associated with LS are less well characterized than for CRC. In 2006, Broaddus et al. published their investigation of the pathologic features of ECs (18 ). They compared 50 women with LS (all had confirmed mutations in either MLH1 or MSH2) with 2 groups of patients with sporadic disease (confirmed negative MLH1 and MSH2 mutations): (a) women ⬍50 years of age (42 patients) and (b) women of all ages with MSI-high (MSI-H) tumors secondary to MLH1 methylation (26 patients). Ninety-four percent of the patients were carriers of MSH2 mutations. The mean age at diagnosis for LS patients was 46.8 years, vs. 39.9 years for the group ⬍50 years of age and 61.1 years for the MLH1-methylation group. The majority of tumors had an endometrioid histology, either pure or mixed, and 14% of the LS patients had nonendometrioid tumors (3 patients with clear cell carcinoma, 3 with uterine papillary serous carcinomas with a clear cell component, and 1 with malignant mixed Müllerian tumor), all of which had MSH2 mutations. Nonendometrioid tumors were very rare in the 2 sporadic groups (2.4% and 3.8%, respectively). Compared with the other 2 groups, the MLH1methylated group was associated with a higher-grade endometrioid tumor with lymphovascular invasion, and 19% had the distinctive undifferentiated histology. The 3 groups were not significantly different with respect to pathologic stage, but there was a trend toward a more advanced stage (stage III or IV) in the groups with sporadic disease, compared with the LS group (18 ). One shortcoming of this study is that it did not examine for pathogenic DNA alterations in the PMS2 and MSH6 genes; carriers of mutations in these 2 genes might have fallen into their ⬍50-years-old category. 112 Clinical Chemistry 60:1 (2014) Women with LS also have a 10%–12% lifetime risk of developing ovarian cancer, and recent studies have shown that endometriosis-associated ovarian cancers (clear cell, endometrioid, undifferentiated, or mixed) are more frequently associated with MMR abnormalities or are MSI-H, compared with high-grade serous carcinomas and other histologic subtypes. Mutational status was not confirmed in these patients, however (17, 19 –21 ). Several studies have attempted to characterize the EC morphology suggestive of MMR deficiency or the MSI-H phenotype. The host inflammatory response seems to be the most important feature. The response includes (a) peritumoral lymphocytes, defined as lymphocytic aggregates apparent at a scanning magnification, and (b) the presence of tumorinfiltrating lymphocytes, defined as lymphocytes within tumor cell nests or glands (a score of ⱖ40 lymphocytes per 10 high-power fields indicates a positive finding). An additional feature is tumor heterogeneity, defined as 2 morphologically distinct populations of tumor cells that constitute ⱖ10% of the tumor and are juxtaposed but not admixed with one another. A tumor with this feature is often dedifferentiated EC, which comprises FIGO (Fédération Internationale de Gynécologie et d’Obstétrique) grade 1 or 2 endometrioid carcinomas and undifferentiated carcinomas (19, 22 ). The undifferentiated histology is characterized by round or polygonal cells with vesicular nuclei that grow in solid, discohesive sheets without a pattern or gland formation. A variably myxoid matrix and rhabdoid-like cells have also been described. Most undifferentiated carcinomas show focal but strong staining for cytokeratins or epithelial membrane antigen, with cytokeratin 18 being the most frequently produced keratin. In contrast to better-differentiated components, the undifferentiated component is usually histologically negative for estrogen receptor and progesterone receptor (23 ). This histology is associated with a particularly aggressive clinical course (23, 24 ). In their study of MMR proteins produced in EC, Garg et al. found that 7 of 8 dedifferentiated ECs occurred in the group with abnormal immunohistochemistry (IHC) characteristics. Of these 7 patients, 5 had associated MLH1/PMS2 abnormalities, and the other 2 patients had loss of MSH2 and MSH6 (19 ). The genotypic and MLH1-methylation data available for these patients is limited; however, incorporating the features discussed above into a screening algorithm might better define a target EC population for screening (25 ). A recent report by Ryan et al. described a study of 76 women with mutation-confirmed LS and EC. Fifty (66%) of these patients had MSH2 mutations: 18 (24%) had MLH1 mutations, and 8 (10%) had MSH6 mutations. The original histology results for 38 EC pa- Reviews Lynch Syndrome and Endometrial Cancer tients were available for review. These investigators identified a correlation between the anatomic origin of the cancer and individuals with LS: Up to 29% of patients with ECs centered in the lower uterine segment had LS (26 ). In another study, the actual incidence of involvement of the lower uterine segment in LS patients was 5.3% (27 ). The study of Ryan et al. found that 76% of the tumors were low-grade (grade 1 or 2) endometrioid carcinomas. The remaining tumors were of high grade (2 dedifferentiated carcinomas, 2 serous carcinomas, 1 clear cell carcinoma, and 4 mixed/other carcinomas, including malignant mixed Müllerian tumor). The morphologic review also focused on evaluating 4 features associated with MSI-H, including lower uterine segment involvement, tumor heterogeneity (dedifferentiation), peritumoral lymphocytes, and ⬎40 tumor-infiltrating lymphocytes per 10 highpower fields. Only 42% of tumors had ⱖ1 of these features without any significant difference in genotype, suggesting that although these features may be helpful for identifying patients with MSI-H, they are not specific for LS (26 ). Screening for LS in EC National guidelines have been created for both IHC and MSI testing of CRC tumors to screen for potential cases of LS (28 ). The main rationale for screening is the opportunity for timely initiation of risk-appropriate screening and prevention interventions for