Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
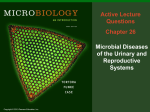
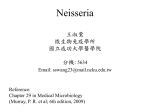
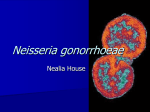
CLASS: 9:00 – 10:00 DATE: October 25, 2010 PROFESSOR: Waites I. II. III. IV. V. VI. Neisseria and Chlamydia Scribe: Adam Baird Proof: Page 1 of 7 NEISSERIA AND CHLAMYDIA [S1] a. Two forms of bacteria will be discussed in this lecture: neisseria and chlamydia OBJECTIVES [S2] a. Specifically, this lecture will cover microbiological characteristics, epidemiology, virulence factors, associated diseases, and laboratory detection of neisseria and chlamydia. i. Neisseira Group 1. Neisseria meningitides 2. Neisseria gonorrhoeae ii. Chlamydia Group 1. Chlamydia trachomatis 2. Chlamydophila pneumoniae 3. Chlamydophila psittaci PICTURE: NEISSERIA MENINGITIDIS [S3] a. Everyone has likely heard of this organism as a cause of meningitis. N. MENINGITIDIS [S4] a. Neisseria meningitidis 1. Oxidase positive a. A closer look at gram-stain smears of body fluids of the neisseria shows that neisseria is frequently found inside of white blood cells (or at least that’s how they appear, because they are readily phagocytosed) 2. Gram-negative coccoid a. Often appears as diplococci (little pairs of organisms together) 3. Capnophilic (meaning they like environments with elevated carbon dioxide, 5 – 7% CO2) a. Note: Neisseria meningitidis is not as fastidious as N. gonorrhoeae, but they both prefer elevated CO2 environments and will grow better in those conditions. 4. Non-motile 5. Grows on chocolate agar and sheep blood agar a. Chocolate agar gets its name because it looks like solidified chocolate pudding. b. Chocolate agar is made from sheep blood agar. The sheep blood agar is heated, which lyses the red blood cells and congeals it, turning the cells brown. c. Chocolate agar is necessary for fastidious organisms that are non-hemolytic to get the nutrients and growth factors in the red blood cells that they need. (Recall: Most of the streptococcus and staphylococcus hemolyze red blood cells. So, streptococcus and staphylococcus grow on the blood agar because they get things out of the red blood cells that they need.) More fastidious organisms do not have the ability to open red blood cells, so they must be put in a medium that already has the red blood cells opened for them so that they can get the necessary nutrients and growth factors. d. Neisseria meningitidis is very adaptable though; it can grow on the chocolate agar and the unsupplemented blood agar (like sheep blood agar) – this is a characteristic that will help distinguish it from more fastidious organisms (that causes gonorrhoeae, for example, which would not grow on unsupplemented blood agar like sheep blood agar.) FIGURE: THE MENINGOCOCCAL CELL WALL [S5] a. Like the gram-positive cocci, there are many components of the microbial cell that help it produce disease. b. The figure shows these various components of the meningococcal cell wall. c. (Review Dr. Yother’s lecture on the difference between gram-positive and gram-negative cell wall components. Recall that gram-positive bacteria have peptidoglycan and that gram-negative bacteria have lipopolysaccharide, which is the endotoxin that specifically contributes to disease.) N. MENINGITIDIS PATHOGENESIS [S6] a. Main Characteristics 1. Lipopolysaccharide (Endotoxin) - Virulence factor of neisseria meningitidis because it is responsible for many of the diseases that the organism causes. More important than any of the other virulence factors of neisseria meningitidis. 2. Capsule – Virulence factor of neisseria meningitidis because it can be used to type the strains. 3. IgA Protease – An enzyme that breaks down IgA. Recall that IgA is an important immunoglobulin that is secreted in the respiratory system. If someone encounters neisseria meningitidis through the respiratory system (which is typical way that it is transmitted), the IgA is one of the first lines of defense, neutralizing the organism and opsonizing it for phagocytosis. But since neisseria CLASS: 9:00 – 10:00 Scribe: Adam Baird DATE: October 25, 2010 Proof: PROFESSOR: Waites Neisseria and Chlamydia Page 2 of 7 meningitidis has the ability to break down IgA, neisseria meningitidis can circumvent the first line of the host immune system defense, allowing it to grow in the host and produce an invasive