Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
CONTRAST
SENSITIVITY
THROUGHOUT
ADULTHOOD
CYXTHIAOWSLEY’,ROBERTSEKULER’and DES% SIEMKS’
‘Department of Physiologic& Optics. School of Optometry Medical Center. University of Alabama
in Birmingham. Birmingham. AL 35191.
‘Cresap Neuroscience Laboratory. Departments of Psychology. Ophthalmology. and
Neurobiology & Physiology. Northwestern tiniversity. Evanston. IL 60201.
‘Illinois College of Optometry. 3241 S. Michigan Ave.. Chicago. IL 60616. U.S.A.
Abstract-Previous studies of spatial contrast sensitivity in adulthood have produced contlicting results.
To clarify the situation, we measured contrast sensitivity functions on a large sample of adults (n = 91).
ranging in age from 19 to 87. All observers were free from significant ocular pathology and were
individually refracted for the test distance. Sensitivity for stationary gratings of low spatial frequency
remtlined the same throughout ad&hood. At higher spatial frequencies. sensitivity decreased with age
finning
around 40 to 50 years. When a low spatial frequency srating was drifted. young adults’
sensitivity improved by a factor of 4-5 over sensitivity to a static gratmg: this motion enhancement was
markedly diminished in adults over 60 years. implying an impairment of temporal processing in the
elderly. Reduced retinal illuminance characteristic of the aged eye could account for a large part of older
adults deficit in spatial vision. but appeared to play little role in their deficit in temporal vision.
Contrast threshold
Acuity
Contrast sensitivity
Human aging
ISTRODUCTIOS
in recent years, the contrast sensitivity function has
become a major tool for describing human spatial
vision. Since the optical and neural characteristics of
the visual system change significantly throughout
adulthood. several studies have tried to assess how
the contrast sensitivity function (CSF) changes during
those years. This line of research is important for at
least two reasons. First. because the CSF describes
sensitivity to a broad range of target sizes, deveiopmental research on the CSF allows US to test hypotheses about how various mechanisms underlying spatial vision change throughout the lifespan. Second,
because an observer’s CSF is a good predictor of that
observer’s visual performance [Ginsburg et al., 1982).
knowing how the CSF changes with age may enable
us to predict better the daily vision problems that
older people have. We should emphasize that the CSF
gives information about visual status above and
beyond that provided by more common clinical
measures, such as visual acuity (Sekuler er rrl., 1982).
UnfortunateIy, up to now there has been no clear
description as to how the CSF changes in adulthood.
Studies have contradicted each other, in some cases
presenting widely disparate results; many are fraught
with methodological problems. In one of the earliest
reports. Arden (1978) measured contrast sensitivity to
Iow and intermediate spatial frequencies in people
ranging in age from 1I to 70 years. Spatial frequencies
were presented by photographic plates, each plate
presenting a different spatial frequency. Contrast on
the plate varied from a subthreshold level at the top
Spatial frequency
Motion
to a suprathreshold level at the bottom. Contrast
threshold for each frequency was measured by an
uncovering process, in which the experimenter slowly
uncovered the grating, exposing in~r~sin~y
higher
contrasts, until the observer said the grating was
visible. Arden reported that there were no age-related
changes in sensitivity at any of the frequencies tested.
Another paper with a similar sample (Arden and
Jacobsen, 1978) reported a slightly decreased sensitivity at older ass at each tested frequency. fn neither
study do the authors describe the number of subjects
in the various age ranges. crucial in the analysis of
developmental data. Additionally, there is no mention
whether subjects wore their best optical correction for
the test distance (50cm). Blur can significantly affect
the CSF (Campbell and Green, 1965). es~cia~~y
reducing sensitivity at higher frequencies. Presbyopia
makes refraction for the near-distance of 50cm
crucial to minimize blur during testing.
It is also unclear whether observers had eye health
examinations. In studying vision and aging, it is important to separate, as much as possible, those effects
related to ocular disease from those effects due to
aging per se. This is particularly important in studying the CSF since several ocular diseases, not uncommon in the aged, do affect the shape of the CSF (e.g.
macular disease: Sjostrand and Frisen, 1977: cataract:
Hess and Woo, 1978: glaucoma: Atkin et nl.. 1979).
Resides these methodological problems, the use of
the Arden plates to measure the CSF is problematic
in itself. First, threshotd can be crucially affected by
the rate at which the examiner uncovers the test grating. This rate may not only vary between examiners,
689
but also may vary for the same examiner on repeated
tests. Second. illumination level of the plates significantly agects threshold (&den and Jacobsen. l978t.
yet there is no standard procedure for controlling
luminance of the ptates Third. when tested with the
Arden, plates. older observers give a high number of
fabe positive responses, especially to higher frequencies (Sokol rt al., 1981). invalidating estimates of
threshold. Fourth, given the increased lenticular density and senile miosis of the aged eye. one might
expect that aider individuals may have a pronounced
fess of sensitivity at high frequencies. Yet, at recommended viewing distances. the Atden plates only
test as high as fi.Jc{drg. These factors make the
Arden plates less than ideal in the measurement of the
CSF and in the comparison of contrast sensitivity
across studies.
Two other studies have found decreased contrast
sensitivity in older observers at all frequencies tested.
Using the Arden plates. Skaika (1980) reported that
older subjects had elevated thresholds at all six frequencies tested, but did not present data separately
for each frequency and decade of age. ;McGrath and
Morrison fl98lt tested contrast sensitivity in a sample
(a = 66) ranging in age from 5 to 94 years. Gratings
were presented on an oscilloscope at a mesopic mean
luminance, 2 cd/m’. It was unclear whether observers
were screened for ocular pathologies that might agect
the CSF. The authors report an overall shift downward in the CSF with increasing age; the frequency at
which sensitivity was maximal was approxim~~tely the
same for all age groups. Reported contrast sensitivities for younger adults were unusually high for
mesopic conditions, ranging up to 1000.
Sekuler et nl. (1980) measured contrast sensitivity in
10individuals in their sixties and seventies, comparing their results to those from 25 coilege-aged indivlduals. Both young and old observers were free from eye
diseases as determined by detailed ophthalmological
exams and were in good general health. All observers
had good acuity, 20/30 or better. Older observers had
decreased sensitivity at low and intermediate frequencies compared to young observers, but had similar
sensitivity at 16c/deg, the highest frequency tested.
Similarity at high frequencies for the two age groups
is not really surprising since the two groups were very
similar in their acuity levels. If older subjects had not
been pre-screened for good acuity, individuals having
acuity worse than 20/30 (not uncommon for this age
range) would have been included in the sample.