at-risk patients and their families. Historically, the revised Bethesda criteria have been the most frequently used guidelines, with the major indication for tumor testing being CRC diagnosis before 50 years of age. The National Comprehensive Cancer Network (NCCN) guidelines also support the use of IHC and MSI testing for LS in individuals who have CRC diagnosed before 50 years of age (29 ). Although MSI is characteristic of LS, it can also occur in up to 15% of sporadic CRCs. The reported diagnostic sensitivity of MSI is 89% for defective MLH1/MSH2 genes and 77% for MSH6 (28 ). The NCCN practice guidelines recommend screening for LS in EC patients ⱕ50 years of age, but because of the high prevalence of EC in patients with LS, including those older than 50 years, many institutions have adopted the practice of screening all ECs for the genetic abnormalities associated with LS (5, 30 ). More than 90% of LS-associated EC patients show MSI. IHC SCREENING FOR LS IN EC The MMR proteins form heterodimers as part of the base-excision repair complex, with MLH1 pairing with PMS2 and MSH2 pairing with MSH6. Therefore, loss of MLH1 expression is almost always coupled with loss Table 1. Genetic defect in one of the 4 MMR genes and the corresponding IHC staining patterns expected.a Gene with defect IHC staining pattern MLH1 MLH1 ⫺/⫹,b PMS2 ⫺ PMS2 MLH1 ⫹/⫺, PMS2 ⫺ MSH2 MSH2 ⫺, MSH6 ⫺ MSH6 MSH2 ⫹, MSH6 ⫺ a Germ line mutation— or, in the case of MLH1, gene silencing by somatic promoter hypermethylation in addition to germ line mutation—leads to loss of the protein. b Occasionally, interpretation of IHC analysis can be problematic; abnormal methylation or some MLH1 mutations may produce false-normal MLH1 IHC staining [Umar et al. (28 )]. of PMS2, and loss of MSH2 expression is accompanied by MSH6 loss (Table 1) (31 ). For the IHC studies, complete loss of expression of these genes in the setting of a positive internal control (often stromal cells, lymphocytes, or nonneoplastic endometrium) is interpreted as a positive result (Fig. 1). IHC analysis for MMR proteins is a convenient test and is a diagnostically sensitive and specific method for detecting MSI. Modica et al. showed that testing with a panel of 4 antibodies (to MLH1, MSH2, MSH6, and PMS2) has a 91% diagnostic sensitivity and an 83% specificity for detecting MSI-H (32 ). In addition, the staining pattern is very useful, because it can guide subsequent genetic testing for specific MMR gene sequencing or MHL1methylation studies. MSI SCREENING FOR LS IN EC MMR is one of the postreplication DNA-repair systems that correct errors made by the polymerase during DNA replication (33 ). Base– base mismatches and insertion/deletion loops created by polymerase slippage within sequence repeats (microsatellites) are repaired by this MMR system. Lack of proper MMR function leads to the accumulation of mutations and genomic instability that can manifest as MSI. MSI refers to the altered length of somatic oligonucleotide repeat sequences (short tandem repeats of up to 6 bp) within the genome. MSI can be useful as a surrogate marker for defective MMR when the presence of MSI in the tumor suggests an MMR defect. MSI is detected as either increases or decreases in the number of repeats in these short tandem repeat sequences (29 ). The standard method for detecting MSI is to use the PCR and fluorescently labeled primers to amplify microsatellite repeat sequences in samples of tumor and normal tissues from the same patient. After the PCR, fragment size is typically analyzed with capillary Clinical Chemistry 60:1 (2014) 113 Reviews A B C D Fig. 1. Immunohistochemistry of the 4 MMR proteins: MLH1, MSH2, MSH6, and PMS2. This tumor displays loss of nuclear staining of MSH6 (A), whereas staining is retained for MSH2 (B), MLH1 (C), and PMS2 (D) (magnification, ⫻20). electrophoresis to identify repeat-sequence PCR products of different sizes from tumor tissue, which is accomplished by comparing the results with those for normal tissue. The detection in tumor tissue of fragments of additional sizes, which are more often smaller than the unmutated alleles, suggests defective MMR (Fig. 2) (28 ). A panel of 5 microsatellite markers had originally been recommended in 1997 by a National Cancer Institute workshop and was embedded in the Bethesda guidelines. This panel consisted of 2 mononucleotide repeats (BAT-25, BAT-26) and 3 dinucleotide repeats (D2S123, D5S346, D17S250) (34 ). Several other panels that have since been described include the moresensitive mononucleotide markers (35 ). Many laboratories currently use a commercially available panel (Promega Corporation) that includes 5 mononucleotide markers (BAT-25, BAT-26, MONO-27, NR-21, NR-24) and 2 pentanucleotide markers (Penta C, 114 Clinical Chemistry 60:1 (2014) Penta D) to identify the tumor and healthy tissue as arising from the same individual. If instability in ⱖ2 of the 5 markers is detected, the tumor is classified as MSI-H. Instability in only 1 of the 5 markers is considered MSI low, and instability in none of the markers is considered MSI stable. The newest panel contains quasimonomorphic mononucleotide repeats with an increased diagnostic sensitivity, which allows for the detection of MSI in tumor tissue without the need for testing healthy tissue; however, this practice has not been widely adopted (36, 37 ). If only a single modality is to be chosen, there are 2 main reasons why screening with IHC might be preferred to MSI testing. First, MSH6 mutations may not show MSI-H; therefore, these cases would not be flagged for additional testing. Of 6 patients with MSH6 mutations in a study by Hampel et al., 1 was MSI stable, 2 were MSI low, and 3 were MSI-H (5 ). This result is particularly relevant, because the likelihood of an EC Lynch Syndrome and Endometrial Cancer Reviews Fig. 2. In MSI testing, control genomic DNA from a blood sample is compared with genomic DNA from a patient’s tumor. Seven MSI markers are evaluated in this assay (5 mononucleotides