Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
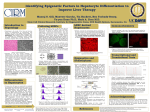
PEROXISOME MOSAICS IN PATIENTS : MODULATION OF GENE EXPRESSION ? Frank Roels, Hanna Mandel, Marisa Giros, François Eyskens, Mercedes Pineda, Jeannette Gootjes*, Marc Espeel, Bwee Tien Poll-The* and Jean-Marie Saudubray Universiteit Gent, Belgium; Rambam Med Ctr, Haifa; Inst Bioquimica Clin, Barcelona; Ctr Metab Dis, Antwerpen; Hosp S Joan de Deu, Barcelona; *AMC, Amsterdam; Enfants-Malades, Paris The liver of mosaic patients displays cells with peroxisomes (Px) adjacent to cells without Px; instead the matrix enzymes catalase and AGT(alanine-glyoxylate aminotransferase) are in the cytoplasm. The latter cells resemble those of Px biogenesis disorders such as the cerebro- Figure 1. Liver parenchyma of mosaic patient : localisation of catalase activity (DAB at pH 10.5); boundary is shown between regions with and without peroxisomes (granules). In hepatocytes without Px, the cytoplasm and some nuclei are stained. Identical images are obtained after immunolocalisation of matrix enzyme AGT. Figure 2. Gold particles give evidence of normal localisation of thiolase inside Px of mosaic patient 3 (antibodies from T. Hashimoto that reveal hTH1, clofibrate-inducible in rats). Postembedding, LRwhite. hepato-renal syndrome of Zellweger (ZS) and infantile Refsum disease (IRD). Peroxisome containing hepatocytes are estimated at 1-10 % of the liver parenchyma in the biopsy- or autopsy sample. Identical to ZS, mosaic livers show PAS positive macrophages with polarizing, trilamellar inclusions and insoluble lipid droplets. Blood and urine metabolites give proof of impaired peroxisomal fatty acid oxidation of straight and branched chains (accumulation of very long chain fatty acids C26, and phytanic acid) and of pipecolic acid – similar to patients without Px. In contrast, mosaic patients have normal or mildly decreased plasmalogen synthesis, explained perhaps by the activity of the residual peroxisomes. Since these disorders are inherited, all cells are expected to have an identical genome; the wide use of cultured fibroblasts in diagnosis and research is based upon this axioma. The discovery of mosaics in the liver is a challenge to geneticists. In normal individuals Px vary during development and in distinct cell types; they are altered when cells are cultured depending on the culture conditions, and under the influence of hormones and substrates. This reflects regulation of gene expression. We have studied 10 of such patients; 5 were reported in detail (1-6). A review is in print (8). Six patients have died : the youngest at the age of 13 months (from bronchopneumonia, after some initial development and improved hepatic function); others died at 8 3/4 y, 13.5 y, 15 y (after menarche), 17.5 y; 24 y. This outcome was preceded by progressive central neurological deterioration in 4/6. Four more are alive and now 7 y, 12 y, 14y and 43 y old. The younger two are developing further : one walks, talks, dresses, reads a few characters; the youngest has acquired syntaxis and vocabulary but not reading because of her visual handicap; both receive supplementation of DHA C22:6. At birth 6 were without symptoms, only 2 showed facial dysmorphia; this is very different from a typical Zellweger. Although their disease history is diverse, the 10 patients have in common a less severe syndrome and longer survival than Zellweger syndrome. Pathology: in the hepatocytes that possess Px, acylCoA oxidase, thiolase and the 43 kDa Px membrane protein (PMP), in addition to catalase and AGT, are correctly localised (fig. 2). Pat3 is peculiar in that catalase is in Px as well as in the cytoplasm of the same cell (3). However in the liver of Pats 9 and 10, the mosaic is formed by incomplete peroxisomes i.e. Px miss one or more enzymes, which are in the cytoplasm or even in lysosomes. In Pat9, catalase and AGT are absent in peroxisome-like organelles but they label for thiolase; oxidase is seen in fewer structures. In Pat10 the pattern is more complex still : rare hepatocytes have large and normal looking catalase positive peroxisomes; more cells show numerous smaller organelles labelling for AGT and thiolase, while the immuno-gold label for oxidase is seen over large granules with heterogeneous contents resembling secondary lysosomes. Indeed, these large granules also label for the lysosomal enzyme cathepsin D and sometimes display trilamellar inclusions that in other patients are within lysosomes (6). Thiolase1 labelling is positive in Px-like organelles but also at the periphery of “empty” vesicles. Immunoblot analysis in fibroblasts of this patient shows normal acylCoA oxidase, and abnormal thiolase. Morphometry in random electron micrographs finds that Px are significantly smaller in 2, and more numerous (Nv) in 2 livers when their number is expressed over the volume of the positive hepatocytes only (2,3,5); this suggests activation of the peroxisomal compartment. In a third liver Px have a raised volume Vv and surface density Sv. The adrenal cortex of Pat4, who died at 15 y, shows atrophy and few but the same equidistant trilamellar inclusions in lysosomes and insoluble lipid, as in Zellweger, X-ALD and D-BP (bifunctional protein) deficiency (7). The brain has paucity of myelin and PAS-positive macrophages with polarizing inclusions that are however much more discrete than in X-ALD. Genetics : 2 patients in our series are brothers, and their parents are consanguinous. Mutation analysis in mosaic patients is hampered by normal or variable parameters of their cultured fibroblasts. Complementation analysis of fibroblasts from 3 patients indicate mutations in Px biogenesis genes PEX2 and PEX6 (2 pts). As reported earlier, a deficiency of both genes can be compensated by overexpression of Pex1protein, resp PMP70. Moreover Pex1p and Pex6p interact with Pex25p. Both PEX2 and 6 have temperature sensitive mutants. Hypothesis: these features might lead to modulation of the genetic defect, depending on the expression level of compensating and interacting proteins, and on temperature (fever...). Since protein concentration normally varies between hepatocytes (albumin...), modulation could result in biogenesis of normal Px in some cells, and not in others. This model implies that both types of hepatocytes have the same genome. This is being investigated by analysis of regions with and without Px separated by laser microdissection. Refs.: Mandel 1994, J Pediatr 125:549; 2) Espeel 1995,Hepatology 22:497;3) Espeel 1995, Eur J Cell Biol 67:319; 4) Giros 1996, Ann NY Acad Sc 804:747; 5) Roels 1996, Ann NY Ac Sc 804:502; 6) Pineda 2000, J Child Neurol 14:434; 7) Depreter 2003, Microsc Res Techn 61:202; 8) Peroxisomal disorders and regulation of genes, Eds Roels, Baes, DeBie, Kluwer Ac/Plenum Publ, 2003, in press.