Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
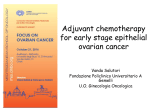
Original Article Does Delay of Adjuvant Chemotherapy Impact Survival in Patients With Resected Stage II and III Colon Adenocarcinoma? Ulas Darda Bayraktar, MD1; Emerson Chen, BA2; Soley Bayraktar, MD1; Laurence R. Sands, MD3; Floriano Marchetti, MD3; Alberto Jose Montero, MD1; and Caio Max S. Rocha-Lima, MD1 BACKGROUND: It is unclear whether delays in commencing adjuvant chemotherapy after surgical resection of colon adenocarcinoma adversely impact survival. METHODS: Patients with stage II-III colon adenocarcinoma who received adjuvant chemotherapy at 2 centers were identified through the institutional tumor registry. Time to adjuvant chemotherapy, overall survival (OS), and relapse-free survival (RFS) were calculated from the day of surgery. Patients were dichotomized into early (time to adjuvant chemotherapy 60 days) and late treatment (time to adjuvant chemotherapy >60 days) groups. OS and RFS were compared using log-rank test and multivariate analysis by the Cox proportional hazards model. RESULTS: Of 186 patients included in the study, 49 (26%) had received adjuvant chemotherapy >60 days after surgical resection. Thirty percent of the delays were system related (eg, late referrals, insurance authorizations). Time to adjuvant chemotherapy >60 days was associated with significantly worse OS in both univariate analysis and a Cox proportional hazards model (hazard ratio, 2.17; 95% confidence interval, 1.08-4.36). Although difference in RFS between the 2 groups favored time to adjuvant chemotherapy <60, this did not reach statistical significance. CONCLUSIONS: Adjuvant chemotherapy delay >60 days after surgical resection of colon cancer is assoC 2010 American Cancer Society. ciated with worse OS. Cancer 2011;117:2364–70. V KEYWORDS: colon cancer, adjuvant chemotherapy, cancer therapy delay, disparity, 5-fluorouracil, oxaliplatin. Adjuvant chemotherapy after surgical resection in stage III colon adenocarcinoma decreases recurrences and improves survival.1 5-Fluorouracil with leucovorin,2,3 5-fluorouracil/leucovorin with oxaliplatin,4,5 and capecitabine monotherapy6 are current standard adjuvant chemotherapy regimens in colon cancer. The role of adjuvant chemotherapy in patients with resected stage II colon cancer remains controversial. However, in the subset of stage II colon cancer patients with high-risk features such as T4 tumors, poor differentiation, perforation, and inadequate number of evaluated lymph nodes, there might be a role for adjuvant chemotherapy.7 Adjuvant chemotherapy is thought to increase cancer cure rates by eradicating micrometastases after surgical resection. Surgery can stimulate angiogenesis and suppress the immune system, leading to tumor growth.8-10 Consequently, it is intuitive that there exists a time-dependent point after surgery where adjuvant chemotherapy would fail to eradicate the micrometastases. In a mathematical model, Harless and Qiu11 proposed that the tumor burden at the time of adjuvant chemotherapy initiation was a function of 4 factors: metastatic load remaining after surgery, intrinsic doubling time of the tumor, relative effectiveness of the immune system in eradicating residual malignant cancer cells, and the time period elapsing before the start of effective chemotherapy. Currently, the latter is the only clinically controllable variable in this equation. Clinical trials for adjuvant chemotherapy in colon cancer generally have required a time interval between surgery and adjuvant chemotherapy initiation of no more than 6 to 8 weeks.1,2,12-14 However, it is unclear from the published literature to what extent the time to initiating adjuvant chemotherapy for colon