disease. VII. FIGURE: NO TITLE [S7] a. Neisseria meningitidis pathway: Enters through the nasopharynx (through the respiratory tract). Many times it will only stay in the respiratory tract, but if it is going to cause disease, it will spread into the blood stream; and then if it’s going to cause meningitis (which it does in about half of the cases that it enters the blood stream), it will cross the blood-brain barrier (it has a particular tropism for the central nervous system). VIII. N. MENINGITIDIS SEROTYPES [S8] a. Like many microorganisms, different strains of neisseria meningitidis can be categorized based on antigens that are on the polysaccharide capsules. This helps in identifying the type of neisseria meningitidis and is the basis for the vaccines that are used against neisseria meningitidis. b. There are 13 different serogroups (named alphabetically): 1. Serotypes A, B, and C contribute to more than 90% of the global cases of neisseria meningitidis a. Serotype A – Epidemic in developing countries; causes sporadic outbreaks of large numbers of people with meningitis b. Serotype B, C, and Y – Sporadic outbreaks in developed countries (might be more common in the US). IX. PICTURE: COLONY MORPHOLOGY [S9] a. Neisseria meningitidis on chocolate agar. b. Notice large grey, opaque, circles. X. PICTURE: OXIDASE POSITIVE [S10] a. Defining characteristic of neisseria meningitidis: oxidase positive. b. Oxidase, or cytochrome oxidase, is an enzyme marker that is used in organism identification and typing. It’s a very quick way to classify organisms. 1. Positive oxidase result = dark purple result 2. Negative oxidase result = no color result XI. PICTURE: N. MENINGITIDIS CARBOHYDRATE METABOLISM [S11] a. There are several species of neisseria (although this lecture only covers neisseria meningitidis and neisseria gonorrhoeae, because they are major pathogens in humans). Other neisseria species include neisseria mucosa, neisseria submucosa, etc. Many of the other neisseria species are found in the oral cavity as normal flora. Some neisseria species are also found in the lower urogenital tract of women as normal flora. b. Because there are different strains of neisseria, it’s important to distinguish pathogenic neisseria from nonpathogenic neisseria – and there are several different biochemical ways that this can be determined: 1. For example, neisseria meningitidis has a specific carbohydrates metabolism that will distinguish it from neisseria gonorrhoeae. Neisseria meningitidis will oxidize glucose and maltose, whereas neisseria gonorrhoeae will only oxidize glucose. (A simple way to remember this: Neisseria meningitidis oxidizes glucose and maltose. Neisseria gonorrhoeae only oxidizes glucose.) c. These simple sugars (glucose, maltose, sucrose) can distinguish neisseria meningitidis from neisseria gonorrhoeae, but in order to distinguish all of the other neisseria strains, additional biochemical pattern tests are needed. XII. N. MENINGITIDIS EPIDEMIOLOGY [S12] a. In the US: 1. Neisseria meningitidis is the leading cause of bacterial meningitis in older children and young adults. a. The concern for this age group is this: many people might have neisseria meningitidis in their upper respiratory tracts and not be harmed (because the bacteria hasn’t crossed over into the blood stream), but in crowded institutional settings (like in a college dorm, army barracks, or anywhere else many people are in close-contact and breathing the same air), mixing of different serotypes of neisseria meningitidis may occur, leading to neisseria meningitidis outbreaks. This is why the neisseria meningitidis vaccine is recommended for children as they go through school and especially college. b. There are sporadic cases of neisseria meningitidis in the community, although not as often as in crowded institutional settings. 2. Neisseria meningitidis is not a common disease, but it is a significant one due to high fatality rates. Even though there are antibiotics to fight neisseria meningitidis, there is about a 10 -15% mortality rate. This is a dangerous disease though, causing fatality within hours. Someone with neisseria meningitidis might feel fine one morning, start feeling sick in the afternoon, and be dead by the next morning. 