Under these circumstances, high frequency sensitivity
in the older group would most likely have been impaired relative to the younger group.
Also of note is that the Sekuier et RI. study found
considerable individual differences in sensitivity at
low frequencies. Although the mean sensitivities of the
two age groups were fairly well separated at low frequencies, there were some older individuals whose
low frequency snsitivity fell within the range of that
of the younger group. Thus, from a sample of only 10
older observers it is dithcult to determine how preva-
lent the low spatial frequency loss actually is in the
popuIation at Iarge.
Finally. two papers have reported that aging primarily affects higher frequency sensitivitl;, with no
reduction in sensitivity at lower frequencies~ Derefeldt. Lennerstrand and Lundh (1979). presenting
gratings on an oscilloscope. measured CSFs of people
ranging in age from early childhood to their 60s.
Children and young adults had simifar CSF’s. Compared to the younger groups. observers over age 60
showed reduced sensitivity for spatial frequencies of
4c;deg and above. All observers were screened for
ocular disease and wore their best optical correction.
Arundale (1978) also found that the main difference in
CSF between young adults and older adults in their
40s to 60s was that the latter had reduced high frequency sensitivity. ~Ilthough his sample had only five
subjects in the oidest age group.
To clarify how the normal aging process affects the
CSF, we have conducted a large-sample study that is
designed to avoid many of the problems inherent in
much of the previous work. Specifically:
(1) All individuals over 60 years received a
thorough eye ~.~cttttitt~7t~ott, Ocular diseases not
uncommon in the aged (e.g. glaucoma. macular disease. cataract) can affect contrast sensitivity. Thus, it
is important to know whether differences between
contrast sensitivity in young and oider observers are
due to aging puv se. rather than ocular diseases which
happen to occur more frequently in old age. We
recognize, though, that it is difhcuft to separate biological changes that are due to old age from those
that are due to disease (Ludwig and Smoke, 1980).
Aging, according to one view, is an unidentified disease process: in another view, aging is a time-dependent process that predisposes disease but is not identical to it. Whatever definition of aging one holds, it is
reasonable to examine what kinds of changes in spatial and temporal vision might be expected throughout adulthood in cases where significant disease is
absent.
(2) All individuals wore their best possible optical
correction for rhr F@St &stctrtcc. A few other studies
have reported that observers were refracted, but, if
these refractions are to minimize blur, they must be
performed at the actual test distance. This is especially true for presbyopic observers. We cannot
assume that a refraction that optimizes acuity for 3 m
also does so at i m. Moreover, proper correction of
astigmatism in studying vision and aging is particularly important. In early adulthood the cornea’s curvature tends to be greater in the vertical meridian
(astigmatism -with the rule”); later in life the greater
curvature often tends to shift to the horizontal meridian f”against the rule”; see Weale, 1963). If astigmatism is uncorrected unambiguous comparisons of visual thresholds for young and old observers are difbcult: effects of aging per se will be confounded with
astigmatism differences between the two groups. This
691
Contrast sensitivity throughout adulthood
Table 1. Age distribution of subject sample
Age range (yrl
Sample size
19-2s
31-37
1’
6
1’
33
s
41
41-4
W-65
W-69
X-79
80437
Mean age (yr~ SD
66
74
3
3
3
3
3
,
x1
;
54
li
28
t-t
confound can be avoided by refracting subjects for
both spherical and cylindrical components.
(3) Contrast sensitivity functions were measured on
a large sample of older observers. This was to ensure
that the data woutd be representative of older individuals. rather than largely due to a few individuals
whose data might be atypical of the rest of the group.
A second goal was to measure sensitivity for mu&g
targets throughout adulthood. A number of workers
have reported that older subjects exhibit anomalous
responses to transient stimuli-moving
or flashed
targets (Kline and Schieber, l9S2; Sekuler rr al.,
1980). Parallel measures of sensitivity to moving and
static targets on the same subjects could illuminate
the connection between visual mechanisms that process temporal transients and mechanisms that process
more sustained stimuli. In addition, developmental
changes in sensitivity to motion could have considerable practical importance. Such changes in motion
sensitivity might alter visu~vestibular interac[ions in
older people and contribute to the difficulties many
older people experience in postural adjustments and
visual. guidance of locomotion (Tobis er 4., 1981).
,METHODS
Sribjecfs
Tabte 1 gives the age distribution of our subjects,
by decade, listing sample size, mean and standard deviation for each age group. Note that the sample as a
whole is weighted toward higher ages; this enhances
the generalizabitity of the findings for older subjects.
Observers age 60 and over were recruited from the
North Shore Senior Center. a meeting center for older
adults in a northern suburb of Chicago. All volunteers
came from middle income backgrounds, were healthy
and active, and lived independently in the community.
Our solicitations for participants emphasized that we
did not wish to test people who knew they had ocular
pathology. Individuats were excluded from the sample
if they reported that their own doctors had diagnosed
them as having any eye diseases such as macular disease. glaucoma, cataract, or problems associated with
diabetes.
Observers younger than 60 years were recruited
from the Northwestern University campus by means
of signs advertising the study. These observers were
for the most part university students or emptoyees
and also came from middle income backgrounds.
Volunteers were excluded from the sample if their
own doctors had diagnosed them as having eye diseases such as those mentioned above.
ilcuir.~ and refractions: older arbjects
Observers over age 60 were tested at the Senior
Center. After informed consent was obtained, each
volunteer had both eyes examined by an optometrist
IDS.), who specializes in geriatric optometry. This eye
exam included a refraction at a distance of 3 m.
using both standard subjective refraction and static
retinoscopy to determine spherical and cylindrical
components. Acuity was measured with each observer’s best correction white viewing a projected
chart (Bausch and Lomb Compact Acuity Chart) at a
distance of 3 m, mean luminance 57.6cd;‘m’ at 0.90
contrast. Funduscopy and slit lamp examination were
performed as welt as measurement of intraocular
pressure (American Optical Non-Contact
Tonometer).
In ffleneral, eye examinations were UnremarkabIe.
Most older subjects had traces of cataract. typical for
this age range (Leibowitz et al., 1980). Intraocutar
pressures were-within the normal range and are given
in Table 2 for eyes that we would later test psychophysically (i.e. the eye for each subject which had
better acuity). Only nine volunteers had potentially
serious eye problems in the eye that would be used for
psychophysical
measurements. Three had senile
macular changes which co-occurred with acuity
between 20/35 and 20/30. 5 had moderate cataract
within the line of slight. and I high intraocular pressure (over 25 mmHg). These nine subjects were eliminated from the sample since the emphasis of the
present study is on visual abilities in adults with good
ocular health. Those individuals with eye problems,
not currently under medical supervision, were referred
to their own doctors.
