Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
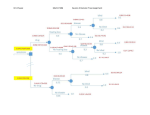
PROJECT REPORT Candidate Number: 490196 MSc CEH Title: Magnitude and Causes of Childhood Blindness and Severe Visual Impairment in Sekoru District of Jimma Zone, South West Ethiopia: The Key Informant Method. Supervisor: Dr Anthony Solomon Word Count: 8,238 Project Length: Standard Submitted in part fulfilment of the requirements for the degree of MSc in CEH For Academic Year 2008-2009 Acknowledgement: I would like to say thank you so much to my supervisor Dr Anthony Solomon for his immeasurable support and advise he has been giving to me starting from the first day I met him. This project work would have not been completed without his continued assistance and support. I would like to extend my thanks and deep appreciation for Dr Daksha Patel, our course director and clinical lecturer, for her support at different times in the course of this project work. I am very thankful for ORBIS UK for sponsoring me to study this MSc in Community Eye Health course at the renowned LSHTM and also funding the summer project work and the forthcoming alumni workshop. My thanks and gratitude also extend to JJ/WBGSP (Joint Japan/World Bank Graduate Study Program) who co-sponsored me to study this masters course at LSHTM, University of London. I would like to thank the School Trust Fund for covering the cost of round trip flight ticket to Ethiopia for this project work. I am also very grateful to all participants of the research and those who supported me in the study in Sekoru district, Jimma zone, Ethiopia. Finally, I would like to thank all the staffs at ICEH (International Centre for Eye Health) and lecturers from other Universities who delivered and thought us these state-of-the-art lectures in community eye health without reservations. 2 Contents: Page Acknowledgements ………………………………….…....……...………………......…2 Table of contents………………………………………..…………..…...…….…..…….3 Abbreviations....................................................................................................…...5 List of tables and figures……………………………………..……...…….….…...…….6 Abstract ……………………………………………………………........…....….…..…...7 1. Introduction ………………………………………………………......…....……..…...8 1.1 Background………………………………………………………............…..……..8 1.2 Literature review……………………………………………….…….............……..8 1.2.1 Definitions……………………………………………………................……8 1.2.2 Magnitude of visual impairment worldwide………………................……9 1.2.3 Magnitude and causes of blindness worldwide…………...............…….10 1.2.4 Epidemiology of childhood blindness……………………..........……....…11 1.2.4.1 Childhood blindness worldwide………………………............….......…..11 1.2.4.2 Childhood blindness in Africa ……………………….................…....…..12 1.2.4.3 Ethiopia.................................................................................................13 1.3 1.2.4.3.1 Country profile.............................................................................13 1.2.4.3.2 Health coverage..........................................................................13 1.2.4.3.3 Eye care in Ethiopia....................................................................14 1.2.4.3.4 Magnitude of visual impairment in Ethiopia.................................14 1.2.4.3.5 Childhood blindness in Ethiopia..................................................15 1.2.4.3.6 VISION 2020 and Ethiopia..........................................................16 1.2.4.3.7 Partners in eye care in Ethiopia......………………....……..…......16 Rationale …………………………………………………….......…..….……...….17 2. Aim and objectives of the study…………………………………...…....………......18 3. Methodology………………………………………………………......…………...…19 3.1 Study design, subjects and study area………………………….....…….……...19 3.2 Ethical approval………………………………………………….........….….….…19 3.3 Sample size calculation...............................................................................….20 3.4 Selection criteria………………………………………………….........…..…..…..20 3.5 Selection of key informants………………………………………........…...….…20 3.6 Training of key informants................................................................................21 3.7 Data collection……………………………………………………................….…..22 3.8 Examination of identified children by Key Informants.......................................22 3.9 Data entry and analysis………………………………………….........…...…..…..24 3 page 4. Results……………………………………………………….………....….….……. 25 5. Discussions…………………………………………………………....…....……….30 6. Conclusions………………………………………………………….......….….……36 7. Recommendation……………………………………………………......…....……..37 8. References.........................................................................................................38 9. Appendices ………………......………………………………………...............……41 4 Abbreviations: AMD -Age-related Macular Degeneration CBM -Christian Blind Mission CHA -Community Health Agents CBRHA -Community Based Reproductive Health Agents EPI -Expanded Program of Immunization IAPB -International Agency for the Prevention of Blindness ICD-10 -International Statistical Classification of Diseases and Related Health Problems, 10th revision IMR -Infant Mortality Rate KI -Key Informant KIM -Key Informant Method logMAR -Logarithm of Minimum Angle of Resolution LP -Light Perception LSHTM -London School of Hygiene & Tropical Medicine NCPB -National Committee for the Prevention of Blindness NLP -No Light Perception ORBIS -ORBIS International, Inc. PA -Peasant Association RE -Refractive Error SVI -Severe Visual Impairment U5MR -Under Five Mortality Rate UNICEF -United Nations Children’s Fund VA -Visual Acuity VAD -Vitamin A Deficiency VI -Visual Impairment WHO -World Health Organisation WHO/PBL -WHO Prevention of Blindness 5 List of tables and figures: Tables: Table 1. Category of blindness and low vision (visual impairment) Table 2. Magnitude of visual impairment worldwide, 2004 Table 3. Association between level of income and prevalence of childhood blindness. Table 4. Summary of field activities at Sekoru district. Table 5. Key informants trained and number of blind/SVI children identified Table 6. Age & sex characteristics of blind/SVI children identified Table 7. Anatomical causes of blindness/SVI Table 8. Proportion of identified children who were blind and SVI. Table 9. Causes of blindness/SVI by age group. Table 10. Aetiological classification of causes of blindness/SVI. Figures: Figure 1. Magnitude and Causes of blindness globally, 2004. Figure 2. Map of Ethiopia Figure 3. Causes of visual impairment (blindness and low vision) in Ethiopia. Figure 4. Map of the study area (Sekoru district): Figure 5. Flow diagram of children identified by KIs as blind/SVI. Figure 6. Aetiological classification of causes of childhood blindness/SVI at Sekoru district. Figure 7. Proportion of avoidable/unavoidable causes of blindness/SVI and reversible/irreversible vision loss at Sekoru district, Ethiopia 6 Abstract: Background/Aim: Most studies on childhood blindness in sub-Saharan African countries have been performed in schools for the blind. As in many countries, there are no populationbased data on childhood blindness in Ethiopia. The overall aim of this study was to determine the magnitude and causes of childhood blindness/severe visual impairment (SVI) using the key informant (KI) method in Sekoru district, Jimma zone, Ethiopia. Methodology: A population-based cross-sectional survey was performed in Sekoru district, Jimma zone, Ethiopia in June and July 2009. We selected 42 KIs and trained them to identify blind/SVI children aged <16 years. Identified children were examined by the candidate, an ophthalmologist. Causes of blindness/SVI were identified and the prevalence of childhood blindness was estimated. Results: The KIs identified 112 children of whom 36 (32%) were blind/SVI. Twenty (56%) were male and 16 (44%) female. Mean age was 10.7 years. The district prevalence of childhood blindness/SVI was 0.062% (95% CI 0.042-0.082). The anatomical causes of blindness/SVI were lens-related in 33% (12 cases), cornea in 28% (10 cases), whole globe [glaucoma in 11% (4 cases) and phthisis bulbi in 8% (3 cases)], refractive error in 17% (6 cases) and optic nerve in 3% (1 case). Avoidable causes of blindness accounted for 89% of cases. Conclusion: The majority of childhood blindness/SVI in Sekoru district is avoidable. Lensrelated abnormalities (mainly congenital cataract) were the commonest causes of childhood blindness/SVI in Sekoru district. A paediatric ophthalmic surgical set-up is required in the region. Key words: Childhood blindness, Ethiopia, key informant, Sekoru district, visual impairment. 