on the left and 2 pentanucleotides on the right); the arrow indicates markers that show instability when comparing the 2 samples. MSI at ⱖ2 of the 5 mononucleotide markers indicates MSI-H. patient having an MSH6 mutation is 5-fold higher than that of a CRC patient and because the lifetime risk for EC may be as high as 70% in patients with MSH6 mutations. Additionally, these patients often have an older age at presentation (5, 38 ). The second reason is that although in CRC a somatic BRAF (v-raf murine sarcoma viral oncogene homolog B) p.V600E mutation is present in about 64% of sporadic tumors with a loss of MLH1 expression as detected by IHC (likely due to MHL1 methylation), a similar test is not currently available for LS-associated EC (39 ). Djordjevic et al. recently showed that positive IHC results for PTEN in nonendometrioid (but not endometrioid) carcinomas is associated with a high likelihood of intact MMR (as detected by IHC staining), suggesting that PTEN IHC positivity combined with histology data may also become clinically useful for detecting sporadic nonendometrioid EC (40 ). MLH1-METHYLATION TESTING MSI associated with LS is caused mainly by inherited mutations in MMR genes, but somatic hypermethyl- ation of the MLH1 promoter also leads to MSI in sporadic tumors. MLH1 methylation is found in about 15%–30% of all ECs (75% of MSI-H cases) (25 ). The majority of these tumors will also test negative for MLH1 and PMS2 by IHC analysis, a result that is indicative of a silenced MLH1 gene. Testing for MLH1 promoter hypermethylation can be used to distinguish sporadic tumors from those that are likely to be associated with LS and require additional gene sequencing. Methylation occurs on cytosine residues of CpG islands in the promoter region of the MLH1 gene. Promoter methylation is one form of epigenetic gene regulation. The methyl groups on the cytosine residues protrude into the major groove of the DNA molecule and sterically hinder the ability of transcription factors to anneal to the DNA, thereby blocking DNA transcription. Methylation also attracts methyl-binding proteins, which cause chromatin compaction and gene silencing (41 ). The majority of methods for MLH1-methylation analysis begin with the conversion of unmethylated cytosine to uracil by sodium bisulfite. The methylated Clinical Chemistry 60:1 (2014) 115 Reviews cytosine is left intact and can be detected with a variety of methods. One common method is the MethyLight assay, a quantitative real-time PCR assay for DNA methylation. A patient’s sample is amplified with specific primers for MLH1 and a control gene and then compared with a methylated control sample to determine the percent methylation (42 ). Additional detection techniques include methylation-specific multiplex ligation-dependent probe amplification, methylationspecific melt curve analysis, pyrosequencing, and methylation-specific PCR followed by capillary electrophoresis (40, 42 ). A positive MLH1-methylation result indicates MLH1 silencing via sporadic promoter hypermethylation. DNA SEQUENCING FOR SCREENING OF LS IN EC Current testing practices in the setting of LS include screening assays that use IHC and MSI analysis, which may suggest the presence of a germ line mutation. These assays are typically followed by Sanger sequencing of the MMR genes to identify specific mutations. This type of testing algorithm has been developed because of the high cost of routine germ line screening via Sanger sequencing. When used in combination, these former assays can be effective in identifying probable LS-related tumors. These tests have certain limitations, however, that make alternative testing modalities desirable. IHC and MSI testing have a demonstrated false-negative rate of 5%–10%, and MSI is present in about 10% of all CRCs (22, 30 ). IHC analysis can be limited by variation in staining patterns, which can lead not only to uncertain interpretation but also to decreased efficacy with small biopsy samples, for which staining may be difficult to visualize. MLH1 gene expression can also be problematic for IHC testing, because ⬎33% of mutations in this gene are missense mutations that encode proteins that are both functionally inactive and antigenically intact (therefore producing a normal staining pattern). Finally, neither of these tests is capable of identifying the specific germ line mutation; thus, additional testing is required for diagnostic and counseling purposes. Typical genetic analysis of the MMR genes would consist of single-gene (Sanger) sequencing to identify potential mutations. As a screening approach, Sanger sequencing would not be cost-effective or timely for identifying MMR gene mutations. On the other hand, massively parallel sequencing or next-generation sequencing has great potential as a diagnostic or screening assay for directly identifying MMR gene mutations (43 ). Use of this new molecular technique allows simultaneous sequencing of multiple genes and multiple patient samples to identify mutations of interest (44 ). 116 Clinical Chemistry 60:1 (2014) Whereas Sanger sequencing was previously reserved as a final confirmatory step in the testing protocol, but owing to its cost and long turnaround time, the advent of next-generation sequencing technology has made it possible and affordable to sequence all of the LS-causative genes in parallel. It is also possible to bar code and sequence multiple patient samples simultaneously, which would further reduce the costs and time necessary to deliver actionable clinical data (43 ). As more laboratories move testing to nextgeneration sequencing platforms, we will experience a substantial increase in throughput and a decrease in costs compared with traditional Sanger-sequencing methods. Using instruments such as the Illumina MiSeq and the Ion Torrent Personal Genome Machine (PGM™), laboratories have already designed and implemented next-generation sequencing assays for the MMR genes, which have led to a cost- and performance-competitive