Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
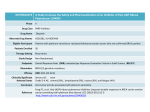
SERIOUS ADVERSE EXPERIENCE REPORT for the Onchocerciasis Treatment Program A serious adverse experience (SAE) is defined as an adverse experience following treatment with a drug that results in any of the following: death life-threatening adverse drug experience in-patient hospitalization or prolongation of an existing hospitalization persistent or significant disability/incapacity congenital anomaly or birth defect cancer overdose (accidental or intentional) Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered a serious adverse drug experience when, based upon appropriate medical judgment, they may jeopardize the patient or subject, and may require medical or surgical intervention to prevent one of the outcomes listed in the definition above: such events should also be reported. COMPLETE THIS FORM ONLY IF THE ADVERSE EXPERIENCE MEETS THE ABOVE CRITERIA and send it promptly to: Mectizan Donation Program 325 Swanton Way Decatur, GA 30030 USA TEL: +1-404-371-1460 FAX: +1-404-371-1138 E-mail: [email protected] 1 Annex VI-D May08 Serious Adverse Experience (SAE) Report Onchocerciasis Treatment Program Country: Date of Report: / / (Day/Month/Year) 1. Patient Information Name (First/Middle/Last) Age (yr.) Village District Sex (M/F) Province 2. Pre-existing Conditions Health Status before treatment with Mectizan (including any CNS disability): Parasitic Infections 1. Onchocerciasis 2. Loiasis If Loiasis is confirmed Confirmed Suspected mf/ml (blood): Unknown … or mf/smear: Other parasitic infections, known or suspected (e.g. Malaria) Negative Details mf/ml (CSF): Other medications being taken (currently or recently) Is patient pregnant? Yes No Unknown Alcohol: a) Consumption of alcohol within 24hrs of taking Mectizan b) History of Chronic Alcoholism 3. Information on Recent Mectizan Treatment Date of treatment (Day/Month/Year): Source of treatment: Community treatment program Clinic or physician treatment Other method / / Dose of Mectizan administered (no. of tablets) Was this a first treatment with Mectizan? Yes Patient’s height (cm) No Patient’s weight (kg) Unknown If “No”, explain when and circumstances of past treatment(s): 2 Annex VI-D May08 4. Description of the Serious* Adverse Experience (SAE) / / hours OR Date of onset (Day/Month/Year) days How long after Mectizan was taken? Clinical signs and symptoms Were there signs of acute alcohol intoxication on initial examination ?: Yes No Unknown Dates of tests (Day/Month/Year) Laboratory results / / / / / / Case management, clinical course, drugs used (e.g. Hospitalization – provide date of admission and summarize the reason for admission): a) Hospitalization: If “Yes”, indicate: Yes No Date of admission (Day/Month/Year): / / Date of discharge (Day/Month/Year) : / / (Attach any relevant reports) b) Drug treatments administered: *A serious adverse drug experience is an adverse experience occurring at any dose that results in any of the following outcomes: death, a life-threatening adverse drug experience, in-patient hospitalization or prolongation of an existing hospitalization, a persistent or significant disability/incapacity, a congenital anomaly/birth defect, a cancer, or an overdose (whether accidental or intentional). Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered a serious adverse drug experience when, based upon appropriate medical judgment, they may jeopardize the patient or subject and may require medical or surgical intervention to prevent one of the outcomes listed in this definition. 3 Annex VI-D May08 5. Condition/Outcome at time of last observation Full recovery: Yes No Unknown Ongoing illness: Yes No Unknown Persistent/Significant Disability/Incapacity: Yes No Unknown If “Yes”, describe: Death: Yes Date of death (day/month/year) No If “Yes”, indicate / Cause of death / In fatal cases please provide circumstances at the time of death in detail below. Report any autopsy findings made including tissues taken for histopathology and any additional studies done or requested (use additional pages necessary to complete your answers): Presumptive diagnosis: 6. Conclusions Do you think the treatment with Mectizan was a causative possible factor in this SAE? Yes No Not sure If “Yes”, explain: If “No”, or “Not sure”, what do you believe was the cause of the event? 4 Annex VI-D May08 7. Source (reporter(s) of the data in this form) Name of person making the report Title Organization Address Telephone number Fax number Please send this report to the following: Mectizan Donation Program 325 Swanton Way Decatur, GA 30030 USA TEL: +1-404-371-1460 FAX: +1-404-371-1138 E-mail: [email protected] 5 Annex VI-D May08