cancer correlates with patients’ survival. Various analyses of prospective clinical trials and a few retrospective studies have reported conflicting results.13,15-25 It can be postulated from the published studies that delay of adjuvant chemotherapy for >56 to 60 days could have a detrimental effect on survival. However, a major limitation of these studies is that confounding factors such as urgency of the surgical Corresponding author: Ulas D. Bayraktar, MD, Sylvester Comprehensive Cancer Center, 1475 NW 12th Ave St 3300, Miami, FL 33136; Fax: (305) 585-0037; [email protected] 1 Division of Hematology/Oncology, Sylvester Comprehensive Cancer Center, University of Miami, Miami, Florida; 2University of Miami Miller School of Medicine, Miami, Florida; 3Division of Surgical Oncology, Sylvester Comprehensive Cancer Center, University of Miami, Miami, Florida DOI: 10.1002/cncr.25720, Received: June 10, 2010; Revised: August 20, 2010; Accepted: September 24, 2010, Published online December 17, 2010 in Wiley Online Library (wileyonlinelibrary.com) 2364 Cancer June 1, 2011 Colon Cancer Adjuvant Chemotherapy Delay/Bayraktar et al resection, reason for the adjuvant chemotherapy delay, delays during adjuvant chemotherapy, and early adjuvant chemotherapy discontinuation were not incorporated into the analyses. Here, we compared the survival between colon cancer patients who received adjuvant chemotherapy within and after 60 days of surgical resection while controlling for confounding factors. MATERIALS AND METHODS After approval by our institutional review board, we identified patients diagnosed with stage II-III colon adenocarcinoma who received adjuvant chemotherapy after complete surgical resection between January 2000 and December 2008 at Jackson Memorial Hospital (the tertiary-care county hospital in Miami, Fla) and The University of Miami Sylvester Comprehensive Cancer Center (a private academic cancer center), through the institutional tumor registry. Patients with rectal carcinoma, those who received adjuvant chemotherapy >120 days after surgery, and those with <90 days of follow-up were excluded from the study. By using a standardized data collection form, the following data were gathered from the medical records and institutional tumor registry: age, sex, race/ethnicity, marital status, serum creatinine and albumin levels within 2 weeks of surgery, cancer diagnosis (colonoscopy/computerized tomography that first identified the tumor) date, surgical resection date, urgency of the surgical resection, pathology from surgical resection, staging information, follow-up data, and adjuvant chemotherapy data including the type, number of cycles, and dates of first and last doses. Survival data and date of death were obtained from the institutional tumor registry, chart reviews, and social security death index searches. Time to adjuvant chemotherapy and overall survival (OS) were calculated from the surgery date. Relapse-free survival (RFS) was calculated from the surgery date until the date of disease relapse, death, or last follow-up. Reasons for adjuvant chemotherapy delay were classified as 1 of the following: secondary to surgical complications, systemrelated reasons (late referral from outside hospital, late appointments within the hospital, extended time required for insurance authorization), patient-related reasons (missed appointments and extensive time a patient required to decide on adjuvant chemotherapy), or medical reasons (extra time needed for additional tests and tumor board discussions; and extensive discussions between physician and patients). Early discontinuation was defined as cessation of adjuvant chemotherapy before at least 80% of Cancer June 1, 2011 planned adjuvant chemotherapy