Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
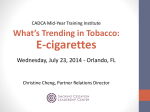
Winning the Tobacco Battle: One Smoker at a Time Carol Southard, RN, MSN Tobacco Treatment Specialist [email protected] 312 926 2069 Disclosure Information: The presenter, Carol Southard, RN, MSN, has received honoraria as a guest speaker for the following company: •Pfizer Presentation Objectives At the conclusion of this program, the participant will be able to: • Describe trends and issues regarding tobacco cessation • Discuss tobacco cessation intervention • Review treatment options in the management of tobacco cessation • Explain current guidelines on tobacco cessation intervention • Summarize appropriate tobacco cessation pharmacotherapy • Incorporate tobacco cessation treatment into clinical practice Historica Vital et Mortis 1622 “The use of tobacco… conquers men with a certain secret pleasure so that those who have once been accustomed thereto can hardly be restrained therefrom” Sir Francis Bacon “There is little doubt in my mind that if it were not for nicotine, in tobacco smoke, people would be little more inclined to smoke than they are to blow bubbles or light sparklers” Philip Morris Researcher 1976 Some Harmful Chemicals in Tobacco Smoke Acetaldehyde Acetone Acetonitrile Acetylene Acrolein Acrylonitrile Ammonia Aniline Arsenic Benzene Benzopyrene 2,3 Butadione Butylamine Carbon Monoxide Cyanide Dimethylamine Dimethylnitrosamine Ethylamine Formaldehyde Hydrocyanic Acid Hydrogen Cyanide Hydrogen Sulfide Methacrolein Methanol Methyl Alcohol Methylamine Methylfuran Methylnapthalene Nicotine Nitric Oxide Nitrogen Dioxide Phenol Pyridine Tar Toluene Unique Qualities of Nicotine Addiction Through Smoking • Cigarette is a highly engineered drug-delivery system • Inhaling produces a rapid distribution of nicotine to the brain • Drug levels peak within 10 seconds in the brain • Acute effects dissipate within minutes, causing the smoker to continue frequent dosing throughout the day • Average smoker takes 200-300 boluses to the brain per day • Easy to get, easy to use, and it is legal! Tobacco Facts • #1 public health problem in the United States • Most preventable cause of morbidity and mortality • Causes more deaths each year than alcohol, motor vehicle accidents, suicide, AIDS, homicide, illicit drugs and fires combined • One-third of all tobacco users will die prematurely • If current trends hold, tobacco will kill a billion people this century, 10 times more than the 20th century Smoking Incidence & Scope The annual toll on the nation’s health and economy is staggering: 430,000 deaths, 8.6 million people suffering from at least one serious illness related to smoking • More than $289 billion a year, including at least $133 billion in direct medical care for adults and more than $156 billion in lost productivity • $5.6 billion a year (2006 data) in lost productivity from exposure to secondhand smoke • Each day, more than 3,200 persons younger than 18 years of age smoke their first cigarette. • Each day, an estimated 2,100 youth and young adults who have been occasional smokers become daily cigarette smokers CDC (2/14). U.S. Smoking Statistics • About 42.1 million Americans are current smokers – 18.1% • 20.5% of men and 15.8% of women smoke in US (since 1974, the smoking prevalence in men has decreased by about 1% a year, in women 0.33%) • Prevalence – Native Americans & Alaskan Natives (21.8%), – Caucasians (19.7%) – African Americans (18.1%) – Hispanics (12.5%) – Asians (10.7%) CDC (2/14). Tobacco is Not an Equal Opportunity Killer • Affects young, the poor, depressed, uninsured, less educated, blue-collar, and minorities most in the US • Addiction affects those with the least information about health risks, with the fewest resources to resist advertising, and the least access to cessation services • Those below poverty line are >30% more likely to smoke than those above poverty line Smoking-Related Disease Smoking Prevalence • • • • • • Smoking-related chronic disease - 36.9% Smoking-related cancers (other than lung) - 38.8% Stroke - 30.1% CHD - 29.3% Emphysema - 49.1% Chronic bronchitis - 41.1% Cessation Facts • 70% of smokers say they are “interested” in quitting • Only 32% consult a health care provider about quitting • The majority of smokers try to quit on their own • Overall, self-quitters have a success rate of 4 to 6% OF 3 BILLION OFFICE VISITS 2005-2009*: • 62.7% of patients were screened for tobacco use • 17.6% were current tobacco users • 20.9% received cessation counseling • 7.6% received cessation medication *MMWR/June 15, 2012/Vol. 61 Treatment Facts • The efficacy of several tobacco cessation therapies is well established • All proven treatments appear to be equally effective: quit rates are at least doubled • Evidence suggests that all smokers should be offered pharmacotherapy and assisting with treatment produces better outcomes • The Agency for Health Care Policy and Research (AHCPR) published updated smoking