analysis scheme (43 ). We have developed a next-generation sequencing assay that uses the Ion Torrent PGM. The design of a custom panel allows the greatest possible coverage of the region to be sequenced. PGM custom panels can cover up to 1 Mb of genomic targets, and amplicons can be optimized for formalin-fixed paraffin-embedded samples. The primers for these types of sequencing reactions can be padded to increase the coverage of the exon regions for the gene(s) of interest. Our assay design produced an MMR panel consisting of 2 primer pools that produce 85 and 87 amplicons. This design approach allowed us to achieve a predicted coverage of the coding regions for the 5 MMR genes of ⬎92%. Our ability to sequence all of the MMR genes of interest and to combine bar-coded patient samples into a single sequencing run makes it conceivable for such an assay to replace much of the IHC and MSI testing in LS. Genetic Counseling and Hereditary Cancer Syndromes Approximately 2.5% of all ECs are due to LS (35 ). LS is inherited in an autosomal dominant fashion, meaning that an individual who has this condition has a 50% chance of passing it on to each of their offspring. In addition, most individuals with LS have inherited the condition from a parent (45 ). Families with LS, as with other hereditary cancer syndromes, typically exhibit the following key features: (a) an early age of cancer diagnosis, (b) an autosomal dominant inheritance pattern of the cancer, (c) multiple relatives within 1 generation affected with similar types of cancers, (d) an excess of multiple primary cancers, (e) the presence of other nonmalignant features, and (f) the occurrence of rare cancers (45 ). Reviews Lynch Syndrome and Endometrial Cancer The process of genetic counseling and risk assessment for LS uses a variety of tools to help identify whether an individual is at high risk. These tools include pedigree (family history) analysis, risk modeling, genetic testing, biochemical testing, imaging, and, in some cases, evaluation of physical features (46 ). If a patient is identified as an appropriate candidate for genetic testing, the testing process is discussed with the patient in greater depth. Such discussions include a review of the possible test results, as well as other issues: the risk of uncovering a genetic variant of unknown clinical significance; the risks, benefits, and limitations of testing; the implications for medical management based on the possible test results; and the potential psychosocial implications of testing (45 ). Ultimately, all of the information gathered, including the results of genetic testing if pursued, is combined to develop a personalized management plan for cancer screening, risk reduction, and prevention (46 ). Furthermore, when an individual is found to have LS, the identification and notification of at-risk relatives often becomes an integral extension of the genetic-counseling process. Multiple publications have detailed when to refer patients for genetic counseling in the context of hereditary cancer syndromes. Regarding LS specifically, a brief overview of appropriate referrals includes (a) individuals meeting the revised Bethesda criteria, (b) individuals from a family meeting the Amsterdam criteria, (c) individuals with ⬎10 adenomas, or (d) individuals from a family with a known LS mutation. The 2012 NCCN guidelines (47 ) provide a more comprehensive overview of appropriate referral indications. PREVENTIVE SCREENING The main cancer risks for women with LS include a 40%– 80% risk for colon cancer, a 25%– 60% risk for EC, and a 10%–12% risk for ovarian cancer (48 –51 ). A smaller— but still increased—risk of urinary tract, small bowel, stomach, biliary tract, and brain tumors also exists (48 –50 ). For ECs specifically, the median age of diagnosis is approximately 48 – 62 years of age (51, 52 ). Screening for the gynecologic malignancies associated with LS is less well established than the screening recommendations for colon cancer. A few published studies have investigated screening for EC in LS patients, but the results have been conflicting. One study showed that annual transvaginal ultrasound followed by endometrial biopsy in the setting of an abnormal ultrasound result detected 3 premalignant lesions; however, this method failed to detect an actual EC that was ultimately detected from symptoms (53 ). A second study showed that a transvaginal ultrasound examination every 1 to 2 years failed to detect 2 ECs (54 ). In contrast, a Finnish study showed that the use of endo- metrial biopsy and transvaginal ultrasound together detected EC better than transvaginal ultrasound alone. Eleven of 14 ECs were diagnosed via endometrial biopsy, compared with 8 of 14 ECs diagnosed via ultrasound alone (55 ). Because many early-stage ECs present with such symptoms as abnormal vaginal bleeding, however, it is still not clear whether heightened surveillance ultimately improves cancer detection and survival (56 ). The NCCN Clinical Practice Guidelines in Oncology (47 ) recommend that female LS carriers be educated about the signs and symptoms of EC, as well as the importance of seeking prompt medical attention should any of these symptoms present. Several groups have proposed possible ECscreening protocols for LS carriers that could include the following: referral to a gynecologic oncologist for screening, total hysterectomy and bilateral salpingooophorectomy, transvaginal ultrasound beginning at 30 –35 years of age, and endometrial biopsy, if indicated (47, 57–59 ). With regard to the other cancers associated with LS, increased surveillance via colonoscopy screening and subsequent removal of polyps have been shown to be effective in reducing the incidence of colon cancer in carriers (47, 56 ). The effectiveness of screening for the extracolonic cancers has yet to be determined, however. Information on screening for both the colon and extracolonic cancers associated with LS is available (47, 57, 60 ). GENETIC-COUNSELING