7 1. Introduction: 1.1 Background: According to the new global estimates by the World Health Organization (WHO), there are approximately 314 million people around the world whose vision is impaired, due either to eye diseases or uncorrected refractive errors. Of this number, forty-five million are blind (about thirty-seven million from eye diseases and eight million from uncorrected refractive errors). Ninety percent of these blind people live in developing world where blindness remains one of the major public health problems. Women are at higher risk of blindness than men and they constitute at least sixty percent of the blindness worldwide.1-3 Globally, up to seventy-five percent of all blindness in adults is avoidable (either preventable or treatable). In developing countries this number could be as high as ninety percent. The causes of blindness worldwide are variable and differ from one continent to another and between countries depending on access to and availability of health facilities and socioeconomic status. But generally common causes of blindness include cataract, uncorrected refractive errors, glaucoma, age-related macular degeneration, and corneal opacity (mainly from trachoma and onchocerciasis).1 Childhood blindness is one of the five ocular conditions established as immediate priorities for control by the collaboration between the International Agency for the Prevention of Blindness (IAPB) and WHO that is known as VISION 2020: The Right to Sight. VISION 20202 is the global initiative for the elimination of avoidable blindness by the year 2020. Unlike in adults, only about fifty percent of all childhood blindness is avoidable.4 The major preventable causes include vitamin A deficiency, measles, trachoma, harmful traditional eye medicines and ophthalmia neonatorum. Cataract, glaucoma and retinopathy of prematurity are common surgically treatable causes of childhood blindness. The VISION 2020 initiative aims to reduce the prevalence of blindness in children from the present 0.75 per 1000 children to 0.40 per 1000 children by the year 2020.5 1.2 Literature Review: 1.2.1 Definitions: According to the UNICEF definition, a child is defined as an individual whose age is less than 16 years. According to WHO, blindness is defined as best corrected vision of less than 3/60 in the better eye or a visual field no greater than 10° in radius around central fixation.6 Low vision is defined as visual acuity of less than 6/18 but equal to or better than 3/60 or a corresponding visual field loss to less than 200 in the better eye with best possible correction. 8 Visual impairment (VI) includes both blindness and low vision. Severe visual impairment (SVI) is defined as best corrected visual acuity worse than 6/60 but better or equal to 3/60 in the better eye. Based on recommendations from WHO study group on the prevention of blindness, 7 visual impairment has been divided into six strata by the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10).8 (See table 1) Table 1. Category of blindness and low vision (visual impairment)7 Visual acuity with best possible correction Category of Maximum less than: Minimum equal to or better than 1 6/18 6/60 2 6/60 3/60 3 3/60 1/60 4 1/60 Light perception (LP) Blindness Low vision VI 5 No light perception (NLP) 9 Undetermined or unspecified 1.2.2 Magnitude of visual impairment worldwide The new global estimate of visual impairment (reported in a 2006 WHO press release) was based on presenting vision rather than best corrected vision.1, 2 According to the revised ICD-10 categories and definition of VI formulated in Geneva in 2003, blindness is defined as presenting vision of less than 3/60 or a visual field of the better eye no greater than 10° in radius around central fixation.9 Based on this definition there are 314 million people with VI globally.2 The new definition has helped considerably in estimating the extent of VI resulting from uncorrected refractive errors (table 2). 9 Table 2. Magnitude of visual impairment worldwide, 2004* Number in millions Category of VI RE (uncorrected) All other causes Total Low vision 145 124 269 (85.7%) Blindness 8 37 45 (14.3%) 153 (48.7%) 161 (51.3%) 314 (100%) Total *Adapted from Resnikoff 2008 1 In 2002 estimates, the number of visual impairment people was put at 161 million. The newer estimates nearly double this with the addition of 153 million cases of uncorrected RE of whom 8 million are thought to be blind. The new estimate also shows that RE is the commonest cause of visual impairment and the second commonest cause of blindness globally.1, 2 1.2.3 Magnitude and Causes of blindness worldwide: Globally there are 45 million people who are blind. Cataract is the commonest cause of blindness accounting for 39.1% of cases, followed by uncorrected RE at 18.2% and glaucoma 10.1%. Ninety percent of blind people in the world live in developing countries. 1, 10 Childhood blindness accounts for 3.2% of the burden of blindness worldwide which means there are about 1.44 million blind children (figure 1). Cataract 39.1 RE 18.2 Glaucoma 10.1 AMD 7.1 Corneal opacities 4.2 DR 3.9 Childhood blindness 3.2 Trachoma 2.9 Onchocerciasis 0.7 Others 10.6 0 5 10 15 20 25 30 35 Percent Figure 1. Magnitude and Causes of blindness globally, 2004. 10 40 45 1.2.4 Epidemiology of childhood blindness: 1.2.4.1 -Childhood Blindness worldwide: It is estimated that there are about 1.4 million blind children in the world and the prevalence of childhood blindness ranges from 0.3/1000 children age less than 16 years in the wealthiest countries up to 1.5/1000 children in very poor countries. This makes the overall prevalence of childhood blindness 0.75 per one thousand children.10, 11 Worldwide, about half a million children become blind each year, nearly one per minute. Most of this blindness occurs in children living in the sub Saharan and Asian countries. Many of these children die in their childhood from the underlying causes of blindness such as measles, VAD, meningitis, rubella, prematurity, genetic diseases and head injuries.10, 12 Childhood blindness accounts for only 3.2 percent of the burden of global blindness. 1, 13 Compared to the total number of people who are blind worldwide which is about 45 million, the number of blind children in the world seems small. Nevertheless, childhood blindness is one of the initial five priority areas of the IAPB/WHO VISION 2020, the Right to Sight initiative, a global campaign for the elimination of avoidable blindness by the year 2020.10 A number of reasons can be offered for prioritising blindness in childhood despite its relatively small contribution to the overall global prevalence. First, assuming they survive, blind children have many more years of blindness ahead of them than do blind adults, with an estimated 75 million blind-years (number blind x length of life) in total.12 Second, as already indicated, many of the causes of blindness in children are associated with deaths in childhood. Over 50% of children who are blind in developing countries die within 1-2 years of becoming blind.14, 15 Third, the causes of blindness in children differ from those in adults; as a result different strategies and control measures are needed. Fourth, blindness in children has to be treated as soon as diagnosis is made because irreversible loss of vision may occur from amblyopia if this is not done : this is not the case in blindness that commences in adult life. Failure of normal visual maturation during childhood cannot be corrected in adult life, thus there is an element of urgency in treating blindness in children. Fifth, about 50% of causes of blindness in children are as a result of avoidable causes mainly cataract and VAD which can be either treated or prevented with proper eye care services.4 Causes of childhood blindness: There are two ways of classifying the causes of blindness in children: anatomical and aetiological. The anatomical way of classification depends on the most affected part of the eye and is useful as information can be collected on all children. The aetiological 11 classification on the other hand is useful for planning preventive measures in large scale in a population but obtaining reliable data is more difficult.10 Causes of blindness in children vary from region to region depending on the socioeconomic development of countries. In the poor countries of Africa and Asia corneal scarring (mainly from VAD), cataract and glaucoma are the major causes of childhood blindness. But in affluent countries genetic eye diseases, ocular anomalies and CNS lesions are the predominant causes of childhood blindness.15 1.2.4.2 -Childhood blindness in Africa: The poorest regions of Africa and Asia are where three quarters of the world's blind children live.14 Out of the 1.4 million blind children globally, about 300,000 live in Africa.12 The prevalence of blindness in children in a country is related to the nutritional, health and socioeconomic status of that country and hence the under 5 mortality rate (U5MR). It is estimated that countries with U5MR in excess of 170/1000 have a prevalence of childhood blindness in excess of 0.1%, while those with U5MR below 30/1000 probably have a prevalence of 0.02-0.05% children.4, 16-19 Prevalence of blindness can also be estimated depending on the socioeconomic status and level of development of countries. Those very poor countries have the highest prevalence of childhood blindness while affluent countries have the lowest prevalence (table 3).20 Table 3. Association between country’s level of income and development and prevalence of childhood blindness.20 Level of income Very low Low Middle High Prevalence of childhood blindness per 1000 children 1.2 0.9 0.6 0.3 The difference in prevalence