Acuity and refraction: younger subjects
Observers under age 60 were tested in the Vision
Laboratory on Northwestern’s Evanston campus. Eye
health was not evaluated in these subjects by our
optometrist, but they were all refracted for the test
distance. All observers were free from eye disease as
determined by their most recent eye exam by their
own eye care specialist (on the average, 2 years before
our test date). As with the older group. acuity was
measured while subjects wore their best optical correction. Acuities were taken with the Bailey-Lovie
distance chart at 3 m (Bailey and Lovie, 1976). The
chart had a mean luminance of 2OOcd/m’. presented
Table 2. Intraocular pressure (mmHg) for eye tested
Age group fyr)
60-69
70-79
80-87
mmHg
SD
17.7
3.7
3.9
3.2
16.2
18.9
CYXTHIA OU.SLEY er al
693
at a contrast of 0.90. Both the Bausch and Lomb
Compact Acuity Chart. used to measure acyity in
older subjects. and the Bailey-Lovie chart employ the
Sloan optotypes (see Sloan. 1959).
Pupil diameters were also measured for aI! subjects.
Diameters for subjects over age 60 were measured to
the nearest 0.1 mm with the reticule of a slit lamp. For
younger adults. diameters were measured to the nearest 0.5 mm with a small rule while viewing the display
used for contrast sensitivity testing (103 cd/m’). Since
pupil size for young and old observers was measured
under luminance conditions not strictly comparable
to each other, we will be unable to make direct comparisons between the two age groups on this variable.
Contrast
smsitirit_v
mmurrrnmts
Contrast sensitivity was measured by an Dptronix
Vision Tester (Model 200) a pre-programmed. microcomputer-controlled
television display. Stimuli were
static sinusoidal vertical gratings of the following spatial frequencies: OS, I, 2, 4. 8. 16cideg. presented in
that order. The display subtended a visual angle of
4.2 x 5.5 deg at the test distance of 3 m. Mean luminance of the screen was held constant at 103cd/m2.
Surround luminance was 2 cd/m’.
A tracking procedure, based on von Bekesy’s
audiometric method, was used to determine contrast
threshold for each frequency (Sekuler and Tynan,
1977). This procedure was selected because previous
work indicated it to be a rapid and efficient way to
measure visual thresholds in older observers (Sekuler
rt CJI.,I980). Contrast was defined as the difference
between maximum and minimum luminances, divided
by their sum. A grating was initially presented at a
suprathreshold contrast (0.20) for 1 set so that the
observer would know what pattern wou!d appear
during the tracking procedure. This preview was
designed to minimize the effects of spatial frequency
uncertainty (Davis and Graham, 1981). After 3 set of
blank screen, a high tone indicated that testing was to
begin. The test grating was initially presented at a
randomly selected subthreshold contrast and then
was gradually and steadily increased by the computer.
Table
3. Mean acuity and optical correction for eye tested
Acuity*
Age (yr)
20s
30s
40s
50s
60s
705
80s
Walk-in
0.91
0.79
0.92
1.3 I
I.55
I .73
2.20
At the beginning of the test. contrast was increased
starting from some randomly selected value between
0.0 and 0.002. It took 34s~ to span the entire contrast range, with maximum contrast set at 0.2. Contrast (C) at any given moment in the 3Csec interval
was defined as follows: C = Itij825. where T is time
in seconds. Since the rate OF contrast change was not
linear. we present those rates that cover the contrast
range within which measured thresholds fell. For
example, around a contrast of 0.01, contrast changed
at a rate of 0.1 log unit&c; around a contrast of 0.1,
contrast changed at a rate of 0.035 log unitisec.
The observer depressed a button when the pattern
became visible on the screen, signalling the computer
to decrease contrast. The observer was instructed to
keep the button pushed as long as the grating was
visible, and then to release the button when the pattern became invisible. The button’s release signalled
the computer to increase contrast, and the cycle
began again. This procedure terminated after 8 reversals of contrast. Contrast threshold was defined as the
geometric mean of the 8 reversals and was determined
in the same way for each of the 6 spatial frequencies.
Contrast sensitivity is defined as the reciprocal of the
threshold contrast. Before beginning the actual test
sequence, all subjects were given practice in the task,
by running through the tracking procedure for 1 and
8 c/deg.
After the contrast sensitivity for the six static gratings had been determined, contrast sensitivity was
measured for a grating of f c/deg that moved horitontally at !.I deg/sec and for the same grating moving at
a higher speed, 4.3 deg/sec. The tracking procedure
was again used to determine contrast threshold.
Monocular contrast sensitivity for static and moving gratings was measured using the eye with the
better acuity (best~orrected). Observers either wore
their own correction, if this was the best refraction, or
viewed the display through trial lenses positioned in
trial clips (Keeler) or frames (Bernel!). The untested
eye was occluded with a black, opaque patch. The
right and left eyes were tested with about equal Frequency in each age group.
Best
Sphere+
0.68
0.19
0.78
I.27
I.38
- 2.27
-0.96
- 1.13
-0.20
f I.04
+0.71
I .Y2
+ 2.04
1.07
Correction
With rule:
Cylinder?
astig. (%J
-0.1 I
- 0.46
-0.32
-0.s.5
-0.76
- 0.95
-0.86
Against rule
astig. (“A)
8
16
50
13
60
12
32
0
33
25
20
61
65
100
*Minimum angle resolvable.
t Diopters.
:Not all subjects had astigmatisms as defined (see text) so the two percentages for each age group do not
sum to 100.
Contrast sensifkity throughout adulthood
Fromtngham
.
Burg-
+
Burg-screen
A
Wvymouth-
senan
l
Kornzwerq
*)f 01
0
Chapants
study
orrnoratar
20110
-
20114
-
2Ofl6
I.C
-
20120
O,&I-
-
2Of25
0.6
-
20130
0.4I-
-
20150
0.2I_
-
20/100
I .4
1.2
5
._
0
E
‘L;
A
-
I6
2
693
x
Donders
0
Milne
t*st
- scrsen
-screen
and
screen
test
is?
test
Williamson
test
0”
&
7ii
tz
01I
-
0
I
I
I
I
I
I
I
IO
20
3C
40
50
60
70
I
80
201200
I
90
Age
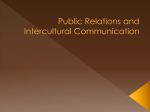
Fig. 1. Mean acuity as a function of age. Acuity is expressed in terms of decimal acuity (left) and SneHen
acuity (right). Solid line represents data from the present study; shaded areas represent two standard
errors above and below the mean. For comparison. data from other studies are also plotted (borrowed
from Pitts, 1982).