cessation guidelines in 2008 for primary care clinicians US PHS Clinical Practice Guideline Fiore M, Jaen CR, Baker TB, et al. Treating tobacco use and dependence 2008 update. Rockville MD: USDHHS, PHS, 2008. http://www.surgeongeneral.gov/tobacco/ Based on approximately 8,700 articles published between 1975 and 2007 Five A’s 1. Ask - initial step is to identify if client uses tobacco 2. Advise - deliver clear, strong, personal, and straightforward advice about the importance of quitting; emphasize five R's: relevance, risks, rewards, roadblocks, repetition 3. Assess - willingness to make a quit attempt 4. Assist - set quit date, offer pharmacologic and behavioral support 5. Arrange - follow-up to prevent relapse Ask. Advise. Refer. = 5 A’s Ask Ask. Advise Every patient about tobacco use. Assess Assist Advise. Every tobacco user to quit. Arrange Refer. Provide information on treatment programs. Refer for Treatment Ask. Advise. Refer. Systematic Approach Does patient now use tobacco? If YES: Is patient willing to quit? If YES: Provide appropriate referral. If NO: Promote motivation to quit. If NO: Did patient once use tobacco? If YES: Prevent Relapse If NO: No intervention required. Encourage continued abstinence. The “5 R’s” to Enhance Motivation for Patients Unwilling To Quit* • • • • • Relevance – Tailor advice and discussion to each patient – encourage patient to identify why quitting is personally relevant Risks – Discuss risks of continued smoking – ask patient to identify potential negative consequences Rewards – Discuss benefits of quitting – ask patient to identify potential benefits Roadblocks – Identify barriers to quitting (targets for counseling and medication) Repetition – Reinforce the motivational message at every visit *Most effective when combined with MI approach and strategies Assessing Nicotine Dependence 1. 2. 3. How soon after you wake do you smoke your first cigarette or take you first dip? • <30 minutes 2 • 31 - 60 minutes 1 • >60 minutes 0 How many cigarettes per day or tins per week do you use? • <10 cigarettes or <1 tin 0 • 11 - 20 cigarettes or 1 - 2 tins 1 • 21-30 cigarettes or >2-3 tins 2 • >30 cigarettes or > 3 tins 3 Do you find it difficult to refrain from using tobacco in places where it is forbidden (e.g., movies, work, etc.)? Yes 1 No 0 Scoring: 0 - 2 (LOW) 3 - 4 (MEDIUM) 5 - 6 (HIGH) Nicotine Withdrawal Symptoms • Constant craving of cigarettes • Insomnia • Irritability • Fatigue • Frustration • Anger • • • • • • Depression Difficulty concentrating Restlessness Decreased heart rate Increased appetite Anxiety Withdrawal lasts anywhere from 3 to 6 months Pharmacotherapy • Seven first-line FDA approved therapies reliably increase long-term smoking abstinence rates • All apt least double the rate of cessation when compared to placebo • All help with symptoms of withdrawal Medications • Nicotine Replacement (gum, patch, inhaler, spray, lozenge) • Bupropion (Zyban ®, Wellbutrin ®) • Varenicline (Chantix®) Nicotine Gum • Available since 1984 • OTC 1995 • 2 mg recommended for patients smoking less than 1 pack per day • 4 mg for patients smoking over 1 pack/day • Full dose absorbed in about 20 minutes • Cost $6.00+ per day Nicotine Patch • Available since 1994 • OTC 1996 • 21 mg recommended for patients smoking 1 pack per day • 14 mg for patients smoking 1/2 pack/day • 7 mg for patients smoking 5 or less cigarettes a day • Full dose absorbed in about 2 hours • Cost $4.00+ per day Nicotine Inhaler® • Available since 1998 - Rx • Each cartridge delivers 4 mg of nicotine over 80 inhalations • Full dose absorbed in about 20 minutes • Cost $10.00+ per day • Designed to combine pharmacological and behavioral substitution Nicotine Nasal Spray Nicotrol NS® • Available since 1996 – Rx • Each spray delivers 0.5 mg of nicotine • Full dose absorbed in less than 5 minutes • Minimum recommended treatment is 8 doses per day • Cost $5.00+ per day • May be most beneficial to highly dependent smokers Nicotine Lozenge • Available since 2002 - OTC • 2 mg recommended for patients who smoke more than 30 minutes after waking • 4 mg for patients who smoke within 30 minutes of waking • Full dose absorbed in about 20 minutes • Cost $5.00+ per day Combination Nicotine Replacement Therapy Combining the nicotine patch and a self-administered NRT (either nicotine gum or nicotine nasal spray) is more efficacious than a single form of NRT Nicotine Delivery Systems: Plasma Concentrations Plasma nicotine (ng/mL) 30 Cigarette 25 20 Gum (4 mg) 15 10 Gum (2 mg) Inhaler 5 Nasal spray Patch 0 0 10 20 30 Minutes 40 50 60 Reprinted with permission from Schneider et al., Clinical Pharmacokinetics 2001;40(9):661–684. Adis International, Inc. Non-Nicotine Medications Bupropion® • An atypical antidepressant with dopaminergic and noradrenergic activity • First FDA approved non-NRT • Risk of seizure is 0.1% or less • Can be used in combination with NRT • Is effective in those with no current or past depressive symptoms Bupropion SR® • • • Available