COMPLEXITIES Historically, genetic testing for LS has been based on the fulfillment of specific clinical criteria. The original clinical guidelines, known as the Amsterdam criteria, were proposed by the International Collaborative Group on HNPCC in 1991. These guidelines were subsequently revised to the Amsterdam II criteria (61 ). Although they were the first guidelines to define LS with the hope of determining the underlying genetic etiology, they had low diagnostic sensitivity and limited applicability in clinical practice. Further delineation of the clinical criteria by the National Cancer Institute produced the Bethesda guidelines, which helped establish which patients should pursue tumor testing via MSI analysis (28 ). Not all individuals with LS will fulfill these criteria, however, and the guidelines are somewhat cumbersome to use in clinical practice (62 ). That is particularly true for carriers of PMS2 mutations, because the penetrance and lifetime cancer risks associated with mutations in this gene are much lower than the cancer risks associated with the MLH1 and MSH2 genes (63 ). Recently, there has been a push toward universal screening via tumor testing for LS, because the vast majority of these cancers exhibit MMR deficiency Clinical Chemistry 60:1 (2014) 117 Reviews Blue line indicates paent-reported cancer history at inial genec-counseling session Red line indicates paent-reported cancer history aer gathering more family history informaon Black line indicates no cancer history Colon cancer Endometrial cancer Colon polyps Non-LS cancer Fig. 3. A 3-generation pedigree for the family of a 64-year-old woman who was referred to our Familial Cancer Program because of a history of EC. and thus can be detected via either MSI or IHC approaches (discussed above) (64 ). Furthermore, the current clinical guidelines (both Revised Bethesda and Amsterdam II) will miss a substantial number of LS cases (65 ). The following case report illustrates some of the abovementioned complexities associated with genetic counseling for LS. It also addresses an additional issue unique to PMS2—the PMS2CL (PMS2 C-terminal like pseudogene) pseudogene (66 ). A 64-year-old woman was referred to our Familial Cancer Program because of a history of EC, diagnosed at 61 years of age. She also had a history of basal cell carcinoma, which was diagnosed at age 60 years. A 3-generation pedigree was obtained at her initial genetic-counseling visit; however, she noted that she did not have much information regarding her family history of cancer and that she had a very large extended family (Fig. 3). The family history was notable for the following: a sister with cervical cancer, diagnosed at age 28 years; a brother with basal cell 118 Clinical Chemistry 60:1 (2014) carcinoma, diagnosed at age 58 years; and a nephew with colon cancer, diagnosed at age 38 years. The maternal family history was notable for the following: a maternal uncle with liver cancer, diagnosed at age 76 years; 2 maternal aunts with skin cancer, diagnosed at ⬎70 years of age; a maternal aunt with lung cancer, diagnosed in her late 30s; and a maternal great-grandmother diagnosed with uterine cancer in her 40s. The paternal family history was notable for the following: her father, who was diagnosed with skin cancer at age 90 years; a paternal aunt, diagnosed with leukemia in her 30s; and a paternal grandmother, who was diagnosed with colon cancer in her 50s and breast cancer at age 59 years. On review of this pedigree, the patient’s family did not meet the Amsterdam II criteria, because there was no Lynch-associated cancer in her father’s generation. Our patient did not fulfill any of the revised Bethesda guidelines either, but her nephew did. At the time of her initial visit, no additional testing was indicated; however, after learning about LS and the importance of Reviews Lynch Syndrome and Endometrial Cancer an accurate family history, the patient became very motivated and reached out to family members for any relevant cancer history information that she lacked. The patient recontacted the genetic counselor after obtaining a much more comprehensive paternal family history. The following additional information was revealed: 2 sisters with multiple adenomatous colon polyps; a paternal uncle with colon cancer, diagnosed around the age of 70 years; a paternal aunt with colon cancer, diagnosed in her late 60s/early 70s; a second paternal aunt with colon cancer, diagnosed in her late 60s/early 70s; a paternal aunt with a history of colon polyps; her paternal grandfather with colon and stomach cancer, diagnosed at approximately 70 years of age; and finally, a paternal first cousin with colon cancer, diagnosed at 61 years. The additional family history markedly changed the interpretation of this patient’s risk of being an LS carrier. Indeed, her family now fulfilled the Amsterdam II criteria, and further testing was very much warranted. An IHC analysis of her EC sample revealed complete loss of the PMS2 protein. Her blood sample was then sent out for PMS2 gene sequencing and deletion/duplication analysis. This testing was performed at a CLIA-approved commercial laboratory in the fall of 2010. The initial results of the testing were inconclusive. After speaking with the laboratory, we determined that the patient likely had a pathogenic mutation within the PMS2 gene, specifically deletion of exons 14 and 15; however, this part of her testing had been done in the research section of the laboratory. The laboratory was currently in the process of clinically validating the methodology, which would be able to detect such large deletions within PMS2; therefore, the laboratory could issue only an inconclusive result. Part of the issue with the clinical validation stemmed from the fact that this region of the PMS2 gene contains the PMS2CL pseudogene, which complicates an accurate analysis. After an additional 9 months, the patient’s report was amended to show that she carried a deleterious mutation