RESULTS
Table; 3 presents for each group, means for
“walk-in” acuity (observers wearing their own correction) and best-corrected acuity. Acuity is expressed in
terms of minimum angle resolvable (MAR). The acuities of all age groups, except the 30-yr-olds, could be
improved by a change in their correction, if they had
one, or by the introduction of a correction. We were
able to improve acuities of older adults somewhat
more than for younger. Also listed in Tabie 3 are
mean spherical and cylindrical corrections and the
percentages of observers having astigmatism at or
around the two major meridians (90 and 180 deg). We
include the astigmatism data because it illustrates the
shift toward “against the rule” astigmatism in later
life.
Best-corrected acuity declined from the 20s to the
80s. except for a period of apparent stability in the 30s
and 40s. Figure I presents mean acuity as a function
of age (solid line), along with the results of earlier
studies {as given by Pitts, 1982)J for comparison.
Pitts summarized the earlier studies by expressing
acuity in terms of decimal acuity (left) or Snellen
notation (right): thus, our data is also presented in
this manner. While our data for age 50 and over agree
very well with the previous studies, our estimates of
acuity in the 20s through 40s are generally higher
estimates from the previous work. Individuals in
their 20s in our sample have a mean acuity of 20/ I5
The shaded area around our data (solid line) rep
resents 2 standard errors above and below the mean.
Although it appears that variabiiity in acuity decreases with age, this decline is an artefact of expressing resolution in terms of decimal acuity. When acuity
is expressed in terms of minimal angle resolvable,
variability actually increases with age, as is the case in
other measures of visual performance.
Despite the aforementioned problem in directly
comparing pupil size for young and older adults in
our sample, our pupil diameter data, listed in Table 4,
do conform to the general finding that pupil diameter
decreases with age (Loewenfeld, 1979). In our sample,
the correlation between age and pupil diameter was
-0.70 (right eye) and -0.68 (left eye). Sekuler (1982)
than
Table 4. Mean pupil diameter by age
Age group(yr)
Pupil diameter
SD
19-28
31-38
41-48
W-58
60-69
XI-79
80-87
5.3
4.0
3.8
3.0
3.2
2.1
2.8
0.8
0.0
1.0
0.5
0.5
0.5
0.6
Z c deg. older
Lsoo
t
200 -
subjects
statistically
sensitivity.
which
more
increasing
age:
severe
with
P = 0.029:
F(6.81) = 2.49.
P c 0.0001:
100 -
exhibited
cant losses in contrast
16c’deg.
S c/deg.
s
IO5
to 20 deg. The
amount
shifts and the age at which
has shifted
by which
from our data. Our sampling
frequency
continuum
steps)
that
was
our
from
the peak
the shift begins are difficult
to estimate
octave
of the spatial
sutlicienttv
ability
peak of the CSF is somewhat
1
= 9.83.
P < 0.0001:
F(6.71) = 7.65. P < 0.0001.
4c!deg
20's 30's 40'S -JO'% I....
60's -TO's '\60'*-.-
Zc;deg.
F&SO)
1) = 7.32.
By the 60s. the peak of the CSF
r JO:
z
'-2 20-
for
4c,deg.
f(6.8
signifi-
are in general
coarse
to identify
limited.
(one
the exact
as is our ability
to detect shifts of that peak.
Spatial
Frequency,
c/deg
Fig. 2. Mean contrast sensitivity at each tested frequency
by age group. The standard error of the mean was approximately the same across age groups at law spa&d frequencies. about 0.05. At higher spatial frequencies. data were
more variable within the older age groups than within the
younger; e.g. at S cideg. SEM = 0.13 for 70-yr-olds and
SE&I = 0.05 for 20-yr-aids. See T;tbles I and 5 for more
detailed information.
reported
a similar
independent
correlation.
-0.70.
in
Spatial contrast sensitivity
is not only related to
age. but also to acuity (best-corrected). Showing CSFs
stratified by acuity without regard to age, Fig. 3 illustrates this relation.
Acuity level has a significant effect
on contrast sensitivity for spatial frequencies Zc/deg
and above.
Subjects
least
in
the acuity
Previous
quency
work
shows
when
on log-log
coordinates
trast sensitivity
at each frequency
trast sensitivity
is defined as the reciprocal
threshold.
To assess the effect
mean con-
by age group.
Con-
of contrast
of age for
each
fre-
quency, a one-way analysis of variance was computed
on log thresholds. Table 5 presents by age group
mean
log
threshold
each spatial
At
and
frequencies
of
it
is
for
and
I c/deg.
for 0.5 cideg.
age
has
no
f(6.8 I) = 0.54,
F(6.81) = 0.46, P = 0.839.
At
however, there is a decrease in sen-
I @deg.
higher frequencies,
sitivity
deviation
beginning
around
40 to 50 years. Starting
at
in this range.
tend to be less sensitive
range
examined
in
the
present
with
that
gratings
modulated
can
take
of
low
spatial
temporally.
the form
This
of either
temporal
flicker
0.5
1.0
2.0
4.0
X.0
16.0
hl
SD
x1
SD
hl
SD
M
SD
M
SD
M
Sf>
20s
30s
- f.433
0.171
- 1.972
0.155
- 2.373
0.18-i
- 2.399
0.183
- 2.045
0.155
- f .-I67
0.225
- I.322
0.196
- I.881
0.218
-3.193
0.218
- 2.207
0.163
- t.95
0.100
- I.293
0.155
or
to sensitivity
presented
defined
ratio
1972). Since temporal
(Kelly,
the amount
of contrast
contrast
culated
to the same grating
stationary.
when
40s
- 1.354
0.100
- I .a43
0.1 I2
- 2.247
0.133
-2.213
0.1 IO
- t .99Y
0.156
- I .289
0.188
of temporal
sensitivity
enhancement
for the moving
we
as the
grating,
to
for the stationary grating. We calthe temporal enhancement in this way for
sensitivity
50s
f .401
0.177
-1.016
O.!Y3
- 2.369
0.097
- 2.369
0.082
- 1.852
0.136
- I.138
0.371
-
it was
For each rate of movement,
Table 5. Mean fog contrast threshold by age group
Cycle,‘degree
fre-
becomes easier to see
a grating
m~ulation
enables the grating to be seen at reduced contrasts,
modulation can be thought of as enhancing sensitivity
to the target. We examined temporal enhan~ment of
sensitivity at various ages. Sensitivity was measured
for a 1 c/deg grating moving at both 1.1 and 4.3 deg/
sec. Sensitivities for these moving gratings were commo~‘ement
pared
0.5
inff uence on sensitivity:
P = 0.777;
its standard
frequency.
acuities
study.
modulation
Figure Z displays
poorer
to targets of higher frequencies. Sensitivity
to low frequencies (0.5 and I c,‘deg) is unaffected by acuity, at
another,
sample.