of childhood blindness between the richest and the poorest countries of the world may be as high as ten-folds (0.1/1000 versus 1.1/1000).21 Besides lack of adequate data on the extent of childhood blindness in African countries, most studies that have been performed have not been community-based but generally performed solely or principally within schools for the blind. These studies therefore may not reflect the true causes and magnitude of childhood blindness in the region as they are prone to different systematic error. Short of that, these studies have until now been the most useful means of estimating magnitude and causes of childhood blindness. According to studies 12 made at different countries in schools for the blind, majority of blindness in children in Africa are due to avoidable causes.22-24 1.2.4.3 - Ethiopia: 1.2.4.3.1 Country profile: Ethiopia is a developing country located in the Eastern Africa. It is a highland complex of mountains and plateaus divided by the Great Rift Valley. It is a land-locked country with a total surface area of 1,127,127 km². It is bordered by Sudan to the West, Kenya to the South, Somalia to the East, Eritrea to the North and Djibouti to the Northeast. It has three climatic zones: the cool zone, the temperate zone and the hot zone. Ethiopia has a population of 73.9 million people with various cultural, religious and ethnicity origins. Eighty five percent of its population live in rural areas and 45% of the population is consisting of children under the age of 15 years. It has an adult literacy rate of 41.5%.25, 26 Figure 2. Map of Ethiopia 1.2.4.3.2 Health coverage: Health care services in Ethiopia are very limited and generally of poor quality. Health coverage is estimated to be only about 43% according to a report in the year 2005. 27 Utilization of the available health services is also low, hospital admission rate is 1.5%, antenatal care follow up is 32%, attended delivery is only 12%, measles immunisation coverage ranges from 54.3% to 65%, under-five mortality rate (U5MR) is 119 per 1000 children and infant mortality rate (IMR) is 75 per 1000 live births.27-29 13 1.2.4.3.3 Eye care in Ethiopia: As is true in most sub-Saharan African countries there is no adequate eye care service delivery system in Ethiopia. Many reasons can be given for this. The country lacks sufficient number of skilled eye care professionals at all levels of hierarchy and service delivery. The number of eye care professionals is very limited and inadequate for the large population of Ethiopia. To make things worse the available eye care professionals are unevenly distributed in the country being concentrated in the main cities. For example of the 100 ophthalmologists in the country, 60% (60) live and work in the capital city Addis Ababa serving only the 2.7 million inhabitants of the capital city. This leaves the 71 million people living out of Addis Ababa (where majority of the blind is also residing) to be served by only 40 ophthalmologists. The proportion of ophthalmologists to population ratio is therefore about 1 to 1.8 million in rural areas and 1 to 45,000 in the capital. Of the 100 ophthalmologists in the country six have been trained in community eye health, another six have been trained in cornea and external eye diseases, four are paediatric ophthalmologists, three are glaucoma specialists, four are retina specialists and one has training in oculoplastics. The rest are general ophthalmologists. In comparison to the country’s population, the number of eye care personnel is so small as there are few training centres for eye care professionals in the country. Until recently there was only one training centre for ophthalmologists (Addis Ababa University) which graduates only 4 to 5 ophthalmologists each year. For the last 3 years Jimma University has started training ophthalmologists as well as cataract surgeons. Recently there has been some progress in this regard, in that training centres for cataract surgeons, ophthalmic officers, optometrists and ophthalmic nurses are opening in different areas in the country. The cataract surgical rate for Ethiopia is only 357 per million population per year, far behind WHO recommendations for the region.30 1.2.4.3.4 Magnitude of visual impairment in Ethiopia: Ethiopia has one of the highest prevalences of blindness in the world. The national blindness survey which was conducted in 2006 revealed that the prevalence of blindness in the country was 1.6%.31 There are about 1.2 million blind people in the country which means that Ethiopia alone contributes for 2.7% of the total blindness worldwide. The prevalence of low vision (presenting vision less than 6/18 but equal to or better than 3/60 in the better eye) is also high at 3.7%. The causes of blindness are as follows: cataract accounts for 49.9% of the blindness followed by corneal opacity (mainly trachomatous) 19.3%, refractive error 7.8%, glaucoma 5.2%, and macular degeneration 4.8%. The three commonest causes of low vision as shown 14 in figure 3 below are cataract accounting for 42.3%, refractive error 33.4% and corneal opacity 13.6%. % 49.9 50 45 42.3 40 33.4 35 30 25 20 15 10 19.3 13.6 Blindness 13 7.8 5.2 5 4.8 4.6 6.1 Low vision 0 0 Figure 3. Causes of visual impairment (blindness and low vision) in Ethiopia.31 Respectively, about 87.4% and 91.2% of the causes of blindness and low vision in Ethiopia are avoidable (either preventable or treatable). 1.2.4.3.5 Childhood blindness in Ethiopia: The national blindness survey done in 2006 showed a very high prevalence of childhood blindness which is 0.1%. This accounts for over 6% of the total blindness burden in Ethiopia.31 Taking the current population of the country there are about 33,000 blind children in Ethiopia. Despite this huge number of blind children in the country, there is only one paediatric eye care facility nationwide, which is located in the capital city. As already mentioned, there are only four paediatric ophthalmologists in the country and therefore most eye problems in children are handled by either the general ophthalmologist or other health care professionals in a set up where appropriate diagnostic and therapeutic facilities are lacking. According to a study performed in three blind schools in Ethiopia the three common anatomical sites of blindness in 295 children less than 16 years of age were cornea (62.4%), optic nerve (9.8%) and lens (9.2%).22 15 The national blindness survey revealed that the prevalence of trachomatous trichiasis (blinding trachoma) in children of age group 1 to 9 years was 3.1% and the national prevalence of active trachoma in this age group was 40.14%.32 Another community-based study in central Ethiopia showed that 51.1% of children less than 10 years of age had active trachoma (trachomatous inflammation-follicular and/or trachomatous inflammation- intense).33 Significant proportions of children are also blind due to corneal scarring resulting from vitamin A deficiency. The national blindness survey showed that in those less than five years of age the prevalences of night blindness, conjunctival xerosis and Bitot’s spots were 0.1%, 0.9% and 0.7% respectively.31 1.2.4.3.6 VISION 2020 and Ethiopia Ethiopia was one of the first sub-Saharan countries to sign the declaration of support for the global initiative VISION 2020: The Right to Sight. The initiative was launched in Ethiopia in September 2002.34 Ethiopia has established a VISION 2020 National Committee for the Prevention of Blindness (NCPB). It has developed and implemented the first phase national five-year strategic plan for eye care (2001-2005) and also the second phase strategic plan (2006-2010) with active participation of regional states of the country and all partners involved in the prevention of blindness.34 Even if the country has a shortage of resources (skilled professionals and budget) with regard to eye care services, it is trying hard to fulfil and implement successfully the VISION 2020 initiative. Some progress has been made in the country especially with regard to infrastructure and human resource development in eye care. New training centres for ophthalmologists, optometrists, ophthalmic officers, cataract surgeons and ophthalmic nurses have been opened in several locations, and the number of trainees enrolled for training at these institutions has increased. The other big achievement was the completion of the National Survey on Blindness, Low Vision and Trachoma in Ethiopia in 2006. The country is now in the second phase of the five-year national strategic plan (2006-2010) for prevention and control of blindness within the VISION 2020 program. 