3. Neisseria meningitidis afflicts approximately 2,800 people per year in the US. (To put that in perspective, that’s about the number of streptococcus pneumoniae per year in the US.) CLASS: 9:00 – 10:00 Scribe: Adam Baird DATE: October 25, 2010 Proof: PROFESSOR: Waites Neisseria and Chlamydia Page 3 of 7 4. Even if someone with neisseria meningitidis survives, there is an 11 – 19% permanent sequelae risk (abnormal neurological functions, cognitive limitations, sensory limitations, or physical limitations). b. Worldwide: 1. Neisseria meningitidis is the only form of meningitis that causes epidemics (especially in the crowded conditions of developing countries). XIII. GRAPH: INCIDENCE OF CULTURE CONFIRMED MENINGOCOCCAL DISEASE BY AGE GROUP AND YEAR [S13] a. Admittedly, this graph is old information, but it is still relevant, as it shows two peaks of meningococcal disease that occur in certain age groups. 1. Peak at early childhood 2. Peak at young adulthood (high school, college) XIV. N. MENINGITIDIS EPIDEMIOLOGY [S14] a. Humans are the only reservoir for neisseria meningitidis. b. Respiratory droplets or oral secretions spread Neisseria meningitidis from human to human. c. 10 – 15% of people may have neisseria meningitidis for prolonged periods in the form of nasopharyngeal colonization, but because it hasn’t crossed into the blood stream, it doesn’t harm them. It can, however, still be spread to other humans. XV. N. MENINGITIDIS RISK FACTORS [S15] a. Neisseria meningitidis risk factors: 1. Household contact of primary case or carrier 2. Crowing - Boarding school, college dorms, military camps, etc. 3. Socioeconomic status - Lower income families may be exposed to poor sanitary conditions, large crowds of people, etc., potentially exposing them to neisseria meningitidis 4. Exposure to tobacco smoke – Smoking affects the respiratory system and its defense mechanisms 5. Recent viral upper respiratory infection – Can damage the respiratory tract and lower normal defense mechanisms, allowing bacteria to invade more readily 6. Asplenia – The spleen is an important part of the immune system, so if someone doesn’t have a spleen, normal immune defense is hindered, allowing bacteria to invade more readily. 7. Properdin or terminal complement deficiency – Deficiencies in the complement cascade (especially terminal complement components) can heighten the risks of getting neisseria meningitidis. So anytime someone has a second case of meningococcal disease, it is important that their complement system be evaluated, as it is very likely that more than one episode can cause significant deficiencies. XVI. MENINGOCOCAL DISEASE [S16] a. Different types of meningococcal disease: 1. Meningitis – Most serious meningococcal disease 2. Bacteremia – May have it without the meningitis, but for the most part, bacteremia and meningitis come together 3. Meningococcemia (Sepsis) – Including purpura fulminans and Waterhouse-Friderichsen Syndrome (which will be further discussed later in the lecture). This is a condition that affects blood clotting, reduces platelet levels, and causes bleeding over the whole body, causing purpura fulminans or petechia skin rashes and hemorrhaging on internal organs. Hemorrhaging of the adrenal gland is called Waterhouse-Friderichsen Syndrome. 4. Respiratory tract infection 5. Focal infection – Relatively uncommon 6. Chronic meningiococcemia – Relatively uncommon XVII. MENINGOCOCCAL MENINGITIS CLINCAL SYMPTOMS [S17] a. Symptoms of meningococcal meningitis: 1. Headache 2. Stiff neck 3. Photophobia 4. Altered mental status 5. Fever 6. Nausea, vomiting 7. Petechial or purpuric rash 8. Pneumonia XVIII. PICTURE: PETECHIAE AND PURPURA [S18] a. Petechiae are small red dots on the skin that when pressed do not blanch. b. Petechiae can spread to purpura. CLASS: 9:00 – 10:00 Scribe: Adam Baird DATE: October 25, 2010 Proof: PROFESSOR: Waites Neisseria and Chlamydia Page 4 of 7 c. Any time that a child comes into the emergency room with a fever and a headache, it’s important that their skin be carefully examined for rashes. Even a few petechiae can indicate early stages of meningogoccal disease and a lumbar puncture is needed to evaluate the child. XIX. PICTURE: WATERHOUSE-FRIDERICHSEN SYNDROME [S19] a. Waterhouse-Friderichsen is hemorrhaging of the adrenal gland. XX. PICTURE: NEISSERIA MENINGITIDIS [S20] a. Brain of someone who died with neisseria meningitidis. (The skull has been cut off and the dura is being pulled back with the