Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
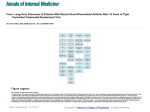
Modern Therapeutics in Rheumatic Diseases Alistair Duncan (Clinical Pharmacist) Lynn Sinclair (Rheumatology Nurse) The Robert Gordon University Non Medical Prescribing Conference 2014 Developments in Therapeutics for.... • Rheumatoid Arthritis • Psoriatic Arthritis • Ankylosing Spondylitis Biologics have revolutionised treatment and outlook for those with inflammatory joint diseases Rheumatoid Arthritis • Emphasis is now on: – Early diagnosis – Early (and aggressive) treatment • Methotrexate is the GOLD STANDARD treatment Goals of Treatment • • • • • Reduce pain and inflammation Preserve function Maintain employment Remission / Cure Reduce cardiovascular risk Symptomatic Control • Analgesia – As per WHO analgesic ladder • NSAIDs – Take into account co-morbidities – COX 1 vs COX 2 selectivity – Cardiovascular and GI side effects • Steroids – i.m. / i.a. / oral Traditional DMARDs Disease Modifying Anti-Rheumatic Drugs • • • • • • • Methotrexate Sulfasalazine Hydroxychloroquine Leflunomide Penicillamine Ciclosporin Gold (injection) • Azathioprine • Cyclophosphamide • Chlorambucil • Prednisolone A: Placebo ! D: Azathioprine G: Penicillamine B: Auranofin E: Methotrexate H: IM Gold C: Antimalarial F: Sulfasalazine Methotrexate • • • • First used in 1947 for childhood leukaemia Probably the most effective DMARD Convenient ONCE weekly dosing ??? Faster onset of action (6 weeks to 3 months) – (compared to other DMARDs) • Mode of action - unclear!! • Remember – Folic acid Side Effects • Nausea, stomatitis • Haematological toxicity • Hepatic toxicity – LFTs, cirrhosis, hepatic fibrosis • Pulmonary toxicity – pneumonitis • Teratogenic (ova and sperm) Patient specific information Responsibility of the Consultant Responsibility of the GP + monitoring schedule What to do if…? Prescribing Information General Responsibilities A Patient’s Story Methotrexate Safety • 2.5mg tablets and 10mg tablets now as different shapes • NHSG policy is to always prescribe 2.5mg tablets • Ensure patient understands dose in terms of mg and number of tablets • Avoid use of “as directed” • Remove prescriptions from repeat piles • Ensure regular monitoring Methotrexate Prescribing Points • • • • • • • Ensure folic acid is prescribed Avoid Trimethoprim (+ Co-trimoxazole) Refer unexplained breathlessness/cough Caution alcohol intake Ensure adequate contraception Avoid live vaccines Follow shared care protocol How to measure Rheumatoid Arthritis? 28 Joint Count DAS (28) Score • Swollen and Tender Joint Count • ESR • Global health assessment by patient DAS28 = 0.56 x sqrt(tender28) + 0.28 x sqrt(swollen28) + 0.70 x ln(ESR) + 0.014 x GH DAS in Practice • “An objective method for measuring disease activity” • >5.1 = Active disease • <3.2 = low disease activity • <2.6 = Remission Health Assessment Questionnaire • Dress yourself including tying shoe laces and doing buttons • Shampoo your hair • Stand up from an armless straight chair • Get in and out of bed • Cut your meat • Lift a full cup or glass to your mouth • Walk outdoors on flat ground Aids or devices that you may use • • • • Cane Crutches Walking frame Built up chair Effect of a treatment strategy of tight control for rheumatoid arthritis (the TICORA study): a singleblind randomised controlled trial Catriona Grigor, MBChB, Hilary Capell, MD, Anne Stirling, RGN, Alex D McMahon, PhD, Peter Lock, MSc, Ramsay Vallance, FRCR, Wilma Kincaid and Duncan Porter, MBChB The Lancet Volume 364, Issue 9430, Pages 263-269 (July 2004) DOI: 10.1016/S0140-6736(04)16676-2 Copyright © 2004 Elsevier Ltd Terms and Conditions TICORA • Tight Control for Rheumatoid Arthritis • Intensive out-patient management of RA vs Routine Care • “Treat to target” • If DAS > 2.4 , = step up in treatment • Joints injected at monthly visits if necessary. Figure 3 Source: The Lancet 2004; 364:263-269 (DOI:10.1016/S0140-6736(04)16676-2) Terms and Conditions Treat to Target Traditional DMARDs Disease Modifying Anti-Rheumatic Drugs • • • • • • • Methotrexate Sulfasalazine Hydroxychloroquine Leflunomide Penicillamine Ciclosporin Gold (injection) • Azathioprine • Cyclophosphamide • Chlorambucil • Prednisolone Biologics** • Target pro-inflammatory cytokines – Tumour necrosis factor (TNF) alpha – Interleukin 6 – Interleukin 1 – Interleukin 12/23 (Ustekinumab for Psoriatic arthritis) • Other immune pathways – B Cells – T Cells **All co-prescribed with MTX where possible Eligibility for Biologics (SMC) • Active disease (DAS > 5.1) – On 2 occasions, 1 month apart • Adequate therapeutic trial of at least 2 DMARDs (inc methotrexate) Treat to Target - Next Steps The nurses role in assessing patients prior to commencing Anti-TNF therapy Medical Requirements • Bloods checked for Hepatitis B + C core Antibodies • Recent chest x-ray • No history of TB or MS • No history of cancer • Patient is not awaiting any surgical/medical/dental procedures • Consultant referral letter • Ensure patient does not require to be TB screened • Varicella • Does patient meet the DAS requirement to commence Biologic (>5.1) • What medication is the patient currently using for arthritis? Patient safe to commence Anti-TNF • When all investigations are completed and the patient is safe to proceed with the nurses assessment they will attend the department to have a repeat disease activity assessment (DAS) • If patient has had recent steroids this may reflect on the actual score • The nurses role is then to assess the patients joints for any tenderness or swelling. • ESR is obtained and recorded. • Health assessment questionnaire filled in by patient and results recorded. • Pain score, early morning stiffness and patients global assessed. • All scores are entered into a DAS calculator Patient meets the criteria to commence treatment. • Education provided on the chosen drug • Injection demonstrated to patient – opportunity to familiarise themselves with the injection device by using demonstration syringes • Patient registered with Homecare company – Injections delivered to patients home – Homecare nurse to supervise patient doing first injection. • Nurse review at 3 months - DAS recorded. • Nurses review again after 3 months, then 6 monthly thereafter. Patient X Etanercept • Patient currently has rheumatoid arthritis and medical staff would like him assessed for possibility of commencing anti tnf therapy • DAS prior to any treatment 7.64 • DAS 3 months after commencing treatment 4.02 • DAS 6 months after commencing treatment 2.16 Anti –TNF alpha • • • • • Certolizumab – fortnightly s/c inj. Etanercept – weekly s/c inj. Adalimumab – fornightly s/c inj. Infliximab – 8 weekly iv infusion Golimumab – monthly s/c inj. • Typically (£9 - 10k per patient per year) • S/C treatments via Homecare Company TNFα and it’s Receptor Recombinant TNFα Soluble Receptor Monoclonal antibody against TNFα Adverse Effects of TNF Inhibitors • Serious Infections – TB – Skin and soft tissue – Blood borne viruses • Malignancy – ? Lymphoma – ? Solid Tumors – Conflicting data • Injection site reactions • Infusion reactions • Increased risk of cardiac failure • Demeyelination When to with-hold biologics? • Should be discontinued in the presence of serious infections, but can be recommenced once the infection has resolved clinically. • Stop biologic 3 to 5 half lives before major surgery. Should not be restarted after surgery until there is good wound healing and no evidence of infection. B Cell Depletion • Rituximab – 2 x fixed 1g doses 14 days apart – IV infusion – Dose repeated, but not at a fixed interval Interleukin 6 Inhibitor • Tocilizumab • 4 weekly iv infusion • Now available as weekly s/c injection T Cell Co-Stimulation Modulator • Abatcept – 4 weekly iv infusion – Now available as weekly s/c injection Remember • Always consider that a patient with RA / AS / PSa may be on a drug supplied via homecare • Ensure recommended monitoring is carried out. • Caution in patients going for major surgery, or with concurrent infection. Info Resources • British Society for Rheumatology (BSR) • http://www.rheumatology.org.uk • European League against Rheumatism (EULAR) • http://www.eular.org/ • Arthritis Research • http://www.arthritisresearchuk.org/ • SIGN 123: Management of Early RA • http://www.sign.ac.uk