1.2.4.3.7 Partners in eye care in Ethiopia: In addition to the federal ministry of health, there are a number of nongovernmental organizations and civic societies which are directly involved in prevention of blindness in Ethiopia. These organizations include the following: ORBIS International, Christian Blind Mission (CBM), Light for the World, International Trachoma Initiative (ITI), Help Age 16 International, Menschen fur Menschen (MFM), The Carter Centre, Girarbet Rehabilitation Project, World Vision, Lions Club, and Rotary Club. Had it not been for the great support from these non-profit making organizations, the progresses seen in eye care service delivery and human resource developments in Ethiopia would have not been achieved. The role they play and the work they perform is magnificent and to mention some: they are involved in human resource development by training eye care professionals abroad and within the country and bringing skilled and experienced expatriates to give free services. They are also involved in building infrastructures, eye care training centres and furnishing and equipping them, strengthening the available eye health facilities both in material supplies and human resources. 1.3 -Rationale: The causes of childhood blindness in Ethiopia are not well established and up to this time period there is no separate childhood blindness survey done at a community level in the country to identify the real causes, magnitude and risk factors for childhood blindness. Data available concerning childhood blindness in the country were obtained from either studies at schools for the blind, hospital records or from national blindness surveys where more emphasis had been given to adulthood blindness. Therefore it has been difficult to plan and implement control and preventive measures to tackle childhood blindness in the country as more realistic and evidence-based data regarding the magnitude and extent of the problem have been lacking. This study will identify the causes and magnitude of childhood blindness at a community level in Sekoru district using the key informant method (KIM) which is a relatively new but effective method to identify children with blindness or severe visual impairment through a house-to-house searching strategy.35-40 The findings of this study will help to plan ways to control blindness in children in Ethiopia. 17 2. Aim and objectives of the study: Aim: The overall aim of the study was to determine the magnitude and causes of childhood blindness and severe visual impairment in Sekoru district, Jimma zone, South West Ethiopia. Objectives: The specific objectives were: 1- to estimate the prevalence of childhood blindness using the key informant method, 2- to identify the causes and estimate the relative contribution of each cause to the overall prevalence of childhood blindness, 3- to estimate the proportion of blind children who lost vision from avoidable causes of blindness, 4- to propose ways of preventing and controlling childhood blindness in the district, and 5- to train suitable key informants to find children with blindness or SVI in the district. 18 3. Methodology 3.1 Study design, subjects and area Study design: a population-based cross sectional survey. Study population: children less than 16 years of age living in Sekoru district of Jimma zone. Study subjects: blind/SVI children less than 16 years of age living in Sekoru district. Study period: from June 2009 to September 2009. Study area: Sekoru district of Jimma zone. Jimma zone is about 325km South West of the capital and has 13 districts. It has a total population of about 2.5 million. Sekoru district has 136,297 inhabitants and is about 100kms far Northeast from Jimma town.25 Among others this district was selected for the study because June and July are monsoon seasons in Ethiopia where there is heavy and torrential rainfall and compared to the other districts with regard to transportations, access to Sekoru district during this season is relatively better. N Main road Limu seka Distribution of villages Limu u Kosa Jimma zone Sekoru district Figure 4. Map of the study area (Sekoru district): 3.2 Ethical approval: Ethical approval for the study was obtained from the ethics committee of the London School of Hygiene & Tropical Medicine (LSHTM) and the Research and Publication Committee of 19 Jimma University Hospital. Consent forms were signed by parents or guardians of blind/SVI children in the presence of witnesses before children were recruited for the study. 3.3 Sample size calculation: The expected prevalence of childhood blindness was 0.1%. For a population of 58,480 children in Sekoru district, worst acceptable result of 0.08% and confidence level of 95%, the sample size calculated using Epi info was 36,333. For 99% confidence level, it became 43,225. 3.4 Selection criteria: Inclusion criteria: All children less than 16 years of age with presenting vision less than 6/60 in the better eye (i.e. blind or SVI according to WHO revised ICD-10 categories of VI9) and living in Sekoru district of Jimma zone were eligible for inclusion. Exclusion criteria: children not meeting the inclusion criteria (specifically children whose presenting vision was ≥6/60 in either eye, Children unable to come to the examination centres for any reason, Children for whom consent to participate was withheld. 3.5 Selection of key informants: To be eligible for selection as a KI, candidates were required to satisfy all of the following criteria: Permanent residence in Sekoru district Ability to read and write Ability to speak the local language perfectly Age not greater than 60 years Selection procedure Following explanation about the objectives of the study and thorough discussion with the head and vice head of Sekoru district health bureau, three community mobilizers (who also acted as supervisors for the KIs) were selected for the study. Then, discussion was made on who could be the best KIs in the district. Agreement was reached on selecting those people who had been working as Community Based Reproductive Health Agents (CBRHA) in the district. The CBRHAs were inhabitants in the community who had had frequent previous trainings about common health problems in their community particularly malaria and tuberculosis. They were also involved in the expanded program for immunization (EPI), polio 20 vaccination and vitamin A distributions. They had in-depth knowledge of the customs and culture of their communities, spoke the local language fluently and were educated (at least able to read and write). There were 34 peasant associations (PA) and four towns in Sekoru district. For each PA, we selected one KI, and for each town two KIs, making a total of 42 KIs. The supervisors contacted all the selected KIs to see if they were willing to participate in the study, and all agreed to do the job. 3.6 Training the Key Informants Training sites Training of the KIs was performed on two separate days in two groups at two towns. The training was performed at Sekoru High School in Sekoru town for the first group and at Kumbi High School in Kumbi town for the second group. The first group consisting of 23 KIs was trained on 25/06/09 and the second group of 19 KIs was trained on 26/06/09. Training procedure The purpose of the study was explained to the KIs. Basic information about childhood blindness globally, its magnitude and common causes and the importance of identifying and treating childhood blindness early were discussed in detail. Pictures of children who had been blinded or severely visually impaired as a result of common eye diseases were shown. Discussions were held with the KIs about how to find blind/SVI children living in the towns, villages and PAs. The KIs were also trained on how to measure visual acuity (VA) at 6 metres using the Eletter, including demonstrations on subjects. The KIs then practiced measuring VA on each other until they were all performing this task well. Lots of questions were raised by the KIs including whether or not to bring children with eye problems or eye discharge who were still able to identify the E-letter at six metres, children who were blind in one eye only, or children who could see at day time but not at dusk or night hours, etc. These questions were answered by the main investigator. The training was given for half a day at the selected sites for each group on two different days. Finally, six convenient examination sites (one health centre and five clinics) were chosen for later examination of identified blind/SVI children by the ophthalmologist could take place. Each KI was given instructions on where and on which days they should take the blind/SVI children they identified. The examination centres chosen were Sekoru health centre, Baso clinic, Deneba clinic, Natri clinic, Kumbi clinic and Abelti clinic. Each KI was given an E-letter, a pen and a notepad. 21 3.7 Data collection Finding blind/SVI children: Following the half day training, each KI returned to their respective village and contacted the village leaders. The KI together with the village leader explained their new task and duty to the villagers in places where people gather like religious areas, market places and community meetings. The community were asked to name or bring those children with visual impairment to the KI. The village leader also identified for the KI all village households with children who the village leader knew to have eye problems. The KI also contacted the church and mosque leaders who introduced him/her and asked the people to bring all children with vision problem to the KI. The KIs also announced to the public at market places and sensitized the community. The main job of the KI was to go systematically from house to house through all the villages for which they have been assigned responsibility, and look for children with visual problems. For identified children > 5 years of age considered to be blind/SVI, vision was measured by the KI outdoors and in daylight at six metres using the E letter. All children <5 years of age and suspected of being blind/SVI either by parents or KIs were brought to the examination centres to be examined by the ophthalmologist. The names, sex and ages of all children identified as blind/SVI by the KIs were listed. Parents and guardians of children identified as blind/SVI by the KIs were told to bring the child on the specified dates to one of the places identified above, for examination by the ophthalmologist. 