cycles were delivered unless adjuvant chemotherapy was discontinued because of disease relapse. Delay during adjuvant chemotherapy was defined as adjuvant chemotherapy duration (time between the first and last adjuvant chemotherapy cycle) >25% of the treatment optimal duration. Optimal duration was calculated as: (number of chemotherapy cycles the patient received 1) required interval between each chemotherapy cycle. However, this is not a validated approach and was designed to address the heterogeneity of the number of delivered treatments and the duration of therapy in the adjuvant setting. Urgent surgery was defined as a resection in a patient who presented to an emergency room with bowel obstruction or severe anemia that necessitated an immediate operation. Patients were dichotomized into early (time to adjuvant chemotherapy 60 days) and late (time to adjuvant chemotherapy >60 days) treatment groups. The 2 groups’ demographic and clinical characteristics were compared with 2-sided Student t test and chi-square test. While comparing chemotherapy regimens that include oxaliplatin to those that do not, the patients who received chemotherapy regimens that incorporate irinotecan were excluded from the univariate analysis. Kaplan-Meier survival curves were constructed and compared between subgroups using the log-rank test. To assess the impact of adjuvant chemotherapy delay on survival independent of other confounding variables, a multivariate Cox proportional hazards model was constructed incorporating the significant prognostic factors found in the univariate logrank test. Variables for which data were missing for >10% of the patients were excluded from the model. Second, subgroup analyses were performed using univariate Cox proportional hazards models in the subgroups with prognostic significance identified in the log-rank test. Finally, OS of patients in whom adjuvant chemotherapy was delayed for specific reasons was compared with OS of the patients in the late treatment group using univariate Cox proportional hazards models. Log transformation was used to calculate 95% confidence intervals of survival estimates. A P value <.05 was considered statistically significant. PASW Statistics 17.0 (SPSS Inc., Chicago, Ill) was used for all statistical analyses. RESULTS One hundred eighty-six patients were included in the study. Thirty-eight and 148 patients had stage II and III colon cancer, respectively. Time to adjuvant 2365 Original Article Table 1. Selected Demographic and Clinical Characteristics of Patients in the Early and Late Treatment Groups Characteristics Early Treatment, n5137, No. (%) Late Treatment, n549, No. (%) P Agea Sex ¼ male 55.7 1.1 52 (38) 56.9 1.8 20 (41) .559 .724 20 (15) 80 (58) 37 (27) 13 (26) 24 (49) 12 (25) 27 (20) 73 (53) 36 (26) 1 (1) 0.83 0.02 3.92 0.09 68 (50) 36/124 (29) 25/76 (33) 7 (14) 28 (57) 14 (29) Marital status Single Married Divorced or widow .169 Race White non-Hispanic White Hispanic Black Asian Creatininea Albumina Diagnosed before 2004 Urgent surgery TTS > 30 days .775 0 0.82 0.03 3.87 0.13 18 (37) 20/43 (47) 5/18 (28) T stage 1-2 3 4 Tumor dimensiona Differentiation ¼ poor Margins involved AC at JMH Oxaliplatin included in AC AC early discontinuation Delay during AC .036 .675 .242 20 (15) 110 (82) 5 (4) 5 (10) 40 (82) 4 (8) N stage 0 1 2 .940 .772 .463 25 (18) 64 (47) 48 (35) 4.79 0.23 27/129 (21) 11/116 (10) 72 (53) 64/109 (59) 11/102 (11) 36/105 (34) 13 (26) 21 (43) 15 (31) 4.76 0.37 6/46 (13) 6/42 (14) 32 (65) 30/42 (71) 11 /40 (27) 15/40 (37) .877 .240 .592 .123 .149 .013 .849 TTS indicates time to surgery (from diagnosis date); AC, adjuvant chemotherapy; JMH, Jackson Memorial Hospital. a Mean standard error. chemotherapy ranged between 22 and 118 days (median, 48). Forty-nine (26%) patients received adjuvant chemotherapy >60 days after surgery. Adjuvant chemotherapy was delayed because of system-related factors in 15 (31%), patient-related factors in 10 (20%), medical reasons in 9 (18%), surgical complications in 8 (16%), and unknown reasons in 7 (14%) patients. Demographic and clinical characteristics of the patients in the 2 groups are demonstrated in Table 1. More patients in the late treatment group underwent urgent surgery and discontinued adjuvant chemotherapy early. Of note, in only 3 (5%) of 56 patients who had undergone urgent surgeries, adjuvant chemotherapy was delayed because of surgical complications (wound dehis- 2366 cence and infection). All 159 patients for whom we had the details of adjuvant chemotherapy had received fluoropyrimidine-based chemotherapy. The most frequently used adjuvant chemotherapy regimens were FOL-FOX (n ¼ 64), Mayo Clinic schedule (n ¼ 30), and Roswell-Park schedule (n ¼ 17). In the early treatment group, 27 (20%) patients were followed until death, and 110 patients were alive after a median follow-up of 42.9 months (range, 7.2-112.2 months). In the late treatment group, 14 (29%) patients were followed until death, and 35 patients were alive after a median follow-up of 26.6 months (range, 10.7-80.3 months). Twenty-three (85%) and 9 (64%) deaths in the early and late treatment groups were cancer-related, whereas cause of death could not be identified in 1 and 3 patients in the early and late treatment groups, respectively. The 5-year disease-specific survival in early and late treatment groups was 80.3% and 70.4%. Table 2 demonstrates the 5-year OS and RFS rates in various patient subgroups. Whereas OS was found to be significantly worse in the late treatment group compared with the early treatment group in the univariate analysis (Fig. 1A), the difference in RFS between the 2 groups did not reach statistical significance (Fig. 1B). Other identified prognostic factors for OS in univariate analyses included diagnosis year, urgency of the surgery, T and N stages of the cancer, treating hospital, and whether adjuvant chemotherapy included oxaliplatin (irinotecancontaining regimens were excluded from this comparison). Data for urgency of the surgery and adjuvant chemotherapy type were missing for >10% of patients. The Cox proportional hazards model incorporating age, diagnosis year, T and N stages of the tumor, treating hospital, and adjuvant chemotherapy delay demonstrated time to adjuvant chemotherapy >60 days as a poor prognostic factor for OS (Table 3, right-most column). Subgroup analyses demonstrated that delay of adjuvant chemotherapy >60 days after surgery was associated with numerically worse OS in almost all patient subgroups (Table 3). Perhaps due in part to overall relatively small sample size, the only subgroups where time to adjuvant chemotherapy >60 days was associated with significantly worse OS were the patients treated at Sylvester Comprehensive Cancer Center and those who were diagnosed with colon cancer before 2004. In a small patient cohort, OS was significantly worse in patients whose adjuvant chemotherapy was delayed beyond 60 days because of patient-related factors and unknown reasons than in patients who received Cancer June 1, 2011 Colon Cancer Adjuvant Chemotherapy Delay/Bayraktar et al Table 2. Five-Year OS and RFS Rates in Patient Subgroups Characteristic Value 5-Year RFS, % (95% CI) Pa Age 60 >60 Male Female Single Married DW W, non-Hisp W, Hisp B Before 2004 Beyond 2004 Nonurgent Urgent 30 days >30 days 0 1 2 1-2 3 4 SCCC JMH 60 >60 FP alone FP þ OX No Yes No Yes 64.7 65.9 55.6 70.2 78.2 65.1 59.0 56.3 66.4 70.7 54.3 76.4 73.7 51.3 73.8 76.0 71.7 74.5 49.4 80.6 66.2 29.6 74.9 57.5 67.6 