P c 0.03 for all frequencies
with
60s
- f ,389
0.202
- I.912
0.201
-2.164
0.23 I
- 2.050
0.181
- 1.707
0.392
-1.047
0.400
70s
-
1.420
0.15Y
- I.940
0.237
- 2.042
0.265
- 1.889
0.349
- 1.468
0.403
-0.874
0.3 I I
80s
- f .433
0.190
- 1.946
0.246
- 2.062
0.353
- 1.747
0.328
- f.360
0.460
-0.709
0.372
Contrast snsrti\itv
throughout
695
aduithood
Reduced retinal illminance
SO0
( 1963) has estimated that the average 60-yr-
Weale
t
old eye transmits
200
transmitted
t
largely
approximately
by the average
due to two optical
1963): a reduction
increased
lowered
tivity
density
retinal
we were
quency
size (“senile
spatial
interested
reduces
frequencies
in how
loss in our older
table to the reduced
much
First,
retinal
we re-measured
seven young
AI*91
This
t
I
factor
I
I
I
I
I
1
0.S
I
2
4
8
16
Spatial
frequency,
filter
both pupil
size under
the estimated
c/deg
and Weale.
Fig. 3. khan contrast sensitivity at each tested spatial frequency by acuity (minimum angle resolvable). Each curve
represents the mean contrast sensitivity of individuals with
acuity in a certain range. These ranges are indicted by the
minarc values printed to the right of each curve. Each
minarc value represents the maximum of its range; from
top to bottom. the ranges are 0.50-0.75, 0.76-1.0, l.lO-1.25.
1.~5-1.50, 1.51-1.75. and over 1.75.
did
not
young
Fig.
results for
4. First.
hancement
rates for each subject. The
each age group
both
are
portrayed
in
rates of movement
produce
en-
significantly
above
the no-enhancement
line in Fig. 4 (P c 0.001). Second,
hancement
produced
I.1 deasec,
slightly
this decrease
the amount
by the slower
rate
enhancement
reach
statistical
for younger
pronounced
adults.
on
temporal
which
function
linear component.
accounts
for
the
en-
is diminished
ratic and cubic
functions
appreciable
for 4.3 deg/sec has a
The best fitting
32% of the variance
(P c 0.001). We also computed
an
in
respectively.
the best fitting
but
over
the temporal
the
the faster rate of movement
with
age.
Contrary
to an earlier report
as linearly
(Brabyn
linear
fit,
at any
gratings
tested
for
associated
declining
in contrast
stationary
of
(P > 0.15 for all tested spatial
fre-
quencies and movement
frequency
then,
and McGuin-
ness, 19793 there were no sex differences
younger
quad-
approximation,
enhancement
with
moving
data
they did not represent
improvement
At feast to a first
we can describe
sensitivity
straight
the
for 3%/, and 41% of the data’s variance.
accounting
and
be emphasized
Instead,
(Said
that
directly
we estimated
for the two age groups
we
in our
reti-
using Said and
density for
density
and
the
groups,
we chose a neutral
the
pupil
size estimates
estimated
for
density
retinal
subjects to the estimated
filter
two
age
(0.5) which
illuminance
of
the
level of the older sub-
jects.
Figure
5 presents
the mean CSF for the 20-yr-olds
viewing
with a filter, their
viewing
(no filter).
olds.
As
would
mean
CSF
and the mean CSF
be expected
1972). reduced retinal
from
with
regular
for the 60-yrprevious
iilumjnance
work
selectively
z-s
f
.?-
.z
5-
s
'i; 4-
E
The age-by-sensitivity
line
conditions
fo:. 20-yr-olds
illuminance
a
account
significance,
effect
for older adults.
significant
density
into
the lenticular
(Kelly.
for the faster rate (4.3 deg/sec) of move-
P c O.OOOI. with
hancement
filter.
by
decreases in the 70s and SOS, but
does not
P c 0.12. Age does have a significant
ment,
of en-
of motion,
taking
Weaie’s measurements (1959) of lenticular
brought
each of the two movement
density
illuminance
adults in their 20s and 60s. Then, given
young
mean
retinal
and old observers.
functions
age = 23) as they
these luminance
retinal
fre-
be attribu-
characteristic
a 0.5 neutral
1959). It should
nat il~uminance
1972).
sensitivity
three,
lenticular
measure
sensi-
might
(mean
their
of approximately
contrast
this issue in two ways.
contrast
through
reduced
and
(e.g. Kelly.
illuminance
observers
viewed the display
2
is
lens. Since
of the higher
observers
of the older eye. We addressed
for
This
miosis”).
of the crystalline
illuminance
to higher
the light
eye.
changes in Iater life (Weale.
in pupii
optical
one-third
IO-yr-old
rates). This was true for both
and older adults.
5
4.3
3-
2
i
2'1.1
.-:
1
%
deg/ set
----_______
No enforcement
I
i
I
I
I
I
I
20
30
40
50
60
70
80
Age
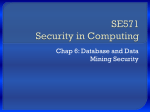
Fig. 4. Mean sensitivity enhancement as a function of age
for a 1 c/deg grating drifting at either 4.3 or 1.1 deg/sec.
Each point is the mean ratio between sensitivity to a moving I #kg
grating and sensitivity to the same grating
presented stationary. The upper curve shows sensitivity enhancement with movement of 4.3 degisec; the lower curve
shows sensitivity enhancement with movement of I.1 deg:
sec. The dashed horizontal line indicates what would be
expected if there were no enhancement.
CYSTHIA
0.5
I
Spatial
2
4
e
frequency,
Ows~Ev ef al.
16
c/deg
Fig. 5 Mertn contrast sensitivity for 20.yr-olds with regular
viewing: these same individuals wearing a 0.5 neutral density filter: and older observers in their has with regular
viekng. The neutral density After worn by young observers
reduced their retinal illumkmce to the cstimnted level of
60-yr-old observers.
illuminance difference we have assumed between
young and old observers.