3.8 Examination of identified children by Key Informants Consent form: The KIs came to the examination centres together with the identified blind/SVI children and their parents/guardian. Before the ophthalmologist examined children brought by the KIs at the chosen referral places, the purpose of the study was explained to each parent, their willingness to participate was confirmed and the consent was read aloud to them in the local language before being signed by each parent. Only then did the investigator proceed to examine the children. Measuring visual acuity: Using a logarithm of minimum angle of resolution (logMAR) visual acuity chart, presenting vision was measured at six metres in a well lit room for those above 5 years of age. Pinhole vision was also measured and subjective refraction using a trial frame lens set was performed for those whose vision showed improvement with pinhole. Neither intraocular pressure nor visual field was assessed. 22 Ocular examination: Ocular alignment and motility tests were performed. A torch and magnifying loop (+2.5) were used to examine the adnexiae and anterior segment of the eye including the lens. Fundus examination was performed using a direct ophthalmoscope. Cyclopentolate eye drops were used to dilate the pupils when indicated. The most likely cause of blindness was identified and finally diagnosis was made. Ocular findings of those diagnosed as blind/SVI were recorded on the modified WHO/PBL eye examination record for children with blindness and low vision. For children with reversible causes of blindness referral to Jimma University Hospital was made for proper management free of charge. Transportation fees were provided to parents who said that they had no money for transport to Jimma Hospital. Parents of those with irreversible causes of blindness were counselled and advised of the advantages of enrolling their children in schools for the blind. Vitamin A capsules were distributed to all examined children and full prescriptions were given to those who needed medications. Figure 5. Flow diagram of children identified by KIs as blind/SVI. Children with vision < 6/60 (better eye) Referred to ophthalmologist (examination centres) VA measured by ophthalmologist VA > 6/60 (either eye) VA <6/60 (better eye) Excluded from the study (Sent home with advise &/or Treatment) Recruited to the study Consent form signed History taking and Systematic ocular examination done Data recorded on WHO/PBL record form Diagnosis & Management plan (Counselling/Referral to eye hospital) 23 3.9 Data recording, entry and analysis: At the examination centres, data obtained from examined blind/SVI children were recorded on the WHO/PBL eye examination record for children with blindness and low vision form.41 Data cleansing/scrubbing was performed manually by the ophthalmologist. All data obtained were entered manually into a computer on excel sheet and subsequently transferred to SPSS and STATA softwares and analysed using SPSS 16 and STATA 10.1 software programs (licensed to LSHTM student labs). Table 4. Summary of field activities at Sekoru district. Activities Week 1 Week 2 Visiting the area, KIs selection & training Finding BL/SVI children by KIs Examination by ophthalmologist Networking Monitoring 24 Week 3 Week 4 4. Results: There were 42 KIs trained (one KI for each PA and two KIs for each town). Thirty-four (81%) of them were males and 8 (19%) were females (table 5). Their ages ranged from 23 years to 54 years with a median and mean of 32 and 37 years respectively Table 5. Key informants trained and number of blind/SVI children identified KIs NO. TRAINED (%) NO. OF BLIND/SVI CHILDREN IDENTIFIED (%) 34 (81) 31 (86) 8 (19) 5 (14) 42 (100) 36 (100) Males Females TOTAL (%) Children identified by KIs: Hundred and twelve children were taken to the examination centres by the 39 KIs. Three KIs (two males and one female) did not bring any children. This means on average one KI took 2 to 3 children to the examination centres. Of the 112 children examined 36 (32%) were either blind or severely visually impaired. The rest had either minor visual problems or were unilaterally blind. There were 20 (55.5%) male and 16 (44.5%) female blind/SVI children identified making the male to female ratio 1.25:1 (5:4). Seven (19.4%) of the blind/SVI children were below the age of 6 years and 10 (27.8%) were between 6 and 11 years. Nineteen (52.8%) of the identified blind/SVI children were above the age of ten. The mean age was 10.7 years. Only six (16.7%) of the blind/SVI children were enrolled in schools, one in a school for the blind near Addis Ababa, the rest (five) in integrated schools locally together with sighted children. The age and sex distribution of the blind/SVI children is as follows. Table 6. Age & sex characteristics of blind/SVI children identified MALE FEMALE TOTAL (%) 0-5 4 3 7 (19.4) 6-10 6 4 10 (27.8) 11-15 10 9 19 (52.8) TOTAL (%) 20 (55.5) 16 (44.5) 36 (100) Age (years) 25 Causes of blindness/SVI: The commonest anatomical site of pathology producing blindness/SVI was the lens which accounted for 33.3% of the cases, followed by the cornea which was responsible for 27.8% of cases. Of the seven children who had whole globe abnormalities four had congenital glaucoma and three had bilateral phthisical eyes of unknown aetiology. Refractive error was the next most common cause, accounting for 16.7% of blindness/SVI (table 7). Table 7. Anatomical causes of blindness/SVI ANATOMY NUMBER Whole globe 7 Cornea 10 Lens 12 Refractive error 6 Optic nerve 1 TOTAL 36 PERCENT (95% CI) 19.4 (8.2-36.0) 27.8 (14.2-45.2) 33.3 (18.6-51.0) 16.7 (6.4-32.8) 2.8 (0.10-14.5) 100% 26 Pictures 1-4. Some of the children who were blind and identified by key informants 1. A child with congenital 2. glaucoma and blind. Bilateral dense cataract in a blind child (after pupils were dilated). 4. Corneal scarring/phthisis in a 14-yr-old 3. Bilateral congenital cataract girl secondary to VAD. (before pupils were dilated). 27 Of the 36 children identified, 30 (83.3%) were blind, with presenting vision less than 3/60 and the rest 6 (16.7%) had SVI with presenting vision <6/60 but better or equal to 3/60 in the better eye (table 8). Table 8. Proportion of identified children who were blind and SVI. Visual acuity Number Percent Blind 30 83.3 SVI 6 16.7 Total 36 100 Table 9. Causes of blindness/SVI by age group. Causes 0-5 years 6-10 years 11-15 years Cataract 3 3 6 Corneal opacity 3 2 5 Refractive error 0 3 3 Glaucoma 1 1 2 Phthisis bulbi 0 0 3 Optic hypoplasia 0 1 0 7 (19.4%) 10 (27.8%) 19 (52.8%) Total Total (95% CI) 12 (33.3%) (18.6-51.0) 10 (27.8%) (14.2-45.2) 6 (16.7%) (6.4-32.8) 4 (11.1%) (3.1-26.1) 3 (8.3%) (1.8-22.5) 1 (2.8%) (0.1-14.5) 36 (100%) In all age groups, cataract was the commonest cause of blindness. Corneal opacity and RE were just as common as cataract as causes of blindness/SVI in age groups 0-5 and 6-10 years respectively. Corneal opacity was the second commonest cause of blindness in age groups 11-15 years. Most of the pathology seen in this cohort of blind/SVI children was of unknown aetiology, as seen in the following table. In about 64% of cases (23 children) the underlying aetiology of blindness could not be identified. The majority of these cases involved congenital cataract. In 25% (9 cases) of the children factors acquired during childhood were the causes of blindness/SVI, these were mostly corneal opacities resulted from VAD. Intrauterine factors accounted for 5.56% of the cases and hereditary and neonatal factors accounted for 2.78% of the cases each. 28 Table 10. Aetiological classification of causes of blindness/SVI. AETIOLOGY NUMBER Hereditary 1 Intrauterine 2 Neonatal 1 Postnatal (infancy/childhood) Unknown aetiology 9 23 TOTAL 36 PERCENT (95% CI) 2.8 (0.1-14.5) 5.6 (0.7-18.7) 2.8 (0.1-14.5) 25 (12.1-42.2) 63.9 (46.2-79.2) 100% Two of the children were operated on both eyes for congenital cataract previously (ECCE+PC-IOLExtra Capsular Cataract Extraction plus Posterior Chamber Intraocular Lens) but their vision remained less than 6/60 due to bad outcomes. Another two were operated for congenital glaucoma (partial thickness trabeculectomy was done). 