57.6 61.3 73.1 74.7 64.5 68.9 75.1 .673 Sex Marital status Race/ethnicity Diagnosis year Surgical resection TTS N stage T stage Hospital TTC AC type AC early discontinuation Delay during AC (54.7-76.5) (54.5-79.7) (42.0-73.8) (61.3-80.4) (63.9-95.8) (55.0-77.1) (45.1-77.2) (40.2-78.9) (56.1-78.5) (58.2-85.8) (44.1-66.8) (65.4-89.3) (64.8-83.9) (36.5-72.2) (63.1-86.4) (58.7-98.4) (57.0-90.1) (64.1-86.6) (36.7-66.5) (64.6-100.0) (57.8-75.9) (10.0-87.6) (64.7-86.7) (47.0-70.3) (59.2-77.2) (41.5-80.0) (49.4-76.0) (60.9-87.7) (65.9-84.7) (39.7-100.0) (58.7-81.0) (61.6-91.6) HR for RFSb .111 .434 .266 .003 Reference 0.53 (0.30-0.96) .005 .421 .001 <.001 .035 .372 .087 .691 .317 Reference 0.92 (0.40-2.10) 2.53 (1.16-5.52) Reference 1.70 (0.67-4.34) 6.30 (1.83-21.72) Reference 1.51 (0.86-2.64) Reference 1.21 (0.66-2.20) 5-Year OS, % (95% CI) Pa HR for OSb 78.6 66.7 70.9 75.3 88.6 71.0 69.4 67.5 73.7 77.8 65.1 84.8 82.4 61.4 79.4 81.8 82.0 82.3 56.2 83.9 74.4 37.0 81.0 67.5 78.6 56.7 66.7 85.8 83.1 68.9 77.9 76.8 .068 Reference 1.41 (0.74-2.70) (69.8-88.4) (54.6-81.4) (59.0-85.2) (66.2-85.7) (76.8-100.0) (60.6-83.2) (55.8-86.3) (51.5-88.4) (63.9-85.1) (64.1-94.4) (55.0-77.1) (76.1-94.4) (74.3-91.3) (47.5-79.3) (69.0-91.4) (63.8-100.0) (68.5-98.2) (72.3-93.7) (43.0-73.5) (65.8-100.0) (66.5-83.3) (13.8-99.8) (70.4-93.2) (57.6-79.2) (71.0-87.1) (40.0-80.3) (54.8-81.2) (77.2-95.4) (74.9-92.2) (46.0-100.0) (68.5-88.6) (61.8-95.5) .351 .265 .637 .018 Reference 0.47 (0.23-0.99) .021 .288 <.001 .004 .016 .036 Reference 1.10 (0.38-3.13) 3.98 (1.47-10.77) Reference 2.17 (0.65-7.23) 8.20 (1.71-39.21) Reference 2.09 (1.06-4.15) Reference 2.07 (1.02-4.19) .046 .288 .433 OS indicates overall survival; RFS, relapse-free survival; CI, confidence interval; HR, hazard ratio; DW, divorced or widowed; W, white; Hisp, Hispanic; B, black; TTS, time to surgery; SCCC, Sylvester Comprehensive Cancer Center; JMH, Jackson Memorial Hospital; AC, adjuvant chemotherapy; FP, fluoropyrimidine; OX, oxaliplatin. a Derived from univariate comparisons of the survival curves with log-rank test. b Derived from the multivariate Cox proportional hazards model. chemotherapy within 60 days of surgery (Table 4). No significant difference was found between OS of patients in the early treatment group and OS of those in whom adjuvant chemotherapy was delayed because of surgical complications or medical reasons; however, this is likely because of small numbers of patients in these subgroups. DISCUSSION To the best of our knowledge, this is the first study that in addressing whether delays in the initiation of adjuvant chemotherapy adversely impact survival in colon cancer patients, also dissects the contribution of other confounding factors, such as urgency of surgical resection, reason for adjuvant chemotherapy delay, delays during adjuvant chemotherapy, and early adjuvant chemotherapy disconCancer June 1, 2011 tinuation. On univariate analysis and a Cox proportional hazards model, we found that patients who had received adjuvant chemotherapy within 60 days of surgical resection for colon cancer had a better OS than those who began adjuvant chemotherapy >60 days after the resection. Although RFS in the early treatment group was numerically better than RFS in the late treatment group, the difference was not statistically significant. Most of the adjuvant chemotherapy delays in our cohort were system- and patient-related, indicating a mix of intra-/interhospital referral system deficiencies and patient behavior as the primary culprits for the adjuvant chemotherapy delay. Similarly, administrative problems were found to be the most common cause of delay in the treatment of breast cancer in a retrospective study published in 1980.26 2367 Original Article