in the PMS2 gene (i.e., deletion of exons 14 and 15), as expected. Clinical validation of this mutation has subsequently allowed us to test other family members. To date, 2 additional family members have been tested: One has tested positive for the known mutation, and the other is a true negative. This case highlights some of the important issues surrounding genetic counseling for LS. First, it shows how critical an accurate family history is for a precise risk assessment (46 ). The 3-generation pedigree is the foundation that guides the majority of the discussion in counseling patients about hereditary cancer syndromes (46 ). This case nicely demonstrates how the interpretation of an individual’s risk of being a carrier can change dramatically, depending on the patient’s knowledge of the pertinent family history. Initially, we were not too concerned about the possibility for LS, but the likelihood for LS became much greater after we acquired the additional information. Second, testing for LS is unique, in that 4 separate genes can produce a similar clinical phenotype. Use of IHC analysis can often narrow down the choices to 1 or 2 genes, thus allowing tailoring of the testing strategy and eliminating unnecessary and costly testing (62 ). As mentioned above, there has been a recent push to institute universal tumor testing via IHC or MSI analysis (64 ). Such testing is increasingly commonplace in the setting of CRC; however, it remains less routine in the setting of EC (66 ). Had universal tumor testing of ECs been implemented at the time our patient was diagnosed, the loss of PMS2 would have been detected, and the patient’s clinicians would have been alerted to her increased risk of LS early on in her cancer treatment. Additionally, had this patient not been motivated to obtain more of her family history, she likely would have gone undiagnosed, perhaps until she developed a second LS-associated cancer. Universal tumor testing would allow an alternative means for identifying LS patients, especially in the setting in which the patient does not have the means to obtain additional family history information. Finally, this case illustrates the complexities of gene mutation analysis and how genetic technology is constantly changing. Analysis of the PMS2 gene has historically been hampered by the presence of 15 pseudogenes located on the same chromosome (65 ). One pseudogene in particular, PMS2CL, contains 6 of the PMS2 exons (9, 11–15, 67 ). Owing to the frequency of recombination and/or gene conversion between PMS2 and PMS2CL, there is a high rate of producing hybrid PMS2/PMS2CL alleles, which makes reliable analysis very difficult, especially in the 3⬘ region of the gene (68 ). Conclusion LS is the most common form of hereditary CRC, and universal screening programs for all CRCs are being implemented nationwide. Women with LS have a substantial risk of developing EC as their first tumor type and therefore require testing to determine if the EC is LS related. Identifying the EC as LS related can lead to screening, early detection, and prevention of other LSrelated tumors, including CRC. A better understanding of the role and mutation spectrum of MMR genes and the advent of newer technologies, such as massively parallel sequencing, could improve screening for LS via more-direct and cost-effective mutation analysis. Clinical Chemistry 60:1 (2014) 119 Reviews Author Contributions: All authors confirmed they have contributed to the intellectual content of this paper and have met the following 3 requirements: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; and (c) final approval of the published article. Authors’ Disclosures or Potential Conflicts of Interest: No authors declared any potential conflicts of interest. References 1. American Cancer Society. Cancer facts & figures 2013. http://www.cancer.org/acs/groups/content/ @epidemiologysurveilance/documents/document/ acspc-036845.pdf (Accessed October 2013). 60 p. 2. National Cancer Institute. Genetics of colorectal cancer (PDQ姞). http://www.cancer.gov/cancertopics/ pdq/genetics/colorectal (Accessed June 2013). 3. Patel SG, Ahnen DJ. Familial colon cancer syndromes: an update of a rapidly evolving field. Curr Gastroenterol Rep 2012;14:428 –38. 4. Vasen HF, Blanco I, Aktan-Collan K, Gopie JP, Alonso A, Aretz S, et al. Revised guidelines for the clinical management of Lynch syndrome (HNPCC): recommendations by a group of European experts. Gut 2013;62:812–23. 5. Hampel H, Frankel W, Panescu J, Lockman J, Sotamaa K, Fix D, et al. Screening for Lynch syndrome (hereditary nonpolyposis colorectal cancer) among endometrial carcinoma patients. Cancer Res 2006;66:7810 –7. 6. Hampel H, Panescu J, Lockman J, Sotamaa K, Fix D, Comeras I, et al. Comment on: Screening for Lynch syndrome (hereditary nonpolyposis colorectal cancer) among endometrial cancer patients. Cancer Res 2007;67:9603. 7. Warthin AS. Heredity with reference to carcinoma as shown by the study of the cases examined in the pathological laboratory of the University of Michigan, 1895–1913. Arch Intern Med 1913;35: 348 –59. 8. Lynch HT, Shaw MW, Magnuson CW, Larsen AL, Krush AJ. Hereditary factors in cancer: study of two large midwestern kindreds. Arch Intern Med 1966;117:206 –12. 9. Barrow E, Hill J, Evans DG. Cancer risk in Lynch syndrome. Familial Cancer 2013;12:229 – 40. 10. Wang Y, Wang Y, Li J, Cragun J, Hatch K, Chambers SK, Zheng W. Lynch syndrome related endometrial cancer: clinical significance beyond the endometrium. J Hematol Oncol 2013;6:22. 11. Kunkel TA, Erie DA. DNA mismatch repair. Annu Rev Biochem 2005;74:681–710. 12. Greenson JK, Huang SC, Herron C, Moreno V, Bonner JD, Tomsho, et al. Pathologic predictors of microsatellite instability in colorectal cancer. Am J Surg Pathol 2009;33:126 –33. 13. Funkhouser WK Jr, Lubin IM, Monzon FA, Zehnbauer BA, Evans JP, Ogino S, et al. Relevance, pathogenesis and testing algorithm for mismatch repair-defective colorectal carcinomas: a report of the Association for Molecular Pathology. J Mol Diagn 2012;14:91–103. 