Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
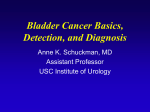
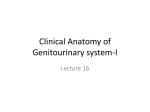
Your bladder cancer diary WA Cancer and Palliative Care Network Patient information and persons to contact Your Name Date of Birth URMN (Patient Hospital Unit Number) Address Phone Mobile GP Name Phone Address Urologist Name Phone Cancer Nurse Phone Hospital Phone Treatment Unit Phone If you are having problems with your treatment: In an emergency contact your nearest emergency department or healthdirect Australia on 1800 022 222. If you are experiencing any urinary symptoms (e.g. blood in urine) please contact the number shown here for further advice: If you have not received any contact informing you of a procedure or appointment contact the number shown here for further information: 1 Introduction This booklet has been designed by a dedicated team of health professionals to provide you with information about your disease, treatment and why it is important for you to have regular check ups as instructed by your doctor. The booklet also enables you and those involved in your care to keep track of both treatments and your ongoing surveillance of your bladder cancer. How To Use This Booklet The booklet contains pages where you and your health professional can fill in your appointments, treatments, and results. It also contains a section for you to document any issues you may wish to discuss when you attend the hospital for appointments. We encourage you to share the information in your booklet with your GP in order for them to be aware of treatment plans of your bladder cancer. You should ensure that the information in this booklet is kept up to date. Ask your doctor, nurse and other carers to help fill it out. Keep this booklet safe and bring it with you with every appointment relating to the management of your bladder cancer. 2 The bladder The bladder is like a balloon. It is a muscular organ that collects and stores urine which has passed down tubes called ureters from the kidneys. It is located in the lower part of the abdomen (the pelvis). Urine is expelled from the bladder through the tube called the urethra when you void. The bladder wall contains different layers made of different types of cells. The inside layer of the bladder is made up of special cells that prevent the waste products in urine being absorbed back into the blood stream. These cells are called transitional cells. Figure 1. Bladder cancer The entire body is made of cells which normally grow and reproduce in an organised manner. Sometimes this process goes wrong. When cells grow and multiply in an uncontrolled way this produces a lump called a tumour. 3 Tumours are classified as being benign (not cancer) or malignant (cancer). When cancer cells first develop they may be contained to the original site, in this case, the bladder. However, these cells have the ability to multiply and spread to other parts of the body if left untreated. Staging and grading of bladder cancer Treatment for bladder cancer depends on three things: 1. type of cancer cells 2. stage of the disease 3. grade of cancer cells. Type of cancer cells: The most commonly occurring cancers in the bladder are transitional cell cancers. This form of cancer originates from the cells which line the bladder and urinary tract. The other 2 types, Squamous cell carcinoma and adenocarcinoma, can occur but are rare. Carcinoma in situ (CIS) is a form of transitional cell cancer that is flat-shaped and usually confined within the inner most layers of the bladder. However this is a high grade cancer. 4 Fat Muscle Connective Tissue Bladder Lining CIS Ta T1 T2 T3 T4 Figure 2. Stage of the disease: The stage tells you how far the cancer cells have grown into the bladder. Figure 2 shows the different stages of bladder cancer. If a bladder cancer affects only the inner lining of the bladder, it is known as a non muscle invasive (or sometimes called superficial) bladder cancer. CIS, Stage Ta and T1 are tumours that are confined to the surface layers of the bladder lining and are classed as non muscle invasive cancer. If the cancer has spread into the muscle wall of the bladder, it is called a muscle invasive cancer. Stages T2 - 4 are types of cancer that invade the bladder muscle wall and require different treatment to non muscle invasive disease. Grading: Tumours are given a grade based on how the cancer appears under a microscope. The grade refers to the aggressiveness of the tumour as this relates to the speed of growth. There are 3 grades: 1.Low (Grade 1) is when cancer cells look more like normal bladder cells which suggest they will not be very aggressive 2. Intermediate (Grade 2) 3.High (Grade 3) is when cancer cells look very abnormal and grow in a disorderly way. These cells tend to grow very quickly. Both grade and stage are factors your doctor will consider when planning your treatment. 5 Treatment for non muscle invasive disease Your doctor may discuss more than one treatment depending on your type of cancer. The most common treatment for non muscle invasive bladder cancer is the removal using surgical instruments inserted through the urethra. This procedure is known as Transurethral Resection of a Bladder Tumour (TURBT). The removed tumour will be sent for inspection by a pathologist to diagnose the type of cancer cells and to establish the extent of the cancer. Your doctor and nurse will be able to explain more about this procedure to you on request. Sometimes patients are given medication directly into the bladder to treat any small non visible areas affected by the cancer and help reduce the chances of the cancer recurring. This treatment is called intravesical therapy. Following your TURBT you may receive an instillation of medication into the bladder called Mitomycin C. This is a purple coloured chemotherapy agent that affects the lining of your bladder to kill any remaining microscopic cancer cells and reduce the likelihood of the cancer returning. It is put directly into the bladder through your catheter. It does not have the usual side effects with chemotherapy such as hair loss and sickness as the treatment is directly to the bladder. For some patients, this is all the treatment needed at this stage. Other patients require further treatment. Your doctor will inform you if you need any more treatment at this point in order to help prevent the return of the cancer. You can use this book for recording any further treatments you are having. 