29 5. Discussion: The use of key informants is a relatively new method of identifying which children in a community have visual problems. The key informant method (KIM) has been proven to be effective in identifying blind/SVI children especially in low and very low income countries like Ethiopia where resources to undertake more formal searches are scarce. KIs are relatively cheaper and also in some countries they are volunteers who do not need any form of payments for their activity.35, 37, 38 In our study the key informants trained were people who have previously been serving their community as Community Health Agents (CHA) previously and who had recently upskilled to become Community Based Reproductive Health Agents (CBRHA). They had been working in this post for four to eight years. They all had good knowledge and details of the community they were working in and basic baseline information concerning health issues. They were able to cover their respective PAs and villages within the time period allocated to find blind/SVI children. They brought a total of 112 children to the examination centres from the 38 PAs and 4 towns in the district, of whom 36 children (32%) were found to be either blind or SVI. This implies that of three children they brought one was either blind or severely visually impaired. Of the 136,000 people in Sekoru district about 43% (58,480) are children aged less than 16 years. Based on the national blindness survey’s estimated childhood blindness prevalence of 0.1%, we expected 58 blind children in Sekoru district. But we actually identified 36 blind/SVI children which makes the prevalence of childhood blindness in Sekoru district 0.062% (95% CI =0.041-0.082) in this study. This prevalence rate is lower than that of the national estimate which was undertaken in 2006 (0.062% vs. 0.1%).31 Thirty of the identified children (83.3%) in this study were blind having presenting vision of < 3/60 in the better eye and the rest six (16.7%) had SVI (table 8). In a similar study undertaken in Bangladesh, 91.5% of the 1935 identified children were blind and the rest (8.5%) were severely visually impaired.36 Most of the blind children identified were in the higher age group. Nineteen (52.7%) of the blind/SVI children were aged 11 to 15 years, of whom 8 were 15 years of age. This is similar to the Bangladesh study where over half of the studied children were aged 11-15 years.36 It is of course difficult to prove ages of the children as there is no official registration of births in these rural communities, so we relied on parental report. Therefore some of those who claimed to be 15 years of age might actually have been older than that. In this study the mean age was 10.4 years which is higher than the mean age obtained in a similar study in Malawi (8.0 years).39 30 Causes of blindness and SVI: According to site of abnormality: Causes and prevalence of childhood blindness vary from country to country depending on the socio economic status, U5MRs and availability of health care facilities. In affluent countries prevalence is very low and most of the causes of blindness are due to factors which are unavoidable (not preventable or treatable).14, 20 In very poor developing countries like Ethiopia the prevalence is very high and the majority of the cases are due to avoidable conditions like cataract and corneal scarring resulting from VAD.20 Lens abnormality (congenital cataract and pseudophakia) was the commonest anatomical cause of blindness identified in this study. It accounted for 33.3% (12 cases) of all blindness. Of the 12 cases identified ten had congenital cataract and two were pseudophakic who developed dense posterior capsular opacity. Previous study in three schools for the blind in Ethiopia showed that cataract/aphakia accounted only for 9.2% of blindness which is much lower than in this study. 22 In other community based studies using KIs in Malawi39 and Bangladesh,36 lens abnormalities accounted for 35% and 32.5% of blindness respectively: similar proportion to the current work. Cataract is now replacing corneal scarring as the leading cause of childhood blindness and low vision in sub Saharan African countries and the rest of the developing world. There is a reduction in prevalence of preventable causes of childhood blindness in developing countries as a result of better measles immunization coverage and distribution of vitamin A capsules to young children. 4, 20, 24, 36, 42 Corneal scarring due to vitamin A deficiency was the second commonest cause of vision loss in children in this study accounting for 27.8% of all cases. In the previous study in schools for the blind in Ethiopia carried out in 2001 VAD accounted for 62.4% of blindness.22 Even though direct comparison may not be possible, this apparent reduction in prevalence of blindness from VAD could be due partly to the extended distribution of vitamin A capsules to children during the expanded programs of immunisation plus better measles immunization coverage and due to relatively better health care services nowadays. The health care service delivery system and the number of health posts in the rural areas is now relatively better than the previous periods addressing the health issues of most of the rural communities. In studies in other settings, VAD does appear to be becoming second to congenital cataract as the main cause of childhood blindness in the developing world. 24, 39 A recent study performed in schools for the blind in four east African countries showed that corneal scarring/phthisis bulbi was the commonest cause of blindness/SVI accounted for 19% of the cases. 43 Another study in India showed that 19% (ranging from 8 to 27% in different States) of 1318 blind/SVI children examined had lost vision due to VAD.44 The actual number of cases of blindness resulting from VAD could be higher and the prevalence of blindness/SVI due to VAD could easily be underestimated by virtue of the fact that the chance of 31 dying from associated protein energy malnutrition and other essential nutrients in these children is very high. The contribution of VAD to childhood mortality is a well known fact.45 There were six children (16.7%) with significantly high degree of refractive error. All of them were cases of high myopia (10-12 dioptres) and none of them were wearing corrective glasses as they had never been seen by eye health professionals. It was less likely that they had developed deep amblyopia as in all cases vision improved to 6/18 - 6/60 with corrective glasses. This means they would have been out of the blindness/SVI category had it not been for the lack of corrective glasses. RE is not a major cause of blindness in children but is one of the common causes of low vision.46 Globally around 12.8 million children between 5-15 years of age have visual impairment as a result of uncorrected or inadequately corrected RE making the global prevalence of RE in children 0.96%.1 In a study in Nigeria, however, RE was the cause of loss of vision in about 59% of those children between 5 and 15 years of age.47 Congenital glaucoma was the cause of blindness in about 11.1% (4 cases) of children identified in this study. Two cases had had the problem since their first year of life, as evidenced by the presence of buphthalmos plus suggestive family history. In a similar study in Bangladesh, glaucoma was the cause of blindness/SVI in 4.3% of the identified children.36 In the study made in schools for the blind in Ethiopia, glaucoma/buphthalmos accounted for only 1.7% of the blindness. 22 In other studies in schools for the blind in Nigeria,24 Malawi, Kenya, and Uganda23 and China48 glaucoma and buphthalmos were the causes of blindness and SVI in 9.3%, 3.7%, 6.5%, 3.4% and 9% of the children respectively. There were three children (8.3%) with phthisis bulbi of unknown aetiology and only one case (2.8%) of bilateral optic nerve hypoplasia with nystagmus which implies that the pathology had been there since early life. In similar study in Bangladesh optic nerve diseases were responsible for blindness in 5.3% of the identified children.36 In schools for the blind in Malawi, Kenya and Uganda optic nerve lesions were found in 5.1%, 10.4% and 13.3% of the blind/SVI children respectively.23 According to the aetiology of Blindness/SVI: In this study the majority of cases of blindness and SVI had unknown aetiology; in 63.89% of cases it was not possible to categorize the blindness/SVI to one of WHO’s four aetiological classifications; these cases involved congenital cataract. In schools for the blind in Ethiopia, the aetiology of blindness/SVI could not be determined in 45.1% of children.22 Of cases of known aetiology, 25% of blindness/SVI was due to childhood factors which are secondary to vitamin A deficiency in this study. Kello found that childhood factors (mainly VAD) accounted for 49.8% of the cases.22 In the study by Muhit et al, 30.7% of cases were due to childhood factors resulting in corneal scarring principally from vitamin A deficiency.36 There were two congenital cataract cases secondary to congenital rubella infection suggested by the type of the cataract they developed and lack of history 32 of immunization of the mother prior to pregnancy. There was also one case of bilateral corneal scarring secondary to ophthalmia neonatorum. 