14. Moreira L, Balaguer F, Lindor N, de la Chapelle A, Hampel H, Aaltonen LA, et al. Identification of Lynch syndrome among patients with colorectal cancer. JAMA 2012;208:1555– 65. 15. Weissman SM, Burt R, Church J, Erdman S, Hampel H, Holter S, et al. Identification of individuals at risk for Lynch syndrome using targeted evaluations and genetic testing: National Society of Genetic Counselors and the Collaborative Group 120 Clinical Chemistry 60:1 (2014) 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. of the Americas on Inherited Colorectal Cancer joint practice guideline. J Genet Couns 2012;21: 484 –93. Recommendations from the EGAPP Working Group: genetic testing strategies in newly diagnosed individuals with colorectal cancer aimed at reducing morbidity and mortality from Lynch syndrome in relatives. Genet Med 2009;11:35– 41. Lu KH, Dinh M, Kohlmann W, Watson P, Green J, Syngal S, et al. Gynecologic cancer as a “sentinel cancer” for women with hereditary nonpolyposis colorectal cancer syndrome. Obstet Gynecol 2005;105:569 –74. Broaddus RR, Lynch HT, Chen LM, Daniels MS, Conrad P, Munsell MF, et al. Pathologic features of endometrial carcinoma associated with HNPCC: a comparison with sporadic endometrial carcinoma. Cancer 2006;106:87–94. Garg K, Leitao MM Jr, Kauff ND, Hansen J, Kosarin K, Shia J, et al. Selection of endometrial carcinomas for DNA mismatch repair protein immunohistochemistry using patient age and tumor morphology enhances detection of mismatch repair abnormalities. Am J Surg Pathol 2009;33: 925–33. Jensen KC, Mariappan MR, Putcha GV, Husain A, Chun N, Ford JM, et al. Microsatellite instability and mismatch repair protein defects in ovarian epithelial neoplasms in patients 50 years of age or younger. Am J Surg Pathol 2008;32:1029 –37. Lu FI, Gilks CB, Mulligan AM, Ryan P, Allo G, Sy K, et al. Prevalence of loss of expression of DNA mismatch repair proteins in primary epithelial ovarian tumors. Int J Gynecol Pathol 2012;31: 524 –31. Shia J, Black D, Hummer AJ, Boyd J, Soslow RA. Routinely assessed morphological features correlate with microsatellite instability status in endometrial cancer. Hum Pathol 2008;39:116 –25. Tafe LJ, Garg K, Chew I, Tornos C, Soslow RA. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently under-recognized neoplasms. Mod Pathol 2010;6:781–9. Silva EG, Deavers MT, Bodurka DC, Malpica A. Association of low-grade endometrioid carcinoma of the uterus and ovary with undifferentiated carcinoma: a new type of dedifferentiated carcinoma? Int J Gynecol Pathol 2006;25:52– 8. Garg K, Soslow RA. Lynch syndrome (hereditary non-polyposis colorectal cancer) and endometrial carcinoma. J Clin Pathol 2009;62:679 – 84. Ryan P, Mulligan AM, Aronson M, Ferguson SE, Bapat B, Semotiuk K, et al. Comparison of clinical schemas and morphologic features in predicting Lynch syndrome in mutation-positive patients with endometrial cancer encountered in the context of familial gastrointestinal cancer registries. Cancer 2012;118:681– 8. Westin SN, Lacour RA, Urbauer DL, Luthra R, Bodurka DC, Lu KH, et al. Carcinoma of the lower 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. uterine segment: a newly described association with Lynch syndrome. J Clin Oncol 2008;26: 5965–71. Umar A, Boland CR, Terdiman JP, Syngal S, de la Chapelle A, Rüschoff J, et al. Revised Bethesda guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst 2004;96:261– 8. Beamer LC, Grant ML, Espenschied CR, Blazer KR, Hampel HL, Weitzel JN, MacDonald DJ. Reflex immunohistochemistry and microsatellite instability testing of colorectal tumors for Lynch syndrome among US cancer programs and followup of abnormal results. J Clin Oncol 2012;30: 1058 – 63. National Comprehensive Cancer Network. NCCN guidelines: NCCN guidelines for detection, prevention, & risk reduction: colorectal cancer screening. http://www.nccn.org/professionals/physician㛭gls/ f㛭guidelines.asp#colorectal㛭screening (Accessed September 2013). Shia J. Immunohistochemistry versus microsatellite instability testing for screening colorectal cancer patients at risk for hereditary nonpolyposis colorectal cancer syndrome. Part I. The utility of immunohistochemistry. J Mol Diagn 2008;10: 293–300. Modica I, Soslow RA, Black D, Tornos C, Kauff N, Shia J. Utility of immunohistochemistry in predicting microsatellite instability in endometrial carcinoma. Am J Surg Pathol 2007;31:744 –51. Geiersbach KB, Samowitz WS. Microsatellite instability in colorectal cancer. Arch Pathol Lab Med 2011;135:1269 –77. Boland CR, Thibodeau SN, Hamilton SR, Sidransky D, Eshleman JR, Burt RW, et al. A National Cancer Institute workshop on microsatellite instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res 1998;58: 5248 –57. Cicek MS, Lindor NM, Gallinger S, Bapat B, Hopper JL, Jenkins MA, et al. Quality assessment and correlation of microsatellite instability and immunohistochemical markers among population- and clinic-based colorectal tumors: colorectal tumors results from the Colon Cancer Family Registry. J Mol Diagn 2011;13:271– 81. Soreide K. High fidelity of five quasimonomorphic mononucleotide repeats to high frequency microsatellite instability distribution in early stage adenocarcinoma of the colon. Anticancer Res 2011; 31:967–72. Deschoolmeester V, Baay M, Wuyts W, Van Marck E, Van Damme N, Vermeulen P, et al. Detection of microsatellite instability in colorectal cancer using an alternative multiplex assay of quasi-monomorphic mononucleotide markers. J Mol Diagn 2008;10:154 –9. Hendriks YM, Wagner A, Morreau H, Menko F, Reviews Lynch Syndrome and Endometrial Cancer 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. Stormorken A, Quehenberger F, et al. Cancer risk in hereditary nonpolyposis colorectal cancer due to MSH6 mutations: impact on counseling and surveillance. Gastroenterology 2004;127:17–25. Parsons MT, Buchanan DD, Thompson B, Young JP, Spurdle AB. Correlation of tumour BRAF mutations and MLH1 methylation with germline