Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
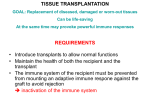
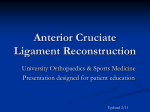
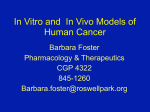
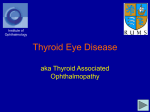
Surface Disorder Ocular Ocular Surface Disorder Mucous Membrane Graft Vishnukant Ghonsikar MS, DNB,FICO,FAICO Vishnukant Ghonsikar MS, DNB, FICO, FAICO, Neelam Pushker MD, M.S. Bajaj MD Dr. Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi I n ophthalmology mucous membrane graft (MMG) has unique application in reconstruction of ocular surface, posterior lamella of lid, contracted socket and as a spacer for lid retraction. Today ophthalmologists are keen to explore these applications of MMG. Detailed knowledge about its various application, graft harvesting, surgical techniques & postoperative care is very essential for providing successful and safe outcome1,2. Grafts in lid reconstruction Free grafts are often needed for large lid defects which cannot be closed by direct suturing or advancement flaps. • • For anterior lamella of the lid, full thickness skin grafts taken from ipsilateral or contralateral upper lid is the best match. If enough upper lid skin is not available as in young patients, full thickness skin grafts can be taken from post auricular region, inner upper arm, supraclavicular region and nasolabial fold. For posterior lamella, tarsoconjunctival free graft is the best option. Other options include buccal mucosa, lip mucosa, nasal or hard palate mucoperichondrium, auricular cartilage. Mucous membrane graft [Lip/ Buccal mucosa]3 A mucous membrane graft can be removed free-hand or with the aid of a mucotome. It is generally easier and safer to remove such a graft free hand. The donor sites are the lower lip (Figure 1), upper lip, and the buccal mucosa. The lower lip is preferred. The access is easier and no sutures are required to close the donor site wound which epithelialises spontaneously over the course of 2 to 3 weeks. The buccal mucosa yields more graft material but normally has to be sutured and is not as accessible. Great care must be taken to avoid damage to the parotid duct, whose opening is opposite the upper second molar tooth, when harvesting a buccal graft. Indications • Ocular surface reconstruction e.g. symblepharon release and reconstruction or excision and replacement of keratinised conjunctiva in Steven Johnson’s Syndrome (SJS). • Lid reconstruction as posterior lamella • Contracted socket • As a spacer for lid retraction • Severe eyelid cicatricial entropion • Conjunctival replacement following an enucleation • With minor salivary gland in dry eye treatment Any patient who is to undergo an enucleation and who has conjunctival scarring from previous surgery or trauma may require a mucous membrane graft. The patient should be counseled about this possibility prior to surgery and the anesthetist should be informed. The anesthetist should place a throat pack after induction of anesthesia and should place the endotracheal tube to one side of the mouth. The donor site is injected with xylocaine and adrenaline before the patient is prepared and draped for surgery. Hard palate graft4 Hard palate mucosa (Figure 2) is more rigid than lip or buccal mucosa as it has perichondrium. It has a rougher surface because of keratinized epithelium unlike lip mucosa. It does not tend to shrink more than 10% postoperatively. www. dosonline.org l 31 Ocular Surface Disorder 1 2 3 Figure 1: The mucous membrane graft is harvested Figure 2: The area of the hard palate from which a graft can be safely harvested (shown with arrows) Figure 3: Position of the nasal septal cartilage to be removed Its use in upper eyelid should be avoided where it may abrade the cornea except in the anophthalmic socket. The anesthetist should place a throat pack after induction of anesthesia. The donor site is injected with 3 to 5 ml of 0.5% Bupivacaine with adrenaline before the patient is prepared and draped for surgery. Indications • Spacer in lower lid retractor recession. • Posterior lamellar graft in lower eyelid reconstruction. • Graft in severe lower eyelid cicatricial entropion surgery. Other Grafts Auricular cartilage graft The auricular cartilage graft has a number of indications but its use is limited by the anatomical size and shape of an individual patient’s pinna. In contrast to the hard palate graft, the auricular cartilage graft has the disadvantage of lacking a mucosal surface. Indications • A tarsal replacement in upper eyelid reconstruction. • A tarsal replacement in upper eyelid entropion surgery. • Graft for the reconstruction of a contracted socket. • Upper eyelid tarso-conjunctival graft Nasal septal cartilage graft A free tarso-conjunctival graft is harvested from the upper eyelid. Caution should be exercised, however, in the use of such a graft as the tarsus provides structural support for the upper eyelid and the adjacent conjunctiva. It is important to evert the upper eyelid preoperatively to ensure that the height of the tarsus is adequate. A minimum of 3.5 mm of tarsus from the eyelid margin should be left undisturbed. A nasal septal cartilage graft (Figure 3) makes an ideal posterior lamellar replacement for lower eyelid reconstruction where the whole of the lower eyelid has been resected. It is usually used in conjunction with a Mustardé cheek rotation flap. Indications A posterior lamellar mucous