forceps.) The exposed surface of the brain is covered with pus. This causes swelling of the brain, acute inflammation, headaches, etc. Ultimately, endotoxic shock causes circulatory collapse. XXI. MENINGOCOCCAL MENINGITIS PROGNOSIS [S21] a. There are some characteristics that help predict the outcome of the meningococcal meningitis. b. Characteristics associated with a fatal outcome: 1. Shock 2. Purpuric rash 3. Low or abnormal WBC 4. Older than 60 years old 5. Coma c. Characteristics of the 10% that recover: 1. Permanent neurologic disability 2. Hearing loss 3. Limb loss (due to excessive bleeding, clotting, etc.) XXII. PREVENTION OF MENINGOCOCCAL DISEASE [S22] a. There are two ways to prevent meningococcal disease: 1. Chemoprophylaxis after exposure. 2. Vaccination – New conjugate vaccine licensed in 2005. XXIII. MENINGOCOCCAL VACCINE [S23] a. The meningococcal vaccine is recommended for: 1. US Military personnel 2. Children (11-12 years old) 3. People at risk during outbreak 4. Travelers to high risk areas 5. College students 6. Asplenia patients 7. Patients with complement deficiencies 8. Laboratory workers XXIV. VACCINE LIMITATIONS [S24] a. The meningococcal vaccine, however, is not universally active against all meningococcal strains. 1. The meningococcal vaccine does not provide protection against serotype B, for example, as the polysialic capsule of serotype B is not immunogenic. 2. The meningococcal vaccine is not useful in children under the age of two. b. There are now two meningococcal vaccines available in the US: 1. MPSV4 – For people 11-55 years old 2. MCV4 – For people 2-10 years old and people older than 55 years old. This new conjugate MCV4 vaccine may provide longer immunity and reduce carriage, hopefully breaking the epidemiological cycle. XXV. GRAPH: EPIDEMIOLOGY OF MAJOR STDs IN USA [S25] a. Notice that neisseria gonorrhoeae is one of the most prevalent of these sexually transmitted diseases (STD). b. Notice that chlamydia trachomatis is one of the most prevalent too. It will be discussed later in the lecture. XXVI. PICTURE: NEISSERIA GONORRHOEAE [S26] a. Looks just like neisseria meningitidis, but causes a different disease XXVII. NEISSERIA GONORRHOEAE CHARACTERISITICS [S27] a. Neisseria gonorrhoeae characteristics: 1. Kidney-shaped 2. Non-motile 3. Gram-negative diplococci 4. Require specialized medium and incubation conditions for growth. Neisseria gonorrhoeae is more fastidious than neisseria meningitidis, and it requires chocolate agar for growth. XXVIII. NEISSERIA GONORRHOEAE PATHOGENESIS [S28] a. Main Characteristics: CLASS: 9:00 – 10:00 Scribe: Adam Baird DATE: October 25, 2010 Proof: PROFESSOR: Waites Neisseria and Chlamydia Page 5 of 7 1. Venereal or vertical transmission – Because neisseria gonorrhoeae is fastidious, it won’t survive in the environment, so it’s passed via mucus membrane to mucus membrane touching (venereal transmission). Neisseria gonorrhoeae can also be passed during birth from an infected mother to her offspring (vertical transmission). Newborns get eye drops to make sure asymptomatic gonorrhea hasn’t been acquired from the mother. 2. Pili that enhance attachment to cells 3. Opacity (opa) proteins in outer membrane facilitate cell invasion 4. Endotoxin 5. Peptidoglycan – Tissue toxin 6. Intracellular location – Enables it to hide itself from the host immune system 7. IgA protease 8. Antigenic variation – No permanent immunity following infection; Gonorrhea can be acquired over and over again. No vaccines have been effective in fighting it though, because gonorrhea organism has the ability to alter its antigens. The immune system is “tricked”. 9. Penicillin resistant – Plasmid and chromosomal, making it more difficult to treat and subsequently easier to spread. Many people (especially women) don’t know they have it, so they are able to spread it without knowing it. XXIX. N. GONORRHOEAE DETECTION [S29] a. Detection in males: Relatively simple… 1. Collection and gram stain of a urethral discharge. Gram-negative diplococci in PMNs. (Recall: Normal male urethral discharge is sterile. So if there is gram-negative diplococci present and purulent discharge from the tip of the urethra, the only disease it can be is gonorrhea. It can’t be anything else.) b. Detection in females: In the cervix and the lower genital tract, there are several living species of neisseria they just don’t cause any harm. So the detection of neisseria gonorrhoeae is more complicated; a test beyond a gram stain is needed…. 