2.78% 5.56% 2.78% Hereditary Intrauterine 25% Perinatal Childhood 63.89% Unknown Figure 6. Aetiological classification of causes of childhood blindness/SVI at Sekoru district. Avoidable causes: Majority of cases of blindness (89%) in this study were due to avoidable causes (either preventable or treatable) and the children were therefore blind needlessly (figure 5). Cataract, corneal opacity, RE, and congenital glaucoma are all treatable surgically; corrective glasses can easily be provided, and other conditions were preventable with appropriate measures directed to the community including health education, antenatal care and immunizations. A study done in South East Nigeria suggested that 74.5% of cases there were avoidable.24 Out of the 36 blind/SVI children identified, vision could improve in 20 (55.5%) of them if appropriate therapeutic measures were taken. Fourteen (38.9%) of the cases needed surgical interventions (ten needed cataract extraction, two needed YAG laser capsulotomy, and two needed optical iridectomy) and six (16.7%) cases required corrective glasses. But in the remaining 16 (44.5%) cases, vision could improve neither with treatment nor with provision of glasses (i.e. they had irreversible vision loss) (figure 7). 33 89% 90% 80% Avoidable causes 70% 55.50% 60% Unavoidable causes 44.50% 50% 40% Reversible vision loss Irreversible vision loss 30% 11% 20% 10% 0% Childhood blindness Figure 7. Proportion of avoidable/unavoidable causes of blindness/SVI and reversible/irreversible vision loss at Sekoru district, Ethiopia. Limitations of the study: 1. There was a lack of adequate baseline data and information concerning low vision and blindness in childhood in the region. As is true in most developing countries, there is no national blindness registration system in Ethiopia. 2. Following their one day training session, pretesting (pilot testing) of KIs on children in order to demonstrate understanding of study procedures was not done. 3. The data collection period was short for the survey as KIs needed to travel long distances to remote rural areas by foot. 4. June and July are monsoon months in Ethiopia and it was difficult for the KIs to travel to the very remote and rural areas; unfortunately, due to restrictions imposed by the UK academic year, these months were the only ones in which data collection could be completed. Identified blind/SVI children and their parents also had difficulties coming to examination centres as the roads were muddy and there were no means of transport except foot. 5. Children between 11-16 years of age might have been over represented in this study as they constituted 52.8% of the study subjects. Consequently, the ocular diseases diagnosed in this age group might have been overestimated. 6. Children who were blind/SVI but sick or unable to come to the examination centre for any reason were not included in the study resulting in underestimation of overall prevalence, and perhaps a bias in the estimation of the relative contribution of various causes of blindness and SVI. 34 Strengths of the study included: 1. This was a community based survey performed using KIs which have been proven to be an effective method in other African and Asian countries with similar socioeconomic status. 2. KIM is a type of population-based study; hence identified children using this method were more likely to be representative of the children’s community, than, for example, studies performed in schools for blind children. 3. The study was sufficiently powered: the theoretical population of children covered by the study (the number of children in the district, 58,480) was higher than the calculated sample size (36,333). 35 6. Conclusions: Despite the limitations mentioned above, the following conclusions and recommendations are made: 1. The prevalence of childhood blindness and SVI in Sekoru district of Jimma zone is lower than that estimated by the national blindness survey done three years ago (0.062% v 0.1%). 2. The causes of blindness in children in Sekoru district included congenital cataract, corneal scarring from VAD, RE, congenital glaucoma, phthisis bulbi and optic hypoplasia. 3. Cataract is the major cause of blindness and SVI in Sekoru district followed by corneal scarring resulting from VAD. 4. Refractive error is responsible for a significant proportion of childhood blindness/SVI in Sekoru district. The attention given to this problem is clearly inadequate despite the fact that it can be corrected with simple refraction and distribution of corrective glasses without the need for more sophisticated intervention. 5. Overall eighty-nine percent of blindness and severe visual impairment in children in Sekoru district is from avoidable causes. 6. Different studies in different countries have shown that identifying blind/SVI children in the community using KIM is useful and relatively cheap. This is particularly true in resource scarce countries where sophisticated ways of doing surveys may be difficult and too costly to contemplate.35, 37, 38 This study has shown that KIs could be a useful means of ascertaining children who are blind/SVI in rural community of Ethiopia. 36 7. Recommendations: 1. Cataract has been found to be the leading cause of childhood blindness in Sekoru district of Jimma zone. To handle this problem effectively, it is recommended to train a paediatric ophthalmologist and one anaesthesiologist to perform better quality cataract surgery for these blind children in the region. 2. It is mandatory to equip and furnish adequately the existing ophthalmology department in Jimma zone with appropriate paediatric ophthalmic instruments including operating microscopes and general anaesthesia machines. 3. Corneal scarring is the second major cause of blindness in children in Sekoru district. Conditions predisposing children to VAD like diarrheal diseases and respiratory infections should be addressed properly. Health education, measles immunization, antenatal care follow-up and vitamin A distributions need to be strengthened further. 4. Refraction services in the region need to be reinforced. Regular school vision screening programs which will have a paramount importance in identifying children with refractive errors in schools have to be started. 5. KIM can be used in Ethiopia to explore the magnitude and causes of childhood blindness and SVI at zonal or national level. 37 8. References: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Resnikoff Serge, et al., Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bulletin of the world health organisation, 2008. 86: p. 63-70. WHO press release. Sight test and glasses could dramatically improve the lives of 150 million people with poor vision. Geneva. 2006. Accessed online on August 24, 2009. http://www.who.int/mediacentre/news/releases/2006/pr55/en/index.html. Allen Foster, Clare Gilbert, and G. Johnson, Changing patterns in global blindness: 19882008. Community Eye Health, 2008. 21(67): p. 37-39. Clare Gilbert and M. Muhit, Twenty years of childhood blindness: what have we learnt? Community Eye Health Journal, 2008. 21(67): p. 46-47. Clare Gilbert and H. Awan, Blindness in children. British Medical Journal, 2003. 327: p. 760761. Resnikoff Serge, et al., Global data on visual impairment in the year 2002. Bulletin of the World Health Organization, 2004. 82: p. 844-851. WHO, Study Group on the Prevention of Blindness. WHO Technical Report Series No.518. World Health Organization, Geneva, 1973: p. 10-11. International Statistical Classification of Diseases and related Health Problems, 10th revision. Geneva: World Health Organization 1992: p. 456-57. WHO, Consultation on Development of Standards for Characterization of Vision Loss and Visual Functioning. Geneva, 2003. Accessed online on August 24/08/2009, http://whqlibdoc.who.int/hq/2003/WHO_PBL_03.91.pdf. WHO, Preventing blindness in children: report of WHO/IAPB scientific meeting. Hyderabad, India, 13-17 April 1999. accessed online on 20/08/2009, http://whqlibdoc.who.int/hq/2000/WHO_PBL_00.77.pdf. Clare Gilbert, H.A., Blindness in children. British Medical Journal, 2003. 327: p. 760-761. WHO, VISION 2020, The Right to Sight: . Global initiative for the elimination of avoidable blindness: Action plan 2006-2011, Accessed online on 22/08/2009, http://www.who.int/blindness/Vision2020%20-report.pdf. WHO, VISION 2020, The Right to Sight. . Global initiative for the elimination of avoidable blindness: Action plan 2006-2011, Accessed online on 22/08/2009, http://www.who.int/blindness/Vision2020%20-report.pdf. Clare Gilbert and A. Foster, Childhood blindness in the context of VISION 2020-The Right to Sight. Bulletin of the World Health Organization, 2001. 79: p. 227-232. Clare Gilbert, Jugnoo S Rahi, and G.E. Quinn, Visual impairment and blindness in children. In: Gordon J J, Darwin C M, Robert A W, Sheila K W, eds. The Epidemiology of Eye Disease, Arnold, 2003 p. 261-286. Gilbert, C., New Issues in Childhood Blindness. Community Eye Health Journal, 2001. 14(40): p. 53-56. Rakhi Dandona and L. Dandona, Socioeconomic status and blindness. Br J Ophthalmol, 2001. 85: p. 1484-88. Foster A, G.C., Epidemiology of childhood blindness. Eye, 1992. 6: p. 172-176. Susan Lewallen, P.C., Blindness in Africa: present situation and future needs. British Journal of Ophthalmology, 2001. 85: p. 897-903. Gilbert, C., Changing challenges in the control of blindness in children. Eye, 2007. 