Table 3. HRs for Adjuvant Chemotherapy Delay on Overall Survival in Selected Patient Subgroups Characteristic Subgroup No. HR (95% CI)a Diagnosis year 2000-2003 2004-2009 SCCC JMH 0 1 2 0-2 3 4 Elective Urgent FP alone FP þ OX Adequate Inadequate Not delayed Delayed 86 100 82 104 38 85 63 13 150 9 112 56 57 94 120 22 95 51 2.49 1.67 3.70 1.30 4.86 1.93 1.84 2.89 1.93 0.64 1.52 1.26 2.24 2.12 2.11 0.60 1.33 1.97 Hospital N stage T stage Surgery AC type Number of AC cycles Delay during AC (1.15-5.38) (0.48-5.74) (1.19-11.48) (0.56-2.99) (0.88-26.72) (0.56-6.64) (0.71-4.78) (0.26-32.30) (0.93-4.04) (0.10-3.92) (0.55-4.24) (0.43-3.70) (0.89-5.64) (0.59-7.68) (0.72-6.15) (0.08-4.60) (0.47-3.75) (0.44-8.81) HR indicates hazard ratio; CI, confidence interval; SCCC, Sylvester Comprehensive Cancer Center; JMH, Jackson Memorial Hospital; AC, adjuvant chemotherapy; FP, fluoropyrimidine; OX, oxaliplatin. a Derived from the univariate analyses comparing early and late initiation of adjuvant chemotherapy in the subgroups specified in the first column. Table 4. HRs for Overall Survival in the Late Treatment Group Stratified According to the Reason for Delay of Adjuvant Chemotherapy Reason for Delay No. (%) HR (95% CI)a Early treatment 137 Reference Late treatment 49 (100) System-related reasons Patient-related reasons Medical reasons Surgical complications Unknown 15 10 9 8 7 (31) (20) (18) (16) (14) 1.07 (0.25-4.54) 4.99 (2.03-12.26) No deaths recorded 1.93 (0.58-6.37) 5.45 (1.60-18.60) a Derived from the univariate comparison of the overall survival between the individual subsets of the late treatment group and the early treatment group. Figure 1. Comparison of overall (A) and relapse-free survival (B) between patients in early and late treatment groups is shown (P values are derived from log-rank test). Patients who required urgent surgical resection tended to have delayed adjuvant chemotherapy. This can be partly explained by the higher surgical complication rates after urgent surgeries compared with elective ones.27 However, only 3 patients who had urgent surgeries in our study cohort started adjuvant chemotherapy late because of surgical complications. Equally, lack of insurance coverage and patient behavior in face of sickness may lead to delays in seeking medical care, consequently leading to both urgent operations and late referrals to the oncolo- 2368 gists. Accordingly, Langenbach et al reported that patients with additional insurance had a mean delay of 18 days between the time of initial diagnosis of colorectal cancer and referral to the surgeon, whereas those without additional private insurance had a mean delay of 57 days in Germany.28 Although not statistically significant, we found that married patients were more likely to start adjuvant chemotherapy within 60 days of surgery compared with single patients, coinciding with Hershman et al’s findings.25 We did not find any association between adjuvant chemotherapy delay and race/ethnicity, time to surgery, or significant delays in administering adjuvant chemotherapy once initiated. Cancer June 1, 2011 Colon Cancer Adjuvant Chemotherapy Delay/Bayraktar et al On univariate analysis, we found a significant association between adjuvant chemotherapy delay and OS but not RFS. Similarly, Chau et al20and Czaykowski et al22 also demonstrated worse OS in patients who received adjuvant chemotherapy >8 weeks after surgery but no difference in RFS. This may be because of relatively small numbers of patients in both studies and the confounding variables that may have obscured the difference in RFS between the 2 groups. Another reason for the difference between the impact of delay on OS and RFS may be more cancer-unrelated deaths in patients whose adjuvant chemotherapy