We were also interested in the role of reduced retinal illuminance in the temporal enhancement effect.
Recall that for young observers, sensitivity to a
1c/deg grating was enhanced when it drifted’ at
4.3 deg/sec, although observers over age 60 exhibited
little increase in sensitivity. TO assess whether this age
difference was due to reduced retinal illuminan~ in
older observers. we re-measured temporal enhancement in seven of our younger observers (mean
age = 23) while they viewed through a 0.5 neutral
density filter (that reduces retinal illuminance by a
factor of 3; see above). As for the originai condition,
contrast thresholds were obtained for a stationary
I c/deg grating and 1 c/deg grating drifting at 1.1 deg/
set and 4.3 deg/sec. Temporal enhancement for young
adults was unchanged when their retinal illuminance
was reduced to a level similar to that of the aged eye.
This result is consistent with Kelly’s work (I972) on
the effects of luminance on detection of temporallymodulated gratings. Our findings suggest that the low
level of temporal enhancement in observers in their
60s is not attributable to reduced retinal illuminance.
Correlational
depresses sensitivity for higher spatial frequencies.
Figure 5 suggests that when retinal itluminance is
roughly equalized for 20-yr-olds and 60-yr-olds, the
sensitivity difference between the two age groups is
minimized. The residual difference between old and
young is non-significant
at 4 and Yc/deg. but
approaches significance at 16 c/deg (0.05 c P c 0.10).
it appears, then. that a signi~c~lnt portion of the sensitivity loss at intermediate and high spatial frequencies
is attributable to a retinal illuminance reduction in
the aged eye.
A second way in which we evaluated the role of
reduced retinal ifluminance in the young-old sensitivity difference is by applying the DeVries-Rose law
(see Kelly. 1972. 1977). In our context, the DeVriesRose law implies that detection thresholds for spatial
frequencies of 4c:‘deg and above should be directly
proportional to the square root of the adaptation
level. Following Weale (19631, we assumed that our
GIFyr-olds received one-third the retinal ~lluminance
of young adults (10-yr-olds). We found that for the
60-yr-olds the obtained thresholds at higher spatial
frequencies were slightly higher than those predicted
by the DeVries-Rose law. More specifically. at 4 and
8 c,deg. the 60-yr-olds‘ obtained thresholds were 0.09
fog unit higher than those predicted by the DeVriesRose law; at 16~ deg. their obtained thresholds were
0.17 log units higher than those predicted. Agreeing
with the control experiment with young subjects mentioned above, the DeVries-Rose analysis suggests that
much of the sensitivity loss of older adults at higher
spatial frequencies is attributable to reduced retinal
itluminance of the aged eye. Of course the accuracy of
the predictors discussed here depends upon the retinal
analysis
Pearson Product Moment Correlations were computed among the following variables: age, best-corrected acuity (MAR) for the eye tested psychophysitally, log threshold for stationary gratings of 0.5, 1, 2,
4, 8, and 16c/deg, and 1c/deg grating drifting at 1.1
and 4.3 deg/sec. Table 6 presents the matrix of resulting correlations.
Several aspects of the Table 6 mirror results already
discussed and shown in Figs 2 and 4. First, age was
positively related to minimum angle resolvable, with
younger adults resolving smaller angles. Second, for
spatial frequencies of 2 c/deg and above. age was positively related to log contrast threshoid. Older observers tended to have higher thresholds to frequencies 2 c/deg and above than did young observers.
Age and threshold for the more slowly moving
grating were positively related, but there was a
stronger positive relation between age and threshold
for the same grating drifting at the higher rate
(4,3c/deg); older observers tended to have higher
thresholds for this moving target.
Now we turn to two features of Table 6 that are not
anticipated by our earlier presentation of results.
First, note that thresholds for static gratings of similar
spatial frequency were correlated. Although the strongest correlations were generally between gratings
closest in spatial frequency, significant correlations
were found between gratings separated by as much as
two to three octaves. For example, the threshold for a
grating of 2c/deg correlated significantly
with
thresholds for all other spatial frequencies tested.
Second, MAR was positively correlated
with
thresholds for gratings whose spatial frequencies were
as low as 2 cjdeg and on up to 16 c/deg.
Contrast
Table
sensitivity
6. Pearson
throughout
adulthood
product-moment
correlations
Stationary
Age
0.75
-0.05
- 0.08
0.31
0.60
0.57
0.61
0.27
0.53
MAR
0.5 c,‘deg
1c,‘deg
2 c;deg
4 c!deg
8 c:deg
16 c/deg
I. 1deg,kec
4.3 deg,kec
MAR
0.5
-0.16
-0.08
0.33
0.59
0.56
0.58
0.11
0.50
1.0
0.5l
0.28
0.11
0.02
-0.07
0.18
0.15
0.62
0.37
0.20
-0.09
0.42
0.38
697
2.0
0.77
0.46
0.30
0.54
0.72
(c-dcg)
4.0
0.15
0.48
0.45
0.74
8.0
0.55
0.33
0.5 1
16.0
0.24
0.47
Moving
(deg jet)
I.1
0.59
For r > 0.26. P -C 0.01: for r > 0.20, P c 0.05.
We should
does
point
not exhaust
out that
this correlational
analysis
the information
content of the variance-covatiance
structure
of our results. In fact, elsewhere we have used our variance-covariance matrix
as the basis for a linear structural
model of the neural
mechanisms that support the CSF (Sekuler et al., submitted manuscript).
DISCUSSION
This
mine
investigation’s
major
purpose
was
to
deter-
how the aging process throughout adulthood
affects spatial vision, as described by contrast sensitivity measurements. We have found that from the 20s
to the 80s. there is a decrease in contrast sensitivity
for intermediate and high spatial frequencies that
becomes more pronounced with age. Contrary to
some previous reports, low frequency sensitivity was
unchanged throughout adulthood (McCirath and
Morrison, 1981; Sekuler et al., 1980; Skalka, 1980;
Arden and Jacobsen, 1978). Our data are in good
agreement with those of Derefeldt et al. (1979). As in
the present investigation. they insured that observers
had good eye health and wore their best optical correction for the test distance.