21(10): p. 1338-43. Gilbert CE, et al., Prevalence of visual impairment in children: a review of available data. Ophthalmic Epidemiology, 1999 6(1): p. 73-82. Kello, A.B. and C. Gilbert, Causes of severe visual impairment and blindness in children in schools for the blind in Ethiopia. British Journal of Ophthalmology, 2003. 87(5): p. 526-30. 38 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. Gilbert, C.E., et al., Causes of childhood blindness in east Africa: results in 491 pupils attending 17 schools for the blind in Malawi, Kenya and Uganda. Ophthalmic epidemiology, 1995. 2(2): p. 77-84. Ezegwui, I.R., R.E. Umeh, and U.F. Ezepue, Causes of childhood blindness: results from schools for the blind in south eastern Nigeria. British Journal of Ophthalmology, 2003. 87(1): p. 20-3. Central Statstical Agency of Ethiopia. 2007. http://www.csa.gov.et/, (accessed online on 20/08/2009). WorldHealthOrganization, Country Health System Fact Sheet 2006 Ethiopia. http://www.afro.who.int/home/countries/fact_sheets/ethiopia.pdf, 2006(accessed online on 22/08/2009). Samuel G, et al., Human Resource Development for Health in Ethiopia: Challenges of Achieving the Millennium development Goals. Ethiopian Journal of Health Development, 2007. 21(3): p. 216-231. Teklay Kidane, et al., National EPI coverage survey report in Ethiopia, 2006. Ethiopian Journal of Health Development, 2008. 22(2): p. 148-157. UnitedNationChildren'sFund2008, http://www.unicef.org/infobycountry/ethiopia_statistics.html#54. accessed online on August 21, 2009. M Melese, et al., Low vision and blindness in adults in Gurage Zone, central Ethiopia. Br J Ophthalmol, 2003. 87: p. 677-680. Yemane Berhane, et al., Prevalence and causes of blindness and Low Vision in Ethiopia. Ethiopian Journal of Health Development, 2007. 21(3): p. 204-210. Yemane B, et al., Prevalence of Trachoma in Ethiopia. Ethiopian Journal of Health Development, 2007. 21(3): p. 211-215. Abebe Bejiga, W.A., Prevalence of trachoma and its determinants in Dalocha District, Central Ethiopia. Ophthalmic Epidemiology, 2001. 8(2-3): p. 119-125. MinistryofHealth, National five-year strategic plan for eye care in Ethiopia (2006-2010). Disease Prevention and Control Department, 2006. Muhit, M.A., Finding children who are blind. Community Eye Health Journal, 2007. 20(62): p. 30-31. Muhit, M.A., et al., Causes of severe visual impairment and blindness in Bangladesh: a study of 1935 children. British Journal of Ophthalmology, 2007. 91(8): p. 1000-4. Muhit M A, et al., The key informant method: a novel means of ascertaining blind children in Bangladesh. Br J Ophthalmol, 2007. 91: p. 995-999. Kalua, K., et al., Productivity of key informants for identifying blind children: evidence from a pilot study in Malawi. Eye, 2009. 23(1): p. 7-9. Kalua, K., et al., Causes of blindness among children identified through village key informants in Malawi. Canadian Journal of Ophthalmology, 2008. 43(4): p. 425-7. Boye, J., Validating key informant method in detecting blind children in Ghana. Community Eye Health Journal 2005. 18(56): p. 130-134. Gilbert C, et al., Childhood blindness: a new form for recording causes of visual loss in children. Bulletin of the World Health Organization, 1993. 71(5): p. 485-9. Waddell K, Childhood blindness and low vision in Uganda. Eye, 1998 12: p. 184-92. Njuguna M, et al., Causes of severe visual impairment and blindness in children in schools for the blind in eastern Africa: changes in the last 14 years. Ophthalmic Epidemiol, June 2009. 16(3): p. 151-5. J S Rahi, S.S., C E Gilbert, A Foster, Childhood blindness due to vitamin A deficiency in India: regional variations. Arch Dis Child, 1995. 72: p. 330-333. 39 45. 46. 47. 48. Alfred Sommer, K.P.W., Vitamin A Deficiency: Health, Survival and Vision. American Journal of Epidemiology, 1998. 147(12): p. 1175-6. G. V. S. Murthy, et al., Refractive Error in Children in an Urban Population in New Delhi. Investigative Ophthalmology & Visual Science, 2002. 43(3): p. 623-631. Umeh, R.E., The cause and profile of visual loss in an onchocerciasis-endemic forestsavanna zone in Nigeria. Ophthalmoic epidemiology, 1999. 6: p. 303-315. S J Hornby, Y.X., C E Gilbert, A Foster, X Wang, X Liang, H Jing, L Wang, W Min, Y Shi, Y Li, Causes of childhood blindness in the people's republic of China: results from 1131 blind school students in 18 provinces. British Journal of Ophthalmology, 1999. 83: p. 929932. 40 Appendices: Appendix 1. Ethics application form 41 42 43 Appendix 2. Ethics approval letter- Local 44 Appendix 3: Consent form Consent Form: I, ………………………………………………………………………………………………., have read or had read to me in my own language the attached patient information sheet and I have understood the information in it. As a father/mother/guardian, I agreed and understood that my child is participating in a study entitled ’’Magnitude and causes of childhood blindness/SVI at Sekoru district of Jimma zone Southwest Ethiopia: The key informant method’’ which is conducted by Dr Berhan Solomon Demissie, International Centre for eye health, London School of Hygiene and Tropical Medicine, London, UK. This will involve interviews and eye examinations. My queries have been answered to my satisfaction. I also give my permission for the publication of the child’s photographs for all educational and fund raising purposes to control childhood blindness, but not for advertising purposes. Signature ………………………………… Date ………………………………………… 45 Appendix 4: Patient Information Sheet Patient Information Sheet: Project: Magnitude and causes of childhood blindness/SVI at Sekoru district of Jimma zone Southwest Ethiopia: The key informant method. Investigator: Dr Berhan Solomon Demissie We will be very thankful if your child participates in this study. Please listen to this form carefully to know about the rationale of this study. Please do not hesitate to ask any questions you feel for clarification before deciding whether you allow your child to participate in the study or not. We are ready to give you all information you want to know about. Why to carry out this study: This study will know the magnitude and identify the causes of childhood blindness at Sekoru district using key informants selected from your own community. This will help to recommend ways of controlling and preventing childhood blindness in the area in the future. Children identified as blind with treatable causes will have arrangements for free treatment at Jimma University hospital. This all depends on your willingness: It is totally up to you to decide whether your child participates in the study or not. We are giving you this information and will ask you to sign on an informed consent form if you agree. If you decide not to participate, it will not affect your medical care to you or your family in anyway. Besides, if you agree and accept, you are still free to withdraw from the study anytime without having any special reason. We will give a free eye examination by an ophthalmologist and offer appropriate treatment when needed. There will be no harm during examinations and you will be by the side of your child all the time during the examinations. Your child’s participation in this study will help to provide better childhood eye care services in your community in the future. This study is undertaken as a part of a master’s degree at international centre for eye health at London School of Hygiene and Tropical Medicine (LSHTM) and has been approved by the research and publication committee of Jimma university hospital and ethics committee of LSHTM. If you need any more information at any time you can contact me with the following address: Dr. Berhan Solomon Demissie, Jimma University Hospital, PO Box 1761 Telephone # 251 0911 406524 Email: [email protected] Thank you so much for your attention. 46 Appendix 5: Combined academic and risk assessment approval (CAR form) 47 48 49 50 51 52 53 54 55 56 57 58 Appendix 6. Letter of support to Sekoru district health bureau in Amharic language. 59 Appendix 7. Use of photographs consent form 60 Appendix 8. Use of photographs consent form 61 Appendix 9. Use of photographs consent form 62 Appendix 10. Use of photographs consent form 63 Appendix 11. Questionnaire form 64 65 Appendix 12. MSc project report (feedback) 66 67 68 69 Appendix 13. Curriculum for training key informants: Job description: to look for blind or severely visually impaired children Selection criteria: Permanent residence in Sekoru district Ability to read and write Ability to speak the local language perfectly Age not greater than 60 years Objectives: Following the training each key informant should able: To communicate with parents or guardian of a blind/SVI child To recognise a blind or SVI child in the community To do vision test at 6 metres using E-letter To convince parents to bring their blind/SVI child to examination centre Teaching method: Lectures Demonstrations Group discussions Role play Place: High schools (Sekoru, Kumbi) Time table: total 4 hours and 30 minutes ACTIVITY DURATION Introduction 15 minutes Lecture 1 hr and 30 minutes Break time 15 minutes Discussion 30 minutes Demonstrations 30 minutes Role play 1 hour Questions and answers Total duration 30 minutes 4 hours and 30 minutes 70