Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
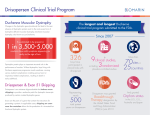
Nov 22, 2016 Sandra Chan Allen Chiu Joseph Correia Tam Myngoc Nguyen X-Linked Muscular Dystrophies: Duchenne’s Disorder PHM142 Fall 2016 Instructor: Dr. Jeffrey Henderson X-linked Muscular Dystrophies • X-linked recessive disorders: affect mostly males • Genetic conditions that cause muscle weakness and eventually atrophy • Effect skeletal and cardiac muscle X-linked Muscular Dystrophies Types: • X-linked Emery-Dreifuss (EDMD): FHL1 gene • Joint rigidity, atrophy of scapuloperoneal muscles, cardiovascular effects • Duchenne: DMD gene • Becker: DMD gene • Later onset, less severe, slower progression Duchenne Muscular Dystrophy • Motor symptoms: • Delayed motor skills • Gait abnormalities • Frequent falling • Difficulty standing up • Muscle weakness starting from the lower limbs • Raised creatine kinase levels • Scoliosis • Dilated cardiomyopathy in adolescence Duchenne Muscular Dystrophy • Associated risks: • Language and developmental delays • Lower IQ • Risk of ADHD, Autism • Restrictive lung disease Duchenne Muscular Dystrophy • Incidence: 1 in 5000 boys • Cause: mutation in DMD gene • DMD a large gene that codes for dystrophin protein • Dystrophin: in the sarcolemma of muscle Dystrophin Structure • hydrophilic1 • rod shaped • 4 domains • N-terminal actin-binding domain • C terminal complex-binding domain • Central triple-helical rod domain • Cysteine-rich domain Function • Integral part of Dystrophin associated protein complex (DAPC)2 • Protein complex attaches cytoskeletal actin to ECM to maintain muscle integrity/tensile strength • Protection of sarcolemma (ex. shock absorption) • Cell signaling (ex. docking site) Mechanism Mechanism ECM DAPC Receptor Dystrophin Actin Sarcolemma Mechanism ECM DAPC Receptor nNOS Actin Sarcolemma Mechanism ECM Ach DAPC Receptor nNOS Actin V-gated channels on SR (Ca2+ in) Sarcolemma Mechanism ECM Ach DAPC Receptor nNOS Actin V-gated channels on SR (Ca2+ in) Calcium binding to troponin Sarcolemma Mechanism ECM Ach Sarcolemma DAPC Receptor nNOS Actin V-gated channels on SR (Ca2+ in) Calcium binding to troponin Actin and myosin interaction Mechanism ECM Ach Sarcolemma DAPC Receptor nNOS Actin Creatine Kinase + V-gated channels on SR (Ca2+ in) Calcium binding to troponin Actin and myosin interaction ATP ADP Power Stroke Mechanism Ach Sarcolemma Receptor Creatine Kinase + V-gated channels on SR (Ca2+ in) Calcium binding to troponin Actin and myosin interaction ATP ADP Power Stroke Mechanism Ach Sarcolemma Receptor Creatine Kinase + V-gated channels on SR (Ca2+ in) Calcium binding to troponin Actin and myosin interaction ATP ADP Power X Stroke Mechanism Ach Ca2+ Sarcolemma Receptor Ca2+ Dependent Proteases - V-gated channels on SR (Ca2+ in) Calcium binding to troponin Creatine Kinase + Actin and myosin interaction X ATP ADP Power X Stroke Mechanism Mechanical damage to membrane • Protein leakage (ex. CK) 3 • Calcium leaks in disturb electrochemical gradient + proteolysis Disturbances in signal transduction • Nitric oxide synthase (nNOS) is associated with dystrophin (via spectrin repeats)4 • NO oxide production activates heme-containing proteins • Proteins regulate muscle contraction, glucose metabolism, and calcium dynamics • Dilates blood vessels Diagnosis of DMD • DMD should be suspected in patients with: • Family history of DMD: any abnormal muscle function • No family history: Gower’s sign, delayed walking (>16-18 months), frequent falls • Increased transaminases • Blood Sample: • Creatine kinase concentrations increased • Muscle Biopsy: • Lack of dystrophin expression • Genetic Tests Types of Genetic Testing • Multiplex Ligation-Dependent Probe Amplification (MLPA) • Modified PCR • Can detect exon deletion or duplications • Most cost effective • Direct Sequencing of Gene • Used to detect small mutations if MLPA unsuccessful • May be more cost efficient in the future Source: Bushby et al., (2010) Treatment • No cure available • Treatment focuses on managing the progression of symptoms i) Drug Therapy ii) Physical Therapy iii) Novel Therapies Drug Therapy (Corticosteroid Therapy) • Improve muscle strength, prolong ambulation, reduce decline of cardiorespiratory function, reduce risk of scoliosis, improve