1. A chocolate agar culture with antibiotics is used for neisseria gonorrhoeae detection. There are several types of this medium, but the most commonly used type is called the Thayer-Martin medium. The Thayer-Martin medium has vancomycin (to kill gram-positive bacteria), trimethoprim (to kill gram-negative), amphotericin (to kill yeast); the only organism that can grow in this medium is neisseria gonorrhoeae. Because neisseria gonorrhoeae is a fastidious organism, the culture can’t be cold or dried out; the culture must be warm in order for neisseria gonorrhoeae to grow. It is oxidase positive, it utilizes glucose, and it requires carbon dioxide as well, all of which promote neisseria gonorrhoeae detection. c. Within the last several years, the way that neisseria gonorrhoeae is diagnosed has changed. Today, we use nucleic acid amplification tests, which picks up neisseria gonorrhoeae in a single urine specimen. Urine for neisseria gonorrhoeae can’t be cultured; the urine is too toxic and will kill the bacteria. But a patient’s urine can be collected, sent to the lab, have PCR test run, which will detect neisseria gonorrhoeae. (Nucleic acid amplification tests pick up chlamydia too, which we will discuss later in the lecture.) No pelvic exam or additional evaluations are needed. However, while this is clearly the method of choice in diagnosing neisseria gonorrhoeae, sometimes cultures are required (because the bacteria can affect other parts of the body). XXX. N. GONORRHOEAE DISEASES [S30] a. Cervical/urethral gonorrhoeae has a 20-30% likelihood of transmission rate b. Although women may be asymptomatic, men are rarely asymptomatic and usually have at least some symptoms c. Complications: 1. Arthritis 2. Pelvic Inflammatory Disease 3. Infertility 4. Proctitis – Inflammation of the anus and the lining of the rectum; usually from anal sexual intercourse 5. Pharyngitis – Inflammation of the throat or pharynx; usually from oral sex 6. Ophthalmia Neonatorum – Infection of the ocular tissues of an infant, causing a severe inflammatory response; usually from vertical transmission (from infected mother to child) XXXI. OPHTHALMIA NEONATORUM [S31] a. Neonatal gonococcal ocular infection. (May also be caused by chlamydia, which will be discussed later in the lecture.) b. Acquired by passage through infected birth canal (vertical transmission). c. Newborn’s eyelids are filled with pus. d. The treatment is prophylactic antibiotic drops at birth (which is now part of normal practice for all newborns). CLASS: 9:00 – 10:00 Scribe: Adam Baird DATE: October 25, 2010 Proof: PROFESSOR: Waites Neisseria and Chlamydia Page 6 of 7 XXXII. NEISSERIA GONORRHOEAE PREVENTION [S32] a. No effective vaccine b. Use of condoms c. Education d. Silver nitrate or antimicrobial drops in newborn eyes. (Silver nitrate causes some degree of chemical conjunctivitis; antimicrobial drops are more commonly used now.) XXXIII. PICTURE: CHLAMYDIA TRACHOMATIS [S33] a. Many of the characteristics about neisseria gonorrhoeae are true for chlamydia trachomatis as well, even though they are completely different organisms. XXXIV. CHLAMYDIA TRACHOMATIS CHARACTERISTICS [S34] a. Characteristics: 1. Obligate intracellular pathogens – Meaning that they inside of another host cell in order to complete their life cycle and survive. 2. Lacks peptidoglycan – Because they don’t have peptidoglycan, they are unable to be detected by gram staining 3. Unique intracytoplasmic growth cycle 4. Depend on host for ATP 5. Growth within cytoplasmic inclusion – Prevents phagolysosome fusion, which is how they can survive within the host 6. 