is delayed. However, because <15% of deaths were because of cancer-unrelated reasons in both groups (time to adjuvant chemotherapy <60 and time to adjuvant chemotherapy >60), it is unlikely that observed differences are unrelated to treatment or to colon cancer. It is still unclear if the process of delaying administration of adjuvant chemotherapy itself adversely impacts survival. It is possible that other factors, such as surgical complications, patient noncompliance with planned chemotherapy schedule, and system-related factors that lead to delays in adjuvant chemotherapy, may also increase mortality independent of time to adjuvant chemotherapy. However, subgroup and multivariate analyses support the hypothesis that delay in adjuvant chemotherapy worsens survival independent of confounding variables. This study has certain limitations. It is a retrospective study with no control over confounding variables. However, a controlled prospective study on the subject is not feasible for ethical reasons. In addition, a retrospective study is better suited to identify the factors leading to deviation from the optimal care. Second, our study cohort was not large enough for the detailed analysis of delay’s impact on survival, and not all data on chemotherapy were available to us. Consequently, our proportional hazards model was reduced and deprived of important confounding variables such as urgency of surgical resection, which was found to be a prognostic factor on OS and was significantly different between early and late treatment groups. Third, lack of data on patient comorbidities and performance status may have decreased the accuracy of our survival analyses. In summary, delay of adjuvant chemotherapy for >60 days after surgical resection was found to be associated with poor OS in colon cancer patients. More extensive retrospective studies are needed to confirm the impact of adjuvant chemotherapy delay on colon cancer survival independent of confounding factors. Finally, it is possible Cancer June 1, 2011 that disparities in clinical outcomes in colon cancer could be reduced by precisely identifying all major factors that lead to significant delays (>60 days) in initiating adjuvant chemotherapy and devising strategies that are effective in decreasing time to chemotherapy. CONFLICT OF INTEREST DISCLOSURES We would like to thank Miami Tumor Registry for providing the list of patients. REFERENCES 1. Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med. 1990;322:352-358. 2. Wolmark N, Rockette H, Fisher B, et al. The benefit of leucovorin-modulated fluorouracil as postoperative adjuvant therapy for primary colon cancer: results from National Surgical Adjuvant Breast and Bowel Project protocol C-03. J Clin Oncol. 1993;11:1879-1887. 3. O’Connell MJ, Mailliard JA, Kahn MJ, et al.Controlled trial of fluorouracil and low-dose leucovorin given for 6 months as postoperative adjuvant therapy for colon cancer. J Clin Oncol. 1997;15:246-250. 4. Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350:2343-2351. 5. Wolmark N, Wieand, S, Kuebler, PJ. A phase III trial comparing FULV to FULV þ oxaliplatin in stage II or III carcinoma of the colon: survival results of NSABP Protocol C07. J Clin Oncol. 2008;26:1008s. 6. Twelves C, Wong A, Nowacki MP, et al. Capecitabine as adjuvant treatment for stage III colon cancer. N Engl J Med. 2005;352:2696-2704. 7. Benson AB III, Schrag D, Somerfield MR, et al. American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol. 2004; 22:3408-3419. 8. Baum M, Demicheli R, Hrushesky W, Retsky M. Does surgery unfavourably perturb the ‘‘natural history’’ of early breast cancer by accelerating the appearance of distant metastases? Eur J Cancer. 2005;41:508-515. 