Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
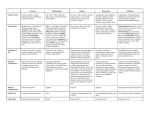
Normal EEG Patterns Dr Lim Shih Hui Senior Consultant Neurologist Singapore General Hospital EEG Interpretation Normal Lack of Abnormality Abnormal Non-epileptiform Patterns Epileptiform Patterns Alpha Rhythm The starting point of analysing awake EEG 8-13 Hz activity occurring during wakefulness 20-60 mV, max over posterior head regions Present when eyes closed; blocked by eye opening or alerting the patient 8 Hz is reached by 3 years of age and progressively increases in a stepwise fashion until 9-12 Hz is reached by adolescence Very stable in an individual, rarely varying by more than 0.5 Hz. With drowsiness, alpha activity may decrease by 1-2 Hz A difference of greater than 1 Hz between the two hemispheres is significant. 10% of adult have little or no alpha Normal Alpha Rhythm Normal Alpha Rhythm Alpha Rhythm: Reactivity Should attenuate bilaterally with eye opening alerting stimuli mental concentration Some alpha may return when eyes remain open for more than a few seconds. Failure of the alpha rhythm to attenuate on one side with either eye opening or mental alerting indicates an abnormality on the side that fails to attenuate Normal Alpha Reactivity Eyes Closed Normal Alpha Reactivity Beta Activity Frequency of over 13 Hz; if >30-35 Hz gamma activity or exceedingly fast activity by Gibbs. Average voltage is 10-20 microvolts Two main types in adults: Often enhanced during drowsiness or when present over a skull defect Should not be misinterpreted as a focus of abnormal fast activity. Beta Activity Frequency of over 13 Hz; if >30-35 Hz gamma activity or exceedingly fast activity by Gibbs. Average voltage is 10-20 microvolts Two main types in adults: The precentral type: predominantly over the anterior and central regions; related to the functions of the sensorimotor cortex and reacts to movement or touch. The generalized beta activity: induced or enhanced by drugs; may attain amplitude over 25 microvolts. Often enhanced during drowsiness or when present over a skull defect Should not be misinterpreted as a focus of abnormal fast activity. Generalized Beta Activity Beta Activity Frequency of over 13 Hz; if >30-35 Hz gamma activity or exceedingly fast activity by Gibbs. Average voltage is 10-20 microvolts Two main types in adults: Often enhanced during drowsiness or when present over a skull defect Should not be misinterpreted as a focus of abnormal fast activity. Theta Activity The term theta was coined by Gray Walter in 1944 when it was believed that this rhythm was related to the function of the thalamus. Occurs as a normal rhythm during drowsiness In young children between age 4 months 8 years: predominance over the fronto-central regions during drowsiness In adolescents: sinusoidal theta activity can occur over the anterior head regions during drowsiness. In adults, theta components can occur diffusely or over the posterior head regions during drowsiness. Single transient theta waveforms or mixed alpha-theta waves can be present over the temporal regions in older adults. Theta Activity The term theta was coined by Gray Walter in 1944 when it was believed that this rhythm was related to the function of the thalamus. Occurs as a normal rhythm during drowsiness In young children between age 4 months 8 years: predominance over the fronto-central regions during drowsiness In adolescents: sinusoidal theta activity can occur over the anterior head regions during drowsiness. In adults, theta components can occur diffusely or over the posterior head regions during drowsiness. Single transient theta waveforms or mixed alpha-theta waves can be present over the temporal regions in older adults. Theta Activity The term theta was coined by Gray Walter in 1944 when it was believed that this rhythm was related to the function of the thalamus. Occurs as a normal rhythm during drowsiness In young children between age 4 months 8 years: predominance over the fronto-central regions during drowsiness In adolescents: sinusoidal theta activity can occur over the anterior head regions during drowsiness. In adults: theta components can occur diffusely or over the posterior head regions during drowsiness. Single transient theta waveforms or mixed alphatheta waves can be present over the temporal regions in older adults. Temporal Slowing Of The Elderly Occur chiefly over the age of 60 years Confined to the temporal regions and are usually maximal anteriorly Occur more frequently on the left side Do not disrupt background activity Usually have a rounded morphologic appearance Voltage is usually less than 60-70 microvolts Attenuated by mental alerting and eye opening and increased by drowsiness and hyperventilation Occur sporadically as single or double