Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Staphylococcus aureus wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
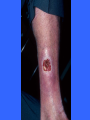
Common Dermatologic Conditions Toby Maurer, MD University of California, San Francisco Acne • Papulopustular – Topicals okay • Cystic, scarring, keloidal – p.o. antibiotics – Accutane Topicals • BP 5% gel (10% - more drying) • Retin A 0.025% - 0.1% ( vehicle determines strength - start with crème) • Cleocin T or erythromycin topically – Use 1 qam and 1qhs – If NO success after 8 weeks, go to p.o.’s P.O. Antibiotics • • • • TCN - 500 bid x 8 weeks Doxycycline - 100 bid x 8 weeks Minocycline - 100 bid x 8 weeks Taper - Do NOT STOP ABRUPTLY Alternatives • Erythromycin - 500 bid • Septra - check WBC’s • Keflex-500 tid Spiranolactone • Diuretic used in cirrhosis of liver • Also an anti-androgen • Useful in females who have cysts around menstruation • 50-100 mg qday continuously • Increased urination, don’t use during pregnancy, ?electrolyte imbalance Accutane • Document failure of antibiotics • Baseline CBC, LFT’s ,TG and cholesterol • Two forms of birth control, negative pregnancy tests • MD’s will need to be registered as will patients • Counseling on depression Acne Rosacea • • • • Common in women over 40 Often seen in persons of Irish decent Associated with seborrheic dermatitis Characterized by papules, erythema, telangiectasia and rhinophyma (M>F) • Sun exposure, alcohol and spicy foods exacerbate rosacea Acne Rosacea • Oral antibiotics for 6-8 weeks clears skin for some amount of time • Topicals work less frequently Perioral Dermatitis TREATMENT Topicals: Cleocin T Gel bid Erythromycin bid p.o. antibiotics –TCN Doxycycline Minocycline - bid x 8 wks Keeps pts in remission x 2 yrs. Hair Loss • • • • Decide if scarring or not: If scarring-refer If not scarring and diffuse: Check recent surgeries/illness, nutrition, anemia, TSH, estrogen replacement, medication history, VDRL. • If hirsute with scalp hair loss-DHEAS and free testosterone • If lactating- check prolactin If all negative • Androgenetic AlopeciaMinoxidil 5% bid topically (even in women) Can make hair oily-may want to start with minoxidil 2% or use 2% by day and 5% at night Use for at least 6 months for results and what you see after 1 yr. is the effect you can expect. What about finasteride (propecia)?-equal to minoxidil in men. Does not work in women. Too Much Hair • Vaniqa – topical cream that breaks the chemical bond of hair – apply 2x’s/day forever – 30% effective – $30/month Hair Removal – pigment of hair absorbs the light and is destroyed – dark hair responds – hair is always in different growth phases, so treatment has to be repeated several times to catch the phase(expensive) – Side effects: pigment changes of surrounding skin and scarring Psoriasis-What is it? • Fast growing skin-takes 3 days to come to surface and desquamate • Normal rate is 28 days • Psoriatic skin has a fast mitotic rate • Triggers an inflammatory response in and around affected skin • New onset often preceded by strep infection (strep pharyngitis) especially in the younger age group. • In older age group, drugs often unmask psoriasis • Drugs: beta-blockers, lithium, NSAIDS, antimalarials, terbinafine, gemfibrozilpts on these meds for 3-6 months before onset of psoriasis Psoriasis-Tx: • Decrease the mitotic rate of skin – Tar (LCD 5% in TAC 0.1% oint) ( Tar emulsions), topical retinoids (Tazarac) • Decrease the inflammatory response of the skin – Steroid Ointment (mid-potency-1st line) – Calcipotriene (Dovonex Ointment)-not on face or groin – Clobetasol/Dovonex combination – Ultraviolet light (psoralen+ UVA), UVB – NO PREDNISONE NEXT STEP • Time for referral • Methotrexate-liver biopsies necessary(don’t give in HEP C pts) • Oral retinoids (Acetretin)-not in persons of reproductive potential -? Okay in liver disease; excellent drug in HIV • Cyclosporine • Biologics (Enbrel, Remicade)-most benefit in psoriatic arthritis and quick reversal of pustular psoriasis Eczema • • • • • • Dry, inflamed skin that becomes “weepy” Not bilateral and symmetric No thick scale No scalp/nail involvement Topical steroids first line of treatment Oral cyclosporine was known to turn off inflammation • Now: topical formulation of Cyclosporine