In addition, our study provides support for the
suggestion that older adults have an impairment in
the processing of temporally-modulated targets (Sekuler et al., 1980; Kline and Schieber, 1982). Although
movement does enhance sensitivity to a 1 c/deg grating for observers of ail ages, the amount of the enhancement declines markedly with age. Control
measurements indicated that this visual deficit could
not be attributed to the reduced retinal illuminance of
the aged eye. Further work must explore the extent of
the elderly’s impairment in processing time-varying
targets. by examining their sensitivity to a wider range
of temporal frequencies for both flickering and moving targets.
Our data indicate that a significant portion of older
adults’ sensitivity loss for intermediate and high spatial frequencies can be attributed to retinal illuminante differences between the two age groups. This
does not. however. preclude some levet of neural involvement in the spatial visual deficits. In the present
study, we reduced retinal illuminance in young observers to the estimated level of that of 6%yr-olds.
Future work on the role of iliuminance reduction in
older adults’ spatial visual deficits should measure
retinal illuminance directly for each subject. thereby
avoiding iiluminance estimates based on an entirely
different group of individuals. This would allow retinal illuminance to be more precisely equalized for the
young and old age groups when their contrast sensitivity is measured. An alternative way to assess the
role of retinal illuminance in the age-related loss in
contrast sensitivity is to compare contrast thresholds
for older adults who are aphakic to older adults who
are not. Since the crystalline lens in the aphakic individuals has been removed, they are immune to the
light reduction associated with the aged lens.
What other factors, besides a retinal illuminance
reduction, might underlie these visual deficits in older
observers? Both young and older observers wore their
best optical correction for the test distance so it is
unlikely that enough blur existed to hamper target
detection. It might be suggested that the increased
light scatter ~haracterjstic of the aged eye (Alien and
Vos, 1967; Wolf and Gardner, 1965) is responsible for
threshold differences between young and old observers. The increased forward scatter of light can be
thought to act as a veiling luminance on the retina
(Stiles, 1928; Fry, 1954), thereby increasing the mean
luminance and decreasing the contrast of art!. pattern
imaged on the retina. Because it would reduce the
effective contrast of any pattern, thresholds for targets
of all spatial and temporal structures should be elevated to the same degree. For this reason, it seems
inappropriate to hold increased light scatter in the
older eye responsible for the young-old threshold differences, since these threshold differences are specific
to certain spatial and temporal characteristics.
Specifically, older observers’ thresholds are greater
than those of young observers for spatial frequencies
above 2 c/deg onty, and for faster (4.3 degjsecl but not
slower (I.1 deg/sec) drift rates. Therefore the agerelated effects cannot be explained on the basis of
scattered light.
Because optical factors appear to have little or no
role in the temporal visual deficits reported here. we
698
CYN,.“IA
OWSLEY
are led to believe that neural changes in the visual
system play an important role. Whethit. neural
changes have any role in spatial visual deficits found
in the elderly remains to be determined. There does
exist a technique to measure directly the role of
neural factors in the contrast sensitivity. Sinusoidal
gratings of various spatial frequencies can be generated on the retina using laser-produced interference
fringes which by-pass the optics of the eye (Campbell
and Green, 1965). Therefore. under these conditions
the CSF represents neural influences alone. Dressier
and Rassow (1981) adapted this technique for clinical
use and measured “neural” CSFs on a sample of control subjects representing a range of ages (I2 to 7 I
years). Although they report that all their subjects had
normal eye health, they do not present the clinical
protocol and results that support this conclusion.
Dressier and Rassow note that they found no change
in neural sensitivity with age. but do not present the
data statified by age, nor do they present sample sizes
by age group. Kayawaza et al. (1981), in a similar
study, also make reference to there being no age effect
in neural sensitivity, but also fail to report important
details for interpreting their findings. Under these circumstances. one should be particularly careful about
accepting the null hypothesis of no change in neural
sensitivity in old age. In view of these considerations,
we believe that the role of aging in neural sensitivity
deserves further study.
It has been maintained that an observer’s acuity is
not predictive of sensitivity to low and intermediate
spatial frequencies (Ginsburg, 1980). Ginsburg has
reported that normal acuity involves the processing of
high spatial frequencies from 18 to 30c/deg and that
acuity reveals nothing about sensitivity to frequencies
below 18 c/deg. Figure 3 shows that for individuals in
good ocular health the shape of the CSF is quite
obviously related to acuity. Better acuities are associated with a generalized decline in sensitivity for frequencies 2 c/deg and above, which was also confirmed
by our correlational analysis.
Our subjects came from middle income backgrounds and had life-long access to health care services and good nutrition, making our subject sample
rather selective. This type of sample was chosen so
that we could demonstrate that even during “optimal”
conditions in a lifetime, visual impairments besides
the known optical and acuity problems, can develop
in later years. Although our data are not “normative”,
they are certainly representative of a large number of
individuals in the United States.
Even though our older adults were free from
serious eye conditions such as macular disease, glaucoma, advanced cataract, and diabetic retinopathy,
they still exhibited substantially elevated contrast
thresholds. This fact suggests that these threshold elevations may be best attributed to factors associated
with the normal aging process. rather than to
advanced stages of eye diseases known to affect contrast sensitivity. As mentioned earlier, this distinction
er d.
may be somewhat precarious [Ludwig and Smoke,
1980): yet we would like to underscore that the impairments in spatial and temporal vision reported
here appear to be frequent concommitants of the
aging process. even for those individuals who would
be considered to be in good ocular health.
~cP,lolrIrdyenrrncs-This
research was supported
by a
grant from the National Institute on Aging I.AG-EY 01251)
to Northwestern
University. We are grateful to the staff
and membership of the North Shore Senior Center. Winnetka. Illinois for their generous cooperation.
We thank
Michael Sloane. Phillip Russell and Patrick ‘Mulvanny for
helpful discussion. and two anonymous
reviewers for
insightful comments.
REFERESCES
Allen M. and Vos J. J. (1967) Ocular scattered light and
visual performance as a function of age. &I. J. Optom.
Ph.k?l. Opt. 4-4. 7 17-727.
Arden G. B. (1978) The importance of measuring contrast
sensitivity in cases of visual disturbance. Br. J. Ophrhal.
62, 198-209.
Arden G. B. and Jacobsen J. tl978) A simple grating test
for contrast
sensitivity:
Preliminary
results indicate
value for screening in glaucoma. Iprrest. Op/rt/~al. Yisctal
Sci. 17, 23-32.
Arundole K. (1978) An investigation into the variation of
human contrast sensitivity with age and ocular pathology. Br. J. Opl~rlrnl. 62, 2 13-ZIS.