life expectancy • Most common are prednisone and prednisolone Prednisone • Mechanism of action is unclear • Initiation of Treatment: between plateau of motor skill development and decline of motor skills (e.g. 4-6 years of age) • Duration of Treatment: Continue even after loss of ambulation to delay symptoms • Side Effects: weight gain, high BP, behavioural changes, delayed growth • Deflazacort Physical Therapy • Promotes mobility and prevents contractures • Stretching (e.g. Achilles tendon, hip flexors) • Surgery may be necessary • Use of braces, splints or wheelchairs Novel Therapies • Gene therapy, stem cell therapy, dystrophin restoration • E.g. Stop Codon Suppression Agents (i.e. Ataluren): ribosome reads through stop codons, allowing for the full translation and production of functional protein • Only works for patients with nonsense mutations in gene • E.g. Exon skipping: allows exons to be omitted to restore dystrophin reading frame • At pre-mRNA level • ~13% of DMD patients have mutations that can be corrected by skipping exon 51 • Challenges: clinical trial design, systemic delivery, safety/tolerability, host immune responses Summary Slide • DMD is an X-linked recessive disorder that causes muscle weakness/atrophy in skeletal and cardiac muscle • Lack of dystrophin expression results in membrane damage causing protein leakage, calcium influx and disturbances in cellular signalling • These processes result in muscle atrophy and eventually cell death • A variety of physical, blood, and tissue testing is available for DMD; however, genetic testing is needed for definitive diagnosis • Multiplex Ligation-Dependent Probe Amplification (MLPA) is the most common and most cost effective method to determine type and location of mutation. • No cure available • Treatment focuses on managing the progression of symptoms • Drug Therapy: Prednisone, Prednisolone, Deflazacort • Physical Therapy: Stretching, Surgery, Assistive Devices (E.g. splints, wheelchairs) • Novel Therapies: Stop Codon Suppression Agents (e.g. Ataluren), Exon Skipping References 1) "The DMD Mutations Database." The dystrophin associated complex, . Accessed 19 Nov. 2016. www.umd.be/DMD/W_DMD/protein.html 2) Goldstein, Jeffery A., and Elizabeth M. McNally. "Mechanisms of muscle weakness in muscular dystrophy." The Journal of General Physiology, vol. 136, no. 1, 2008, pp. 29-34. 3) Rahimov, Fedik, and Louis M. Kunkel. "Cellular and molecular mechanisms underlying muscular dystrophy." The Journal of Cell Biology, vol. 201, no. 4, 2013, pp. 499-510. 4) Guiraud, Simon, Annemieke Aartsma-Rus, Natassia M. Vieira, Kay E. Davies, and Gert-Jan B. Ommen. "The pathogenesis and therapy of muscular dystrophies." Genomics and Human Genetics, vol. 16, 2015, pp. 281308. 5) Yiu, Eppie M., and Andrew J. Kornberg. "Duchenne muscular dystrophy." Neurology India 56.3 (2008): 236. 6) Ziat, Esma, and Anne T. Bertrand. "FHL1 protein isoforms in Emery-Dreifuss muscular dystrophy." Orphanet Journal of Rare Diseases 10.2 (2015): 1. 7) Duchenne and Becker muscular dystrophy: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2016 Nov 15. Duchenne and Becker muscular dystrophy; [reviewed 2016 June; cited 2016 Nov 20]; [about 3 screens]. Available from: https://ghr.nlm.nih.gov/condition/duchenne-and-becker-muscular-dystrophy References 8) Abbs, S., Tuffery-Giraud, S., Bakker, E., Ferlini, A., Sejersen, T., & Mueller, C. R. (2010). Best practice guidelines on molecular diagnostics in Duchenne/Becker muscular dystrophies. Neuromuscular Disorders, 20(6), 422-427. 9) Bushby, K., Finkel, R., Birnkrant, D. J., Case, L. E., Clemens, P. R., Cripe, L., ... & Poysky, J. (2010). Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. The Lancet Neurology, 9(1), 77-93. 10) Falzarano, M. S., Scotton, C., Passarelli, C., & Ferlini, A. (2015). Duchenne muscular dystrophy: from diagnosis to therapy. Molecules, 20(10), 18168-18184. 11)Young, Courtney S., and April D. Pyle. "Exon Skipping Therapy." Cell 167.5 (2016): 1144. 12) Angelini, Corrado, and Enrico Peterle. "Old and new therapeutic developments in steroid treatment in Duchenne muscular dystrophy." Acta Myol 31.1 (2012): 9-15. 13) Merlini, Luciano, et al. "Early prednisone treatment in Duchenne muscular dystrophy." Muscle & nerve 27.2 (2003): 222-227.