9. Fisher B, Gunduz N, Coyle J, Rudock C, Saffer E. Presence of a growth-stimulating factor in serum following primary tumor removal in mice. Cancer Res. 1989;49:1996-2001. 10. Hensler T, Hecker H, Heeg K, et al. Distinct mechanisms of immunosuppression as a consequence of major surgery. Infect Immun. 1997;65:2283-2291. 11. Harless W, Qiu Y. Cancer: a medical emergency. Med Hypotheses. 2006;67:1054-1059. 12. Laurie JA, Moertel CG, Fleming TR, et al. Surgical adjuvant therapy of large-bowel carcinoma: an evaluation of levamisole and the combination of levamisole and fluorouracil. The North Central Cancer Treatment Group and the Mayo Clinic. J Clin Oncol. 1989;7:1447-1456. 13. Taal BG, Van Tinteren H, Zoetmulder FA. Adjuvant 5FU plus levamisole in colonic or rectal cancer: improved survival in stage II and III. Br J Cancer. 2001;85:1437-1443. 14. O’Connell MJ, Laurie JA, Kahn M, et al. Prospectively randomized trial of postoperative adjuvant chemotherapy in 2369 Original Article 15. 16. 17. 18. 19. 20. patients with high-risk colon cancer. J Clin Oncol. 1998; 16:295-300. Moertel CG, Fleming TR, Macdonald JS, et al. Intergroup study of fluorouracil plus levamisole as adjuvant therapy for stage II/Dukes’ B2 colon cancer. J Clin Oncol. 1995;13: 2936-2943. Andre T, Colin P, Louvet C, et al. Semimonthly versus monthly regimen of fluorouracil and leucovorin administered for 24 or 36 weeks as adjuvant therapy in stage II and III colon cancer: results of a randomized trial. J Clin Oncol. 2003;21:2896-2903. Arkenau HT, Bermann A, Rettig K, Strohmeyer G, Porschen R. 5-Fluorouracil plus leucovorin is an effective adjuvant chemotherapy in curatively resected stage III colon cancer: long-term follow-up results of the adjCCA-01 trial. Ann Oncol. 2003;14:395-399. Glimelius B, Dahl O, Cedermark B, et al. Adjuvant chemotherapy in colorectal cancer: a joint analysis of randomised trials by the Nordic Gastrointestinal Tumour Adjuvant Therapy Group. Acta Oncol. 2005;44:904-912. Berglund A, Cedermark B, Glimelius B. Is it deleterious to delay the start of adjuvant chemotherapy in colon cancer stage III? Ann Oncol. 2008;19:400-402. Chau I, Norman AR, Cunningham D, et al. A randomised comparison between 6 months of bolus fluorouracil/leucovorin and 12 weeks of protracted venous infusion fluorouracil as adjuvant treatment in colorectal cancer. Ann Oncol. 2005; 16:549-557. 2370 21. Biagi JJ, Barnes C, O’Callaghan CJ. Time to adjuvant chemotherapy in colorectal cancer. Paper presented at: 2007 Gastrointestinal Cancers Symposium, Orlando, FL, January 19, 2001. 22. Czaykowski P, Gill S, Kennecke H, Turner D, Gordon V. Adjuvant chemotherapy (AC) for stage 3 colon cancer: does timing matter? Paper presented at: 2007 Gastrointestinal Cancers Symposium, Orlando, FL, January 19, 2001. 23. Ahmad I, Anan G, Alvi R. Impact of timing of initiation of adjuvant chemotherapy on survival after resection of colorectal cancer. J Clin Oncol. 2007;25(18 suppl):4054. 24. Carlsson G, Albertsson P, Gustavsson B. Delayed start of adjuvant 5-FU/leucovorin based chemotherapy in colon cancer is safe up to 12 weeks postoperatively. J Clin Oncol. 2007;25(18 suppl):4056. 25. Hershman D, Hall MJ, Wang X, et al. Timing of adjuvant chemotherapy initiation after surgery for stage III colon cancer. Cancer. 2006;107:2581-2588. 26. Adam SA, Horner JK, Vessey MP. Delay in treatment for breast cancer. Community Med. 1980;2:195-201. 27. Kim J, Mittal R, Konyalian V, King J, Stamos MJ, Kumar RR. Outcome analysis of patients undergoing colorectal resection for emergent and elective indications. Am Surg. 2007;73:991-993. 28. Langenbach MR, Schmidt J, Neumann J, Zirngibl H. Delay in treatment of colorectal cancer: multifactorial problem. World J Surg. 2003;27:304-308. Cancer June 1, 2011