6 For patients with non muscle invasive disease treatments include: Further Mitomycin C treatment given on a weekly basis for 6 weeks. This procedure involves having a catheter inserted and the medication inserted through the catheter into the bladder where it is held for 1 to 2 hours before you pass urine into the toilet. BCG (which is primarily used for the vaccine of Tuberculosis). This medication has been found to help the bladder’s immune system to fight the disease and kill the cancer cells left in the bladder. The BCG is put into the bladder in the same way as the Mitomycin C and held in for 1 to 2 hours before you pass urine into the toilet. The BCG is usually given weekly over a six week period initially. Some patients require further BCG given at three monthly intervals. In some cases, you may also be given a combination of BCG and Mitomycin C where the medications may be alternated at different appointments. Follow up & Surveillance It is important to have regular check ups in order for your doctor to observe inside your bladder for the effects of these treatments and to look for any possible signs of cancer recurrence. This is done using a procedure called a flexible cystoscopy. The frequency of the cystoscopy will be determined by your doctors based on your type of cancer. It is important for you to know when your next check cystoscopy is due. This booklet will help you keep track of your medical appointments and treatments. You must contact the hospital if you need to reorganise any of your appointments or have not received notification of your next check up. This booklet contains a section for you to record contact numbers for your treating hospital. 7 Recording of appointments and treatments This section is for you and those looking after you to record visits to the hospital for appointments, check ups and treatments. It helps keep you on track and you are encouraged to keep the book safe and bring it with you whenever you attend. Date 8 Event (e.g. cystoscopy) Results (histology) Treatment resulting Next follow up Date Event (e.g. cystoscopy) Results (histology) Treatment resulting Next follow up 9 Date 10 Event (e.g. cystoscopy) Results (histology) Treatment resulting Next follow up Date Event (e.g. cystoscopy) Results (histology) Treatment resulting Next follow up 11 Date 12 Event (e.g. cystoscopy) Results (histology) Treatment resulting Next follow up Side effects and problems Use this section to record any side effects or problems you are having with your bladder cancer treatments. Date Problem Detail of any current treatment (e.g. BCG) What is the outcome 13 Glossary Adenocarcinoma: A type of malignant cancer cell. and can be performed in the Cystocopy suite. BCG (Bacillus CalmetteGuerin): An intravesical treatment shown to be useful in the management of non muscle invasive bladder cancer. The BCG stimulates the body’s immune systems to destroy the cancer cells. Grade: Refers to the aggressiveness of the cancer. Benign: A non-cancerous growth/lump of normal tissue. Catheter: A flexible tube inserted into your bladder via your urethra to instill fluid as well as drain urine. CIS (Carcinoma In Situ): A flat looking early stage of cancer affecting the lining of the bladder. Cystoscopy: A telescope that is inserted through the urethra in order to view the inside of the bladder. A Rigid Cystoscopy requires the use of a General Anaesthetic and is performed in the Operating Theatre, whereas the Flexible Cystoscopy requires a Local Anaesthetic 14 Histology: The microscopic study of the special staining of tissue specimens to determine the nature of the cells. Intravesical: Medication inserted into the bladder through the urethra. Invasive cancer/disease: A cancer that has spread beyond the layer of cells where it first developed into adjacent tissues. Malignant: A tumour which shows uncontrolled growth and may invade and spread to other parts of the body destroying normal cells. Mitomycin C: A type of intravesical chemotherapy shown to be useful in the management of non muscle invasive bladder cancer. Non muscle invasive cancer/ disease: A cancer that does not extend to the muscle layer of the urinary bladder. Pathologist: A doctor who specialises in the diagnosis and classification of diseases using laboratory tests. Tuberculosis: Respiratory disease of the lungs. Squamous cell Carcinoma: A type of malignant cancer cell. Tumour: A group of abnormal cells (benign or malignant) that may be found in lumps within the body. Transitional cells: The type of cells that make up the bladder lining. Urethra: The tube leading from the bladder where urine passes to the outside of the body. T Stage: T refers to the size of tumour. It is used to define how far a tumour has spread in the bladder. Urologist: Specialist doctor that manages patients with urological symptoms, problems and diseases. References and information source: Figure 1 The Cancer Council New South Wales, (2007). Understanding Bladder Cancer: A guide for people with cancer, their families and friends. Woolloomooloo, NSW: The Cancer Council. Available online from The Cancer Council website: http://www. cancercouncil.com.au Figure 2 CancerHelp UK., (2009). Diagram showing the T stages of bladder cancer. Available from: http://www.cancerhelp.org.uk/ type/bladder-cancer/treatment/bladder-cancer-stage-and-grade Accessed: 19/1/2011 A printed version of the Understanding Bladder Cancer booklet is available from The Cancer Council within Australia. Ph: 13 11 20 15 Useful Contacts and Websites: WA Cancer and Palliative Care Network If you would like to talk to the Urology Cancer Nurse Coordinator. Monday to Friday 8:30 am - 4:30 pm Phone: (08) 9222 0202 http://www.healthnetworks.health.wa.gov.au/cancer/home/ healthdirect Australia 24 hour health advice line Phone: 1800 022 222 Cancer Council WA 24 hour helpline Phone: 13 11 20 http://www.cancerwa.asn.au/ This care diary has been developed for use by patients with non-muscle invasive bladder cancer by the WA Cancer and Palliative Care Network and in consultation with the Australia and New Zealand Urological Nurses Society Incorporated Uro Oncology group. Whilst all efforts will be made to ensure that this record is a true reflection of the current health care plan, it is the responsibility of the patients’ health care providers to ensure treatment plans have considered all appropriate factors within the patients’ history. No guarantee can be given that this document is free from error or omission. Produced January 2011 16 Notes 17 © Department of Health 2011 HP11926A JAN’11 This document can be made available in alternative formats on request for a person with a disability.