Atkin A.. Bodis-Wollner
1.. Wolkstein
M.. Moss A. and
Podos S. (1979) Abnormalities
of central contrast sensitivity in glaucoma. ilrli. J. Opbdlcll. 88. 10s?I I.
Bailey 1. L. and Lovie J. E. (1976) New design principles of
visual acuity letter charts. itru. .I. Oprorn. Plry~iol. Opt. 53,
7-Q-745.
Bodis-Wollner
1. and Camisa J. (1980) Contrast sensitivity
measurement in clinical diagnosis. ~Vr~rro-opltrhrrlmolog~.
Excerpta Medica. Amsterdam.
Brabyn L. B. and McGuinness
D. (1979) Gender diHerences in response to spatial frequencies and stimulus
orientation. Percept. Psyhoph,n.
26, 3 19-324.
Campbell F. W. and Green D. G. (1965) Optical and retinal factors aRecting visual resolution. J. Physiol. 181,
576-593.
Davis E. T. and Graham N. (198 I) Spatial frequency uncertainty etfects in the detection
of sinusoidal gratings.
Vision Res. 21. 705-712.
Derefeldt F. D.. Lennerstrdnd G. and Lundh B. (1979) Age
variations in normal human contrast sensitivity. Acra
ophrhctl. 57. 679-690.
Dressler M. and Rassow B. (1981) Neural contrast sensitivity measurements with a laser interference system for
clinical screening application. I~rx~r. Oplrrlr~l. risucrl Sci.
21. 737-74-L
Fry G. A. (19%) A re-evaluation of the scattering theory of
glare. Illurn. &//I
Sfx. -19. 98.
Ginsburg A. P. (1980) Specifying relcvnnt spatial information for image evaluation
and display design: An
explanation
of how wc see certain objects. Proc. Sot.
Irr/orrtr. Di.\pkn 21. 319 227.
Ginsburg A. P.. E\uns D. I?.. Sshulcr R. and Harp S. A.
llVX2) Contrast scnsiliiitr predicts pilots’ oerformance in
aircraft
simulalors.
:l,,r.- 11. O,j,on,. Phhiol.
Opr. 59,
105-109.
Hess R. and Woo G. (1978) Vision through cataracts.
ftrrrsr. Ophhd.
risd
Sci. 17, 428-436.
Kayazawa
F.. Yamamoto
T. and ltoi M. 11981) Clinical
measurement of contrast sensitivity function using laser
generated
sinusoidal
grating.
Jup. J. Ophrhl.
25,
229-236.
Contrast sensitivity throughout
Kelly 0. H. (I9721 .\daptation effects on spatio-temporal
sine-wave thresholds. i’ision 5e.s. II. S9- 101.
Kelly 0. H. II9771 Visual contrast sensitivity. Opt&r .-lcrq
24. 107-129.
Kline 0. W. and Schieber F. J. 11982) Visual persistence
and temporal resolution. In .+/iog in Htrrnctn l’isuctl
Funcrions (Edited by Sekuler R.. Kline D. W. and Dismukes K.). Liss. Teu York.
Leibowitr H. M.. Krueger
E.. !&under
L. R.. Milton
R. C.. Xlohandes St. K.. Kahn H. A.. Nickerson R. 1..
Pool J.. Colton T. L.. Ganley J. P.. Loewenstein J. I. and
Dawber T. R. The F~lmingham eye study monograph.
SMr. 0$)&t/. (.%,$.) 24. 335-610.
Loewenfeld 1. E. [ 19i9) Pupillary changes related to age. In
7”opics ill .L’urrro-Oplrtktr~rrto/o~~~ (Edited by H. Stanley
Thompson). Williams & Wilkins. Baltimore.
Ludwig F. and Smoke M. E. (1980) The measurement of
biological age. &.ypI .-lyirr(/ Res. 6, 197-522.
McGrath C. and Morrison J. D. (1981) The effects of age
on spatial frequency perception in human subjects. Q. J.
r.xp. Ph,wiol. 66. ‘53-26 I.
Pitts D. G. (1983) The effects of aging on selected visual
functions: Dark adaptation. vis,uaI acuity, stereopsis and
brightness contrast. In Ayirry in *Hutwn Vistrd furtcrions
(Edited by Sekulsr R.. Kline D. W. and Dismukes K.).
Liss. New York.
Said F. S. and Weals R. A. (1959) The variation with age of
the spectra) transmissivity of the living crystalline lens.
Gero~trnl~/itr 3, 2 13-23 I.
Sekuler R. (1982)Vision as a source of simple and reliable
markers for aging. In Bioloyicd
Markers
oj’ Aging
(Edited by M. E. K. and E. L. Schneider). U.S. Government Printing Otlice. Washington. DC.
adulthood
699
Sekuler R.. Hutman L. P. and Owsley C. (198.0) Human
aging and spatial vision. Science 209. Il55-1256.
Sekuler R.. Owsley C. and Hutman L. P. (1982) Assessin
spatial vision in older patients. Am. J. Optom. Ph~.siol.
Opt. 59.961-968.
Sekuler R. and Tynan P. (1977) Rapid measurement of
contrast-sensitivity functions. ,.mr. 1. Oprom. PhFsiol. Opr.
54.573-575.
Sekuler R.. Wilson H. and Owsley C. Structural modeling
of spatial vision. Vision Res.
Sjostrand J. and Frisen L. (1977) Contrast sensitivity- in
macu)ar disease. A preliminary report. ,4crr1 ~~p~rr~lu~.
55.
506-514.
Skalka H. W. (1980) Effect of age on Arden grating acuity.
5r. J. Opthul. 64, 21-23.
Sloan L. L. (1959) New test charts for the measurement of
visual acuity at far and near distances. Am. J. Ophrld.
48, 807-8 13.
Sokol S., Domar A., Moskowitz A. and Schwartz (1980)
Utility of Arden grating test in glaucoma screening: high
false positive rate in normals over 50 years of age. Incest.
Ophthal. cisual Sci. 19, 1529-1533.
Stiles W. S. (1929) The scattering theory of the effect of
glare on brightness difference threshold. Proc. R. Sot.
Ser. 5 t05, 131.
Tobis J. S.. Nayak L. and Hoehler F. (1981) Visual perfeption of verticality
and horizon~lity
among elderly
failers. Archs Phys. Med. Rehahif. 62, 619-622.
Weale, R. (1963) Tfre Aging Eye. Lewis, London.
Wolf E. and Gardner J. S. (1965) Studies on the scatter of
light in the dioptric media of the eye as a basis of vpisual
glare. Acta opthal. 74, 338-345.