Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
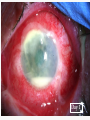
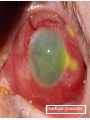
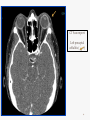
Authors: K Michael, D Lyall, D Anijeet, S Mantry, K Ramaesh. Tennents Institute of Ophthalmology NHS Greater Glasgow and Clyde Glasgow United Kingdom Financial Disclosures None declared for all authors Introduction Severe orbital inflammation from an infective cause is a rare ophthalmological emergency. It is often caused by progression of sinusitis or skin trauma in the form of orbital cellulitis1. The development of severe orbital inflammation from an infective cornea is rare. More commonly they progress to cause perforation and endophthalmitis. CASE SERIES Case 1 85 year old man presented with 2 days history of eye pain, reduced vision, pressure sensation and photophobia. He presented 2 days prior with a 16mm2 epithelial defect, and was treated with lubricants. Examination showed vision of light perception, near total corneal epithelial defect, conjunctival chemosis, hypopyon with corneal thinning. Day 1 Day 7 He was commenced on intensive topical antibiotics, but developed signs of scleritis after 7 days. Oral corticosteroid was commenced (60 mg) 7 days later, he developed signs of orbital cellulitis, confirmed on MRI imaging. MRI Report: “Diffuse inflammatory/infective change affecting left globe extending along intra-orbital optic nerve, with small collection related to sclera.” : Affected globe : Affected optic nerve : Diffuse inflammatory change involving optic nerve sheath : Choroidal effusion Following discussion with the microbiologist, he started a course of high dose intravenous antibiotics He showed signs of recovery after 48 hours, and was discharged home after completion of intravenous antibiotics course 5 months later, during his final clinic visit his vision remained poor at hand movements only from diffuse corneal scarring and pan ocular disruption 6 months later: thinned ectatic sclera with corneal scarring Case 2 65 year old lady presented with 2 days history of red painful eye with decreased vision. Examination showed 33mm2 corneal epithelial defect with white infiltrate, hypopyon with conjunctival injection with chemosis. Her previous ocular history includes recurrent herpetic kerato-uveitis with geographical ulceration. Eye image Day 1 5 days later, despite intensive topical treatment, she began to develop scleritis with signs of orbital cellulitis, confirmed on MRI imaging. She was commenced immediately on high dose intravenous antibiotics and topical corticosteroid. MRI report: Left sided proptosis. Diffuse thickening with enhancement of the sclera of the left globe and minor inflammation of distal optic nerve sheath… …minor thickening of left distal lateral rectus and superior palpebra superioris muscles. MRI head with contrast: Inflammatory tissue extending into post septal intra-conal space involving optic nerve sheath Day 5 Day 8 Her condition showed signs of recovery after 48 hours, and systemic corticosteroids were started after a week. She continued to improve although her vision remained poor at light perception only, from diffuse corneal scarring with pan ocular disruption. Clinic Visit 7 weeks post presentation 6 months post presentation : ectatatic thinned sclera with corneal scarring Case 3 53 year old contact lens wearer returned from holidays with a painful, red left eye with poor vision. Examination showed 34mm2 corneal epithelial defect with hypopyon, conjunctival injection and chemosis. He was commenced on intensive topical antibitiotics Day 1 4 days later despite intensive treatment, he complained of worsening pain around the orbit and had mild restriction in ocular movements. CT orbit showed signs of preseptal cellulitis. He was commenced on high dose of intravenous antibiotics. Day 4 CT Scan report: Left preseptal cellulitis ( ) 2 days later he was also received intravenous methylprednisolone. 48 hours later he showed signs of recovery, and was discharged home with intensive topical antibiotics. He was discharged home and and reviewed regularly as an outpatient. Summary Table 1: Summary of clinical presentations Age/ge nder Onset (days) Epithelial defect area (mm2) Hypopyon Chemosis Scleritis Final Visual Acuity (Snellen) 85/m 2 16 yes yes yes HM 65/f 2 33 yes yes yes HM 52/m 5 35 yes yes yes 6/36 Table 2: Summary of clinical management Topical Abx Topical steroids Systemic Abx Systemic steroids Inpatient duration Systemic history Ocular history 85/m yes yes yes yes 29 nil Idiopathic corneal oedema 65/f yes no yes yes 15 nil Recurrent herpetic keratouveitis 52/m yes yes yes yes 10 nil Contact lens wearer Discussion Severe orbital inflammation is a rare consequence of corneal ulcers1. More common consequence of corneal ulcers include corneal scarring and perforations. Endophthalmitis may occur in immunocompromised individuals. The current literature has only described one case where Pseudomonas aeruginosa associated orbital cellulitis and corneal ulcer co-existed, in a 3 month old child in 19792. The aim of our case series is to highlight our concern at disease progression despite the recommended treatment. 2 patients suffered potentially fatal complication, while 1 patient showed relatively mild symptoms. All 3 patients improved with high dose intravenous antibiotics and steroids. However, all 3 patients has poor visual prognosis following recovery. Pseudomonas aeruginosa are known to be opportunistic pathogen, with high potential for adaptability in compromised ocular environment. This quality is further enhanced by its ability to produce toxins and proteases, as well as the unique type 3 secreting mechanism as a mode of transfection3 Breakdown of its endotoxins are also believed to be pro-inflammatory, may cause severe additional local tissue immune response4 The net combination of simultaneously occurring reactions may be responsible for the intense inflammatory response. Conclusion • Clinicians should be mindful of the potential worsening progression of disease despite receiving treatment of choice • These cases are likely to illustrate the following: o New drug resistance developed by Pseudomonas aeruginosa o Secondary inflammatory mechanisms by released endotoxins • The role and interactions of systemic steroids with active infective process is unclear • Although rare, we recommend close monitoring of large Pseudomonas aeruginosa associated corneal ulcers due to its potential for worsening and intense inflammation References 1. Westfall CT. Infectious processes of the orbit. In: Albert DM, editor. Principles and Practice of Ophthalmology, 2nd edition. Kidlington, UK: WB Saunders, 2000:3121-3130 2. Weiss IS. Pseudomonas Orbital Cellulitis. American Journal of Ophthalmology. 1979 Mar;87(3):368-70 3. Kipnis E, Sawa T, Weiner-Kronish J. Targeting mechanisms of Pseudomoans aeruginosa pathogenesis. Médecine et maladies infectieuses 2006;36: 78-91 4. Sato H, Frank DW. ExoU is a potent intracellular phospholipase. Molecular Microbiology. 2004;53(3):1275-1296