by prescription only (USA) Dosing: – Start 1-2 weeks before quit date – 150 mg orally once daily x 3 day – 150 mg orally twice daily x 7-12 weeks – No taper necessary at end of treatment Maintenance: consider as a maintenance therapy for up to 6 months postcessation Side effects • Dry mouth and insomnia • Risk of seizure: approximately 1 in 1,000 – Contraindicated for patients with seizure disorder or predisposing factors that increase seizure risk (head injury, active substance abuse) Non-Nicotine Medications Varenicline® • A partial nicotinic acetylcholine receptor agonist • Specifically indicated for use as an aid in smoking cessation • Provides some nicotine effects to ease withdrawal symptoms • Blocks effects of nicotine Varenicline® (Chantix) Recommended dosage: • Start 1 week before quit date • 0.5 mg for 3 days • Then 0.5 mg BID for 4 days • Then 1 mg BID for up to 12 weeks Efficacy: • Six clinical trials N=3659 • Self-report verified by CO measurement • 1 in 5 quit at 1 year Side effects: • Nausea and vivid dreams • Pregnancy Category C NO Contraindications though does have Black Box status Extended Use of Pharmacotherapy • • • • • First-line tobacco dependence medications may be considered for extended use, especially in patients with persistent withdrawal symptoms Evidence shows that a minority of patients continue ad libitum NRT agents Does not present known health risks FDA has approved bupropion SR for a long-term maintenance indication FDA has recommended varenicline for a minimal 3month term indication; 6-month term optimal Electronic Cigarettes • No conclusive scientific evidence that e-cigarettes promote successful longterm quitting • Some evidence that current smokers are using e-cigarettes as a way to ingest nicotine in places where smoking is restricted which may delay or even prevent quit attempts • American tobacco companies are now manufacturing electronic cigarettes “….no evidence is available to support the claim that e-cigarettes will help smokers to quit or reduce their harm without unintentional societal effects through large increases in nicotine addiction” The Lancet Oncology, Volume 15, Issue 3, Page e104, March 2014 Practical Counseling • Set quit date within two weeks - starting on the quit date, total abstinence is essential • Tell others (family, friends, co-workers) and request understanding and support • Anticipate challenges - identify what helped and what hurt in previous quit attempts • Remove tobacco products and paraphernalia from the environment (e.g., home) • Provide basic information (e.g., withdrawal) • Help recognize triggers for smoking or relapse (events, activities, emotional states) – discuss challenges/triggers and how patient will successfully overcome them Coding for Treatment of Tobacco Use and Dependence Insurers: ICD-9 Code 305.1 - Tobacco Dependence CPT Code 99406 - Intermediate (3-10 minutes) CPT Code 99407 - Intensive (more than 10 minutes) Medicare: G0436 – Intermediate G0437 - Intensive Affordable Health Care Act • Tobacco use screening for all adults and cessation interventions for tobacco users must be covered without the patient having to pay a copayment or co-insurance or meet a deductible • Applies to new health insurance plans or insurance policies beginning on or after September 23, 2010 • Only applicable when these services are delivered by a network provider Group Program Agenda Session 1 Session 2 Session 3 Session 4 • • • • • • • • • Orientation & Introductions Understanding addiction Preparation_________________ Benefits of Quitting Withdrawal Symptoms Cessation Strategies__________ QUIT DAY_________________ Motivation Reinforcement Support Systems Group Program Agenda (continued) Session 5 Session 6 Session 7 Session 8 • • • • • • • Lifestyle issues: Nutrition/Weight Exercise__________________ Stress Management Relaxation Skills New Self-image____________ Ex-smokers panel_____________ • Graduation & Celebration • Relapse Prevention Online Smoking Cessation Assistance • On-line smoking cessation services now available for smokers who prefer using computers over telephones • Anonymity is a plus, as with telephone quitlines • Early studies show promising efficacy www.smokefree.gov www.becomeanex.org www.quitnet.com www.quityes.com http://www.lungusa.org/stop-smoking/ www.lungchicago.org/quit-smoking http://www.cancer.org/ www.everydayhealth.com/smoking-cessation Power of Intervention • The costs of providing brief interventions is $3 per smoker • Implementing such interventions could quadruple the national annual cessation rate, translating to roughly 4.8 million quitters • Adding brief behavioral counseling and medication can increase the cessation rate six fold, translating to roughly 7.2 million quitters • “If every physician advised every patient at every visit not to smoke, one million Americans could escape nicotine addiction each year.” –Michael Fiore, MD • “Lives saved from smoking cessation would swamp all the benefits accrued if each year every person underwent every cancer screening procedure recommended by the American Cancer Society.”