Eczema • Tacrolimus (Protopic) and Pimecrolimus (Elidel), new kids on the block – Great for facial eczema – $120 for 30gm Topical Immune Modulators and Cancer • Elidel (pimecrolimus 1%) and Protopic (tacrolimus 0.1% and 0.03%) –heavily marketed • 29 cases of cancers in children and adults associated with use of these topicalslymphomas, SCC’s, sarcomas • Causality not proven FDA Response • Black Box Warning Do not use in children under 2 years of age Do not us in adults or children with “weakened” immune systems: Transplants, HIV, cancer patients, etc. • Limit use—no continuous usage; limit area treated Topical Immunomodulators When to use • Eyelid dermatitis • Refractory psoriasis on upper thighs, scrotum, glans penis • Otherwise use cheaper alternatives first – Protopic=TAC 0.1% – Elidel=HC 2.5% Buttock Folliculitis • Mechanical from clothing • Ban roll-on good • Topical antibx qd – Cleocin/Erythro Keratosis Pilaris • Thickening of hair follicles on the out arms and upper legs • Associated with dry skin • Lubrication • Lachydrin 12% lotion bid Intertrigo • • • • • Pendulous breasts or pannus Always component of candida Blow dry area Apply topical antifungals Tucks pads Bacterial Skin Infections • Most common pathogen is staph aureus • More methicillin resistant staph causing skin and soft tissue infections in the community • JAMA-Niami et al Dec 2003 Approach to Treatment • Culture where you can-if you have pus, that is great • Incise and drain when appropriate (Abcesses) If no pus: • Tx with methicillin SENSITIVE drugs-first line but have pt return to evaluate for resolution • If recurrent infection, tx with methicillin RESISTANT antibiotics right off the bat Septra, Doxycycline,Cipro/Levofloxacillin), Clindamycin • Consider adding rifampin 600 qd for 5 days or mupirocin ointment for staph eradication Was it bacterial in the first place? • Remember HSV-culture and/or Direct Fleurescent Antibody • Skin biopsy for histology and tissue culture • Diseases that Masquerade as Infectious Diseases Ann Int Med 2005 Jan 4; 142:47-55 Hidradenitis Supparativa • Not an infectious disease • Disease of apocrine glands • Treatment – – – – – IL Kenalog Minocycline Surgery NOT Antibiotics New Biologics Inflamed Epidermoid Cysts • Antibiotics-USELESS • If just starting to become inflamed and cyst is small( < 1 cm), can try intralesional Kenalog injection but see them back in few days-you can exacerbate the inflammation • INCISE and DRAIN and PACK • 6 weeks later, inspect for residual cyst and excise Recurrent Cellulitis • Recurrent cellulitis knocks out lymph system causing low grade cellulitis and retention hyperkeratosis • Tx. Cellulitis-may need 6 months of tx or more • Tx. Hyperkeratosis-urea crème 40% • Tx. Lymphedema-support stockings with 35mm of pressure or mechanical pumps Venous Insufficiency Ulcer • Compression dressing – Unna boot covered by Coban – this requires a good nursing staff with training and experience – This both provides graded compression AND creates the correct wound environment • Semipermeable dressing (Hydrosorb, Duoderm, etc) • Change dressing weekly • Refer to dermatology if not healing Venous Insufficiency Ulcer • Control Edema – Elevation of leg above heart 2 hours twice daily – Walk, don’t sit – Compression • Diuretics overused and not of benefit unless fluid retention due to central problem is present (CHF, CRF) • Create an appropriate wound environment for healing – Paradigm shift: Ulcers that don’t heal do not have the appropriate biochemical environment to promote healing Complications of Leg Ulcers • Allergic contact dermatitis to applied antibiotics, topical anesthetics • Avoid all topical antibiotics to leg ulcers (except topical metronidazole to prevent odor) • Never apply topical benzocaine, Vitamin E, neomycin, or bacitracin to VI leg ulcer • 64 year old man with psoriasis, hypertension, hypercholesterolemia • 3 months of ulceration of medial aspect of left lower leg • Vascular evaluation confirms venous insufficiency • 3 months of treatment fails to improve ulceration • What is your next step? • Skin Biopsy = Squamous Cell Carcinoma • Chronic phototherapy and prior immunosuppressive treatments may have led to skin cancer • If leg ulcer doesn’t heal with appropriate treatment—refer or biopsy