waves but not in longer rhythmic trains Present for only a small portion of the tracing (up to 1%) of the recording time when the patient is in a fully alert state EEG of Drowsiness (Stage I Sleep) In adults, most sensitive signs of drowsiness is the disappearance of eye blinks and the onset of slow eye movements Slowing, dropout or attenuation of the background Occurrence of theta activity over the posterior regions Drowsy Drowsy Drowsy EEG of Drowsiness Alpha Activity Mu activity may be occurrence or persistence over the temporal regions after a disappearance of the occipital alpha may be asymmetric may persist Beta activity over the fronto-central regions may become more prominent during drowsiness 20-30 Hz; occasional bursts of 30-40 Hz activity Other Activities During Stage I Sleep Vertex Sharp Transients Positive Occipital Sharp Transients of Sleep (POSTs) Vertex Sharp Transient V-Wave In young adults, the V-waves may have sharp or spiky appearance and attain rather high voltages During the earlier stages of sleep these may occur in an asymmetric fashion Should be careful not to mistake V-waves for abnormal epileptiform activity Sometimes trains or short repetitive series, clusters, or bursts of V-waves may occur in quick succession In older adults the V-waves may have a more blunted appearance Vertex Sharp Transients Post Occipital Sharp Transients of Sleep (POSTs) Sharp-contoured, mornophasic, surface-positive transients Occurring singly or in trains of 4-5 Hz over the occipital head regions May have a similar appearance to the lambda waves during the awake record but are of higher voltage and longer duration Usually bilaterally synchronous but may be asymmetric over the two sides Predominantly seen during drowsiness and light sleep POSTs Stage II Sleep Sleep Spindles K Complex Sleep Spindles In adults, a frequency of 13-14 Hz occur in a symmetric and synchronous fashion over the two hemispheres Usually these occur at intervals between 5-15 seconds, Spindle trains ranging from 0.5-1.5 seconds in duration More prolonged trains or continuous spindle activity may be seen in some patients on medication, particularly benzodiazepams Sleep Spindles Sleep Spindles Sleep Spindles K-Complex A broad diphasic or polyphasic waveform (>500 msec) Frequently associated with spindle activity K-complexes can occur in response to afferent stimulation and may be linked to an arousal response K-Complex Hyperventilation Often produces little change in the EEG in adult If there is a change, usually consists of generalized slowing. either gradual or abrupt onset in theta or delta range may continue as series of rhythmic slow waves or consist of repeated bursts of slow waves at irregular intervals Degree of response depends on the age, the vigor of hyperventilation, blood sugar levels, and posture Intermittent Slow During HV Intermittent Rhythmic Slow During HV Persistence slowing following cessation of hyperventilation: Check if patient is still continuing to hyperventilate or if patient is hypoglycemic Hyperventilation The findings accepted as unequivocal evidence of abnormality: epileptiform discharges clear-cut focal or lateralized slowing or asymmetry of activity Contraindications: significant cardiac or cerebrovascular disease, or respiratory dysfunction. Photic Stimulation Flash rate eliciting maximum driving response increases in rough parallel with age (Niedermeyer, 1982) Driving response may normally have a notched appearance resembling a spike-wave discharge. It can be distinguished from spike-waves by its time-locked appearance with the flash rate and its failure to persist after the stimulation stops. Asymmetries of photic driving probably have less clinical value and can only be interpreted in association with other significant asymmetries Photoparoxysmal Response Photic stimulation may elicit posterior dominant or generalized epileptiform discharges in patients suspected of having photosensitive seizure disorders Photo-paroxysmal response: complex waveform repeat at a frequency which is independent of the flash rate field extends beyond the usual posteriorly-situated photic driving region and may be frontally dominant Time-locked with stimulus or not time-locked / selfsustained Photoparoxysmal Response Photomyoclonic Response Physiologic Activities That Can Be Confused With Epileptiform Activities Vertex transients of light sleep Hypnagogic hypersynchrony Positive occipital sharp transients of sleep (POST) Mu rhythm Lambda waves Breach rhythms Benign Variants Of Unknown Clinical Significance Benign epileptiform transients of sleep (small sharp spikes) 6- and 14-Hz positive spikes Wicket spikes Psychomotor variants (rhythmic mid-temporal theta discharge of drowsiness) Subclinical rhythmic EEG discharge of adults Phantom spike and wave