– Steven A. Schroeder, MD Health professionals shouldn’t grade themselves on how many people they can “get” to quit, but rather how many times they give the message when the opportunity arises. Under these criteria, there is no reason not to have an intervention success approaching 100% Dr. Gro Harlem Bruntland, Director General, World Health Organization: “If we do not act decisively, a hundred years from now our grandchildren and their children will look back and seriously question how people claiming to be committed to public health and social justice allowed the tobacco epidemic to unfold unchecked.” US Department of Health and Human Services. Women and Smoking: A Report of the Surgeon General. Washington, DC: Public Health Service, 2001. What about Joe Camel? What about Joe Camel? Role of the Health Care Professional Tobacco-cessation counseling by clinicians is effective in improving tobacco quit rates among adults has been recommended for adolescents. • 3% quit/year if you do nothing • 6% quit for 6 months with 3 minute counseling or practice system USPHSR, 2008 Case Presentation: Mr. E.M. • 66 years old; PMHx CAD with stent 2006; carotid artery disease with stent 1999; CVA 1998; type 2 DM; colon cancer with resection 2011 • Retired teamster • Lives with wife and 2 dogs; wife has MS • Rarely drinks ETOH; smokes 1.5 ppd since teenage years • Patient takes usual secondary prevention medications (ASA, statin, clopidogrel, ACEI, beta blocker, omega-3) • LDL is at goal; was at goal before need for coronary stent • Type 2 DM is well-controlled (metformin) • Height: 5’10”; weight 208 lbs; BMI 29.8 Case Continued • Reports eating “only organic” foods • Physical activity: walks dogs twice a day; swims in backyard pool during the summer • Expresses that he is NOT interested in quitting smoking – Providers have related his progressive CVD to smoking – When addressing the effects of secondhand smoke on his wife, he responded, “Then she shouldn’t have married me!” • Of his risk factors, smoking, BP control, and weight are most urgent (LDL and A1C are at goal) • E.M. is typically willing to make diet and physical activity changes • How do you engage this patient with significant CVD and multiple risk factors to consider quitting smoking? Summary • • Brief tobacco dependence treatment is effective and every patient who uses tobacco should be identified, urged to quit, and offered at least one of these treatments: Patients willing to quit should be provided treatments identified as effective Patients unwilling to quit should be provided an intervention to increase their motivation to quit Intensive interventions should be provided whenever possible • Systems level interventions including reimbursement for effective treatments are essential • It is inconsistent to provide health care and —at the same time— remain silent (or inactive) about a major health risk! References • CDC, “Annual Smoking-Attributable Mortality, Years of Potential life Lose, and Economic Costs – United States 1995-1999,” MMWR, April 11, 2012. • Fiore MC, Bailey WC, Cohen SJ, et al. Treating tobacco use and dependence. Rockville, MD.: Department of Health and Human Services, Public Health Service, 2008. • US Department of Health and Human Services. The Surgeon General’s Report on Women and Smoking. US Department of Health and Human Services, Public Health Service, 2001. • US Department of Health and Human Services. The Surgeon General’s Report on The Health Consequences of Smoking. US Department of Health and Human Services, Public Health Service, 2004. Questions/Comments? True or False The majority of tobacco users are interested in quitting smoking. True 70% of smokers would quit if they knew how and site a provider's advice to quit as an important motivator! True or False Nicotine is capable of creating tolerance, physical dependence and withdrawal syndrome in habitual users. True Nicotine acts on nicotinic acetylcholine receptors in both the central nervous system and the peripheral nervous system resulting in a physical and biologic basis for physical dependence. True or False Nicotine addiction is the most powerful of all addictions to overcome. True It is harder to break the addiction of nicotine than the addiction of alcohol, heroin or cocaine. True or False Cessation pharmacotherapy should be used with all patients attempting to quit using a tobacco product. True There are no longer any true contraindications. Pharmacotherapy approximately double the rate of cessation when compared to placebo. True or False As with other types of drug dependencies, psychosocial or self-help therapies are essential medication alone is ineffective. False Currently, this is not the case with nicotine dependence though adding psychosocial therapy certainly increases quit rates. Insistence on adjunctive therapy as a condition for receiving pharmacotherapy is not based on medical evidence.