membrane graft is typically used for patients with a severe entropion with marked symblephara, severe lagophthalmos and eyelid retraction. A graft is indicated if the patient requires a subsequent penetrating keratoplasty. Amniotic membrane may be used as an alternative graft if the patient agrees to the use of donor material. It is preferable to avoid the use of a hard palate • A posterior lamellar graft in eyelid reconstruction • A graft in severe upper or lower eyelid cicatricial entropion surgery • A spacer in lower lid retractor recession 32 l DOS Times - Vol. 19, No. 4 October, 2013 A tarsal replacement in lower eyelid reconstruction. Mucous Membrane Graft Ocular Surface Disorder 4 5 Figure 4: Extensive keratinization of posterior lamella of eyelid following severe Stevens–Johnson syndrome Figure 5: Excision of the keratinized area avoiding damage to eyelashes 6 7 Figure 6: The lip mucosa has been marked and injected with local anaesthetic followed by careful dissection for the removal of a mucous membrane graft Figure 7: Observe for bleeders and if required bipolar cautery is used to cauterize any bleeding vessels graft for use in the upper eyelid as the corneal surface, which is often already compromised, can be damaged by its rougher surface. The procedure is usually performed under appropriate anesthesia as per the patients age and co-operation. Surgical steps For reconstruction of posterior lamella after symbhlepharon release in post SJS / Chemical injury • The lower lip is everted with fingers or atraumatic forceps. The lip mucosa is dried with a swab. The template is transferred to the lower lip mucosa or the required lip mucosa is marked with avoiding the vermillion border and frenulum. This is outlined with a sterile gentian violet. • The marked incision line is gently incised with a no. 15 scalpel blade and the graft removed very carefully using blunt-tipped Westcott scissors and small-toothed forceps (Figure 6). The Westcott scissors should be kept just under the surface of the graft with the edge of the graft drawn horizontally to ensure that the graft is not inadvertently perforated and that the dissection is not taken too deep. Dissection in a deeper plane risks leaving areas of the lip with sensory loss. • The graft donor site is compressed with topical adrenaline on a swab. Bipolar cautery is used to cauterize any bleeding vessels (Figure 7). The graft is carefully shaped with Westcott scissors (Figure 8) and graft is then placed ensuring that the original graft surface faces upward, on the recipient bed and interrupted 7/0 Vicryl sutures are placed from the graft edge to the recipient conjunctival edge (Figure 9). The graft must be maintained in position with the use of a symblepharon ring when the graft is placed onto the • Two to three milliliters of bupivacaine with adrenaline mixed with lidocaine is injected along the upper lid skin crease. • A 4/0 Silk traction suture or a cotton suture is placed horizontally through upper eyelid margin centrally and the eyelid is everted over a Desmarres retractor (Figure 4). • All symblephara are divided with Westcott scissors. • The conjunctiva at the upper border of the tarsus is incised and dissected free from all subconjunctival scar tissue into the superior fornix and onto the bulbar surface of the globe (Figure 5). • Next, a template is taken of the conjunctival defect or the size of the defect is measured. • The lower/upper lip mucosa is injected with local anesthetic. • • www. dosonline.org l 33 Ocular Surface Disorder 8 9 Figure 8: The graft is carefully thinned with Westcott scissors removing any fibro-fatty tissue Figure 9: The graft is then placed ensuring that the original smooth graft surface faces upward References 10 1. Brian Leatherbarrow: Oculoplastic Surgery Second Edition 2011. Informa Healthcare Ltd. 2. Henderson HW, Collin JR. Mucous membrane grafting. Dev Ophthalmol. 2008; 41: 230–42. 3 . Putterman (1980): Basis oculoplastic surgery in Peyman GA: Principles and practice of ophthalmology, Vol. 3. Philadiphia: WB Saunders Company, 2246-2333. Figure 10: The graft must be maintained in position with the use of full thickness anchoring sutures tied over pegs • • globe or a conformer of an appropriate size and shape when the graft is placed centrally in an anophthalmic socket. If the graft is used to reconstruct a conjunctival fornix it should be held in place with a silicone retinal band and 4/0 Nylon fornix-deepening sutures (Figure 10). Topical antibiotic ointment is instilled into the eye. A compressive dressing is applied. Postoperative Care of donor site The patient is instructed to avoid any hot drinks or hot food for a period of 1- 2 weeks. The patient is discharged on a broad spectrum oral antibiotic for a week and an oral antiseptic mouth wash for 2 weeks. Topical preservative free antibiotic drops are instilled into the eye four times a day for 2 weeks. A preservative free topical lubricant is used. The patient is instructed to sleep with the head elevated for 1-2 weeks. The symblepharon ring is maintained in place for a minimum period of 6 to 8 weeks. The patient has to be reviewed twice weekly to ensure that the symblepharon ring does not cause any corneal problems. 34 l DOS Times - Vol. 19, No. 4 October, 2013 4. Bartley GB, Kay PP. Posterior lamellar eyelid reconstruction with a hard palate mucosal graft. Am J Ophthalmol 1989; 107: 609–12.