15 serovars XXXV. FIGURE: CHLAMYDIA LIFE CYCLE [S35] a. The infection particle of the chlamydia is the elementary body, which is taken up by the host cell (through the eyes, through the lower genital tract, etc.). Newborns can aspirate the chlamydia during birth, resulting in pneumonitis (inflammation of the lung tissue). b. Once the infectious elementary body enters the cells and is taken up by the host’s phagosomes, then the metabolically active reticulate bodies are released inside the phagosome. The reticulate bodies replicate inside the host cells and then change back to elementary bodies (over the course of about three days). The elementary bodies are finally released from the host cell, and the host cell dies (resulting in inflammation and necrosis). XXXVI. CHLAMYDIA TRACHOMATIS PATHOGENESIS [S36] a. Ocular Infections 1. PMNs monocytes macrophages plasma cells lymphoic follicles fibrosis, scarring b. Genital Infections 1. Organism is attached to mucosal epithelium, induces inflammation and discharge c. Chlamydia is not as pyogenic as neisseria gonorrhoeae, but has a more watery discharge instead. d. Inflammation results with chlamydia, but not nearly as much as with neisseria gonorrhoeae. e. Chlamydia is not nearly as potent as neisseria gonorrhoeae. f. Chlamydia, then, is more difficult to detect than neisseria gonorrhoeae because it doesn’t have as pronounced symptoms. XXXVII. CHLAMYDIA TRACHOMATIS DETECTION [S37] a. There are several ways that chlamydia trachomatis can be detected: 1. Cell Cultures – Stain inclusions with monoclonal antibodies; Secretions are collected from the infected patient, added to cell cultures, and put in a centrifuge, forcing the cells to take up chlamydia. The product would be incubated and then stained. This process really isn’t used for urogenital specimens, although non-urogenital specimens sometimes use this method. Takes several days… 2. Nucleic Acid Amplification – The current method of choice, because it’s faster than cell cultures, even though it’s more expensive. 3. Antigen Detection – Less expensive than nucleic amplification, but less sensitive. XXXVIII. OCULAR TRACHOMA [S38] a. Ocular trachoma is completely distinct from the urogenital trachoma b. One of the most common causes of blindness worldwide. 400 million children and adults worldwide are affected by it. c. Ocular trachoma is spread by touch; it is most common in developing countries where sanitation is not good. d. Results in follicular keratoconjunctivitis (cloudy vision, poor acuity, and a chronic red eye), ultimately leading to blindness if not treated. e. Chlamydia trachomatis serovars A, B, Ba, and C XXXIX. NEONATAL INFECTIONS DUE TO C. TRACHOMATIS [S39] a. Inoculation at birth from infected mothers can lead to: 1. Inclusion keratoconjunctivitis CLASS: 9:00 – 10:00 Scribe: Adam Baird DATE: October 25, 2010 Proof: PROFESSOR: Waites Neisseria and Chlamydia Page 7 of 7 2. Pneumonitis XL. C. TRACHOMATIS GENITAL DISEASE IN ADULTS [S40] a. One of the most common STDs b. Other genital disease associated with trachomatis: 1. Cervicitis in women 2. Non-gonococcal urethritis in men c. Complications 1. Infertility 2. Ectopic Pregnancy 3. Salpingitis – Infection and inflammation of the fallopian tubes d. Many women are asymptomatic XLI. LYMPHOGRANULOMA VENEREUM [S41] a. Another disease caused by chlamydia tachomatis (specifically serovars L1, L2, L3) b. Inguinal lymphatic involvement with obstruction (resulting in inflammation) c. Much less common than chlamydial urethritis d. Occurs more commonly in homosexual males XLII. PREVENTION OF C. TRACHOMATIS INFECTIONS [S42] a. No effective vaccine b. No protective immunity following infections c. Prevention methods: 1. Improve socioeconomic and hygiene conditions 2. Education XLIII. CHLAMYDOPHILA PSITTACI [S43] a. Psittacine family of birds includes are parrots and parakeets b. Chlamydophila psittaci (also known as “Parrott Fever”) is a disease of parrots and parakeets that can sometimes be transmitted to humans via bird droppings, resulting in respiratory infections (pneumonitis) c. Detected by an antibody response d. Serologic diagnosis XLIV. CHLAMYDOPHILA PNEUMONIAE XLV. [S44] a. Discovered accidentally as a new species in 1980s, as it was causing positive test for chlamydophila psittaci. This was because the antibody test was not sufficient to distinguish between the two types. It was then determined that chlamydohila pneumoniae was different type of chlamydia, even though it has the same type of life cycle. b. Transmitted from human to human; no birds are involved. c. It’s a cause of an acute lower respiratory infection (like sinusitis, pharyngitis, pneumonia, etc.) d. Frequently asymptomatic e. Detected by PCR, cell structure, serology f. Diagnostic testing not widely available g. Chlamydophila pneumoniae is able to hide from the immune system too, so it may have a relation to other chronic inflammatory conditions such as atherosclerosis and coronary artery disease [End 48:49 mins]