Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
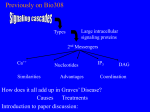
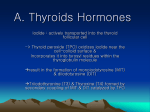
The Family Practice Newsletter The Ohio University College of Osteopathic Medicine The Ohio Northern University Raabe College of Pharmacy Doctors Hospital Family Practice Volume 6, Issue 1 August, 2006 Hashimoto’s Disease or Graves’ Disease? Clinical findings, diagnosis and treatment Kelly Pfaff, Ohio State University College of Pharmacy, Pharm.D. Candidate Graves’ disease is by far the most common form of thyrotoxiCOSIS, or hyperthyroidism, and Hashimoto’s disease, also called chronic lymphocytic thyroiditis, is the most common form of thyroidITIS. Both Graves’ and Hashimotos can present with similar clinical findings which suggests that they may be the same disease manifesting in different ways 1. The pathophysiology of Graves’ disease involves the formation of autoantibodies (IgG) that bind to the TSH receptor in thyroid cell membranes and stimulate the gland to hyperfunction. TSH receptor antibodies are seen in the plasma of approximately 80% of patients with this disease 2. Other antibodies such as antinuclear antibodies (ANA) are also generated in Graves’ disease, with antithyroperoxidase or antithyroglobulin antibodies being increased in most patients as well. Additional laboratory findings include a suppressed TSH level, but increased T4, free T4, and free T4 index. Patients will tend to present with diffuse enlargement of the thyroid or goiter, infiltrative ophthalmopathy, and show signs of gland hyperactivity including sweating, weight loss, anxiety, loose stools, heat intolerance, irritability, fatigue, weakness, or menstrual irregularity 2. Physical exam will show tachycardia, warm, moist skin; stare or tremor 2. In older patients, toxic uninodular and mutinodular goiter account for about 10 to 40% of cases and typically infiltrative ophthalmopathy is absent 3,4. Elderly patients may also present with anorexia and wasting, congestive heart failure, or atrial fibrillation 4. Hashimoto’s thyroiditis is also considered an autoimmune disorder of the thyroid. Its frequency is increased with dietary iodine supplementation and has a strong familial component 2. Also, certain drugs such as amiodarone, interferon-alpha, interleukin-2, and G-CSF frequently induce thyroid antibodies 2. Hashimoto’s thyroiditis is more often found in patients with other autoimmune conditions such as IBS or celiacs disease 2. Patient presentation of Hashimoto’s thyroiditis is mostly related to levels of thyroid hormone and is variable depending on the time of patient diagnosis 1,2. The thyroiditis often progresses to hypothyroidism, which is usually permanent. Depression and chronic fatigue are often reported in addition to dry mouth and dry eyes. Patients with clinically evident disease usually have increased levels of antithyroperoxidase or antithryoglobulin in addition to a diffusely enlarged, firm thyroid gland just as in Graves. Although rare, it has been found that severe Hashimoto’s thyroiditis may cause a transient hyperthyroidism during its initial destructive phase making its presentation similar to Graves’ disease 2. Because of the similar presentation and initial laboratory findings, distinguishing thyroiditis from hyperthyroidism may be difficult, especially if goiter is present, but RAIU (radioactive iodine uptake) can be diagnostic 4. In Hashimoto’s thyroiditis and Graves’ disease, the thyroperoxidase or thyroglobulin antibodies are usually high, but the RAIU is typically low in Hashimoto’s and high in Graves disease 2,4. Also, it is said that in Hashimoto’s, the thyroid gland is firmer and more lobulated than in Graves’ disease 4. Diagnosis of either condition should follow a step by step approach. If hyperthyroidism is suspected, obtain TSH and thyroid function tests, as well as thyroid antibody titers. When hyperthyroidism and exophthalmos are present, the diagnosis is considered Graves’ disease 4. In the absence of exophthalmos, an RAIU is warranted to further define the nature of the disease as above. Treatment of Graves’ disease involves a choice of methods, rather than a method of choice 2. Propranolol is generally used for symptomatic relief until hyperthyroidism is resolved. The recommended dose of propranolol is 10 to 40 mg per dose every 6 hours5. Methimazole or PTU (propylthiouracil) is generally used for young adults or patients with mild thyrotoxicosis, small goiters, or fear of isotopes 2. Older patients also respond well to these agents 2. Methimazole should be given in 3 divided doses approximately 8 hours apart. Initially, 15 mg per day for mild cases, 30 to 40 mg per day for moderate, and up to 60 mg per day for severe hyperthyroidism. Adult dosing of PTU is 300 to 450 mg per day in 3 divided doses (every 8 hours); severe cases may require 600 to 1200 mg per day in 2 to 3 divided doses5. Other options include iodinated contrast agents such as Bilivist or Telepaque, radioactive iodine, or thyroidectomy. Thyroidectomy is indicated for Graves’ disease in the presence of a large symptomatic goiter, failed medical therapy, or the need for rapid reversal of the hyperthyroid state 6. One study also reveals an increased risk for malignancy in patients with concomitant thyroid nodules and Graves’ disease and recommends thyroid surgery 6. In the same study, thyroid removal can stabilize and even reverse both mild and severe forms of ophthalmopathy in most patients6. In Hashimoto’s disease, levothyroxine should be given if hypothyroidism or large goiter is present 2. Dosing of levothyroxine is 1.7 mcg/kg/day in otherwise healthy adults <50 years old. In patients > 50 years old, initial dose should be 25 to 50 mcg per day. In patients < 50 years of age, but with concurrent cardiac disease, initiate levothyroxine dose at 12.5 to 25 mcg per day. Titration of doses should be done at 6 to 8 weeks with appropriate thyroid hormone levels drawn and reviewed. The average starting dose is ~ 100 mcg per day with usual maintenance doses at < 200 mcg per day. If doses exceed 300 mcg, consider poor adherence, malabsorption, or other drug interactions5. Finally, if the thyroid gland is only minimally enlarged and the patient is euthyroid (with normal TSH levels), watchful waiting is in order since hypothyroidism may develop subsequently 2. References: 1 Koda-Kimble MA, Young LY, Kradjan WA, Guglielmo BJ, Alldredge BK. Applied therapeutics: the clinical use of drugs. 7th ed. Maryland; Lippincott; 2000. 2 Tierney LM, McPhee SJ, Papadakis MA, editors. Current medical diagnosis and treatment 2003. 42 nd ed. New York: McGraw-Hill; 2003. 3 Brunton LL, Lazo JS, Parker KL, editors. Goodman and gilman’s: the pharmacological basis of therapeutics. 11 th ed. New York: McGraw-Hill; 2006. 4 Hyperthyroidism. In: O’Hanlon KM, Baustian GH, Toth DW, contributors: First Consult [database on the internet]. St. Louis: Elsevier, Inc.; c2006 [cited 2006 Aug 10]. Available from: http://www.firstconsult.com/fc_home/members/?urn=com.firstconsult/1/101 5 LexiDrugs [palm program database]. Lexi-Comp, Inc. Lexi-Comp reader. Ver. 2.4.060323; 2006; Accessed on August, 21, 2006. 6 Weber KJ, Solorzano CC, Lee JK, Gaffud MJ, Prinz RA. Thyroidectomy remains an effective treatment option for graves’ disease. Am J of Surgery. 2006 (191):400-405.

















![hyperthyroidism[1]](http://s1.studyres.com/store/data/008605222_1-dacb84f161d1e1b3e1ad8241d609e7ce-150x150.png)