mismatch repair (MMR) gene mutation status: a literature review assessing utility of tumour features for MMR variant classification. J Med Genet 2012;49:151–7. Djordjevic B, Barkoh BA, Luthra R, Broaddus RR. Relationship between PTEN, DNA mismatch repair, and tumor histotype in endometrial carcinoma: retained positive expression of PTEN preferentially identifies sporadic non-endometrioid carcinomas. Mod Pathol 2013;26:1401–12. Esteller M. Cancer epigenomics: DNA methylomes and histone-modification maps. Nat Rev Genet 2007;8:286 –98. Pérez-Carbonell L, Alenda C, Payá A, Castillejo A, Barberá VM, Guillén C, et al. Methylation analysis of MLH1 improves the selection of patients for genetic testing in Lynch syndrome. J Mol Diagn 2010;12:498 –504. Pritchard CC, Smith C, Salipante SJ, Le MK, Thornton AM, Nord AS, et al. ColoSeq provides comprehensive Lynch and polyposis syndrome mutational analysis using massively parallel sequencing. J Mol Diagn 2012;14:357– 66. Abou Tayoun AN, Tunkey CD, Pugh TJ, Ross T, Shah M, Le CC, et al. A comprehensive assay for CFTR mutational analysis using next-generation sequencing. Clin Chem 2013;59:1481– 8. Schneider KA. Counseling about cancer: strategies for genetic counseling, 3rd ed. Hoboken, NJ: Wiley-Blackwell; 2012. Riley BD, Culver JO, Skrzynia C, Senter LA, Peters JA, Costalas JW, et al. Essential elements of genetic cancer risk assessment, counseling, and testing: updated recommendations of the National Society of Genetic Counselors. J Genet Couns 2012;21:151– 61. National Comprehensive Cancer Network. NCCN Guidelines姞 [NCCN Clinical Practice Guidelines in Oncology]. http://www.nccn.org/professionals/ physician_gls/f_guidelines.asp#detection (Accessed December 2013). Vasen HF, Wijnen JT, Menko FH, Kleibeuker JH, Taal BG, Griffioen G, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. diagnosed by mutation analysis. Gastroenterology 1996;110:1020 –7. Stoffel E, Mukherjee B, Raymond VM, Tayob N, Kastrinos F, Sparr J, et al. Calculation of risk of colorectal and endometrial cancer among patients with Lynch syndrome. Gastroenterology 2009;137:1621–7. Aarnio M, Sankila R, Pukkala E, Salovaara R, Aaltonen LA, de la Chapelle A, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer 1999;81:214 – 8. Hampel H, Stephens JA, Pukkala E, Sankila R, Aaltonen LA, Mecklin JP, et al. Cancer risk in hereditary nonpolyposis colorectal cancer syndrome: later age of onset. Gastroenterology 2005;129:415–21. Vasen HF, Watson P, Mecklin JP, Jass JR, Green JS, Nomizu T, et al. The epidemiology of endometrial cancer in hereditary nonpolyposis colorectal cancer. Anticancer Res 1994;14:1675– 8. Rijcken FE, Mourits MJ, Kleibeuker JH, Hollema H, van der Zee AG. Gynecologic screening in hereditary nonpolyposis colorectal cancer. Gynecol Oncol 2003;91:74 – 80. Dove-Edwin I, Boks D, Goff S, Kenter GG, Carpenter R, Vasen HF, et al. The outcome of endometrial carcinoma surveillance by ultrasound scan in women at risk of hereditary nonpolyposis colorectal carcinoma and familial colorectal carcinoma. Cancer 2002;94:1708 –12. Renkonen-Sinisalo L, Bützow R, Leminen A, Lehtovirta P, Mecklin J-P, Järvinen HJ. Surveillance for endometrial cancer in hereditary nonpolyposis colorectal cancer syndrome. Int J Cancer 2007;120:821– 4. Järvinen HJ, Renkonen-Sinisalo L, Aktán-Collán K, Peltomäki P, Aaltonen LA, Mecklin JP. Ten years after mutation testing for Lynch syndrome: cancer incidence and outcome in mutation-positive and mutation-negative family members. J Clin Oncol 2009;27:4793–7. Weissman SM, Bellcross C, Bittner CC, Freivogel ME, Haidle JL, Kaurah P, et al. Genetic counseling considerations in the evaluation of families for Lynch syndrome—a review. J Genet Couns 2011; 20:5–19. Lindor NM, Petersen GM, Hadley DW, Kinney AY, Miesfeldt S, Lu KH, et al. Recommendations for the care of individuals with an inherited predisposition to Lynch syndrome: a systematic review. JAMA 2006;296:1507–17. 59. Vasen HF, Möslein G, Alonso A, Bernstein I, Bertario L, Blanco I, et al. Guidelines for the clinical management of Lynch syndrome (hereditary non-polyposis cancer). J Med Genet 2007;44: 353– 62. 60. Koornstra JJ, Mourits MJ, Sijmons RH, Leliveld AM, Hollema H, Kleibeuker JH. Management of extracolonic tumours in patients with Lynch syndrome. Lancet Oncol 2009;10:400 – 8. 61. Vasen HF, Watson P, Mecklin JP, Lynch HT. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative Group on HNPCC. Gastroenterology 1999;116:1453– 6. 62. Hampel H, Frankel WL, Martin E, Arnold M, Khanduja K, Kuebler P, et al. Screening for the Lynch syndrome (hereditary nonpolyposis colorectal cancer). N Engl J Med 2005;352:1851– 60. 63. Senter L, Clendenning M, Sotamaa K, Hampel H, Green J, Potter JD, et al. The clinical phenotype of Lynch syndrome due to germ-line PMS2 mutations. Gastroenterology 2008;135:419 –28. 64. Moreira L, Balaguer F, Lindor N, de la Chapelle A, Hampel H, Aaltonen LA, et al. Identification of Lynch syndrome among patients with colorectal cancer. JAMA 2012;308:1555– 65. 65. Wernstedt A, Valtorta E, Armelao F, Togni R, Girlando S, Baudis M, et al. Improved multiplex ligation-dependent probe amplification analysis identifies a deleterious PMS2 allele generated by recombination with crossover between PMS2 and PMS2CL. Genes Chromosomes Cancer 2012;51: 819 –31. 66. Moline J, Mahdi H, Yang B, Biscotti C, Roma AA, Heald B, et al. Implementation of tumor testing for Lynch syndrome in endometrial cancers at a large academic medical center. Gynecol Oncol 2013;130:121– 6. 67. De Vos M, Hayward BE, Picton S, Sheridan E, Bonthron DT. Novel PMS2 pseudogenes can conceal recessive mutations causing a distinctive childhood cancer syndrome. Am J Hum Genet 2004;74:954 – 64. 68. van der Klift HM, Tops CM, Bik EC, Boogaard MW, Borgstein AM, Hansson KB, et al. Quantification of sequence exchange events between PMS2 and PMS2CL provides a basis for improved mutation scanning of Lynch syndrome patients. Hum Mutat 2010;31:578 – 87. Clinical Chemistry 60:1 (2014) 121