Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
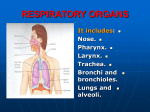
Nasal Drug Delivery Dr Mohammad Issa 1 Nasal physiology The nasal cavity is divided by the nasal septum (comprised of bone and cartilage), with each half opening at the face (via the nostrils) There is also a connection to the oral cavity provided by the nasopharynx The lateral walls comprise a folded structure (refered to as the nasal labial folds or conchae) providing a total surface area of about 150 cm2 in humans The three main areas of the nasal cavity are: The anterior and the posterior vestibules The respiratory region The olfactory region 2 Nasal physiology 3 Nasal physiology The epithelial tissue within the nasal cavity is relatively highly vascularized, and thus provides a potential conduit for drug delivery The cellular makeup of the nasal epithelial tissue consists mainly of ciliated columnar cells, non-ciliated columnar cells, goblet cells and basal cells, with the proportions varying in different regions of the nasal cavity Ciliated cells facilitate the transport of mucus towards the nasopharynx. Basal cells, which are poorly differentiated, act as stem cells to replace other epithelial cells. Goblet cells, which contain numerous secretory granules filled with mucin, produce the secretions that form the 4 mucus layer Nasal delivery: Local delivery Intranasal administration of medicines is the natural choice for the treatment of topical nasal disorders. Among the most common examples are antihistamines and corticosteroids for rhinosinusitis, and nasal decongestants for cold symptoms In these cases, intranasal route is the primary option for drug delivery because it allows a rapid symptom relief with a more favorable adverse-event profile than oral or parenteral routes 5 Nasal delivery: Local delivery In fact, relatively low doses are effective when administered topically, minimizing simultaneously the potential of systemic toxic effects. Recently, for instance, topical antibiotherapy has been considered in chronic rhinosinusitis in an attempt to eradicate biofilm bacteria, often resistant to systemic treatment, and still avoiding systemic toxicity 6 Nasal delivery: Systemic delivery This route is easier and more comfortable for the patient than the parenteral route and it avoids enterohepatic recirculation and gut enzymes This naturally makes it attractive for the delivery of peptides and recombinant DNA technology However, absorption rates fall off sharply when the molecular weight exceeds 1000 Daltons which probably explains why desmopressin is delivered successfully (m. w. 1069 Daltons), whilst insulin (m. w. 6000 Daltons approx.) is not 7 Nasal delivery: Systemic delivery The nasal mucosa demonstrates typical absorption mechanisms. Water soluble drugs enter via passive diffusion through aqueous channels. As the diffusion path through the nasal mucosa is short, intranasally administered drugs demonstrate a rapid rise to peak plasma concentrations, but the rapid clearance from the mucosa limits available time for absorption Amino acids such as tyrosine and phenylalanine are absorbed by active transport, presumably by similar mechanisms to those observed in the blood brain barrier 8 Nasal delivery: Systemic delivery Currently, commercial products which utilize this route for systemic delivery exist for some gonadorelin analogues, which are hypothalmic hormones These include buserelin for prostatic cancer, oestradiol dependent endometriosis and infertility, and nafarelin also for endometriosis and infertility Other commercial products includes desmopressin for diabetes insipidus and primary nocturnal enuresis and lypressin for diabetes insipidus 9 Nasal delivery: Systemic delivery -Penetration enhancers The drive to increase the absorption of large molecular weight molecules has lead to the use of penetration enhancers Bile salts, e.g. sodium deoxycholate, sodium glycocholate and sodium taurocholate, decrease the viscosity of mucus and create transient hydrophilic pores in the membrane bilayer EDTA, and fatty acid salts such as sodium caprate and sodium laurate, increase paracellular transport by removal of luminal calcium, thus increasing permeability of the tight junctions 10 Nasal delivery: Systemic delivery -Penetration enhancers Non-ionic detergents e.g. Laureth-9 alter membrane structure and permeability It should be remembered that the penetration enhancers are generally nonspecific and there remains the potential that any large molecule can enter the systemic circulation once the epithelial barrier is breached Some penetration enhancers, e.g. Laureth-9 and bile salts, have been reported to be toxic to the nasal mucosa 11 Nasal delivery: Systemic delivery -Penetration enhancers Cyclodextrins have been used as solubilizers and absorption enhancers for nasal drug delivery Methylated ß-cyclodextrins have been used to promote absorption of peptides and proteins, but mainly in animals Limited studies show that the cyclodextrins are well tolerated in humans 12 Nasal delivery: vaccination route Advantages include: highly vascular mucous membranes, low enzymatic degradation compared to oral vaccines, and greater acceptability to patients Disadvantages: mucociliary clearance and inefficient uptake of soluble antigens. Therefore, nasal vaccines require potent adjuvants and delivery systems to enhance their immunogenicity and to protect their antigens It is important to note that even for active antigens, intranasal delivery may not elicit an immune response in the absence of an effective adjuvant 13 Nasal delivery: vaccination route Presentation of a suitable antigen with an appropriate adjuvant to the nasal-associated lymphoid tissue (NALT) has the potential to induce humoral and cellular immune responses This approach may be a particularly effective approach to achieving rapid mass immunization, for instance in children and/or in developing countries and disaster areas Intranasal immunization may lead to development of local, as well as systemic, immunity. 14 Nasal delivery: vaccination route Vaccination via the intranasal route does not require a sterile product or a sterile dosing technique (a distinct advantage in developing areas of the world). An example of an intranasal vaccine is FluMist®, a cold-adapted live influenza virus: This product is given as one or two doses over the influenza season via a syringe sprayer 15 Nasal delivery: vaccination route Additional examples of human efficacy testing of intranasal vaccines includes those targeted against adenovirus-vectored influenza proteosome-influenza influenza A influenza B meningococcal outer membrane vesicle a combination respiratory syncytial virus (RSV) and parainfluenza 3 virus (PIV3) live, attenuated intranasal vaccine Effective nasal immunization requires an effective antigen and/or a potent mucosal adjuvant or carrier 16 Mechanisms to increase nasal residence time of formulations Two basic approaches have been used to increase the nasal residence times of drugs: to use viscosity enhancers such as hydroxypropylmethylcellulose and methylcellulose to use a “bioadhesive” excepients such as albumin, Sephadex, starch, dextran, hyaluronan, and chitosan Chitosan has been shown to exhibit advantages as a vaccine carrier due to its immune stimulating activity and bioadhesive properties that enhance cellular uptake, permeation and antigen protection, as well as being well tolerated by humans 17 Intranasal drug delivery to the central nervous system Drugs delivered intranasally are transported along olfactory sensory neurons to yield significant concentrations in the CSF and olfactory bulb Small molecules such as cocaine and cephalexin can be transported directly to the CNS from the nasal cavity Cephalexin preferentially entered the CSF after nasal administration compared to intravenous (IV) and intraduodenal administration in rats. The levels of cephalexin in CSF were 166-fold higher 15 minutes after nasal administration than those of the other two routes 18 Intranasal drug delivery to the central nervous system The ratio of the methotrexate AUCCSF value between the intranasal route and the IV injection was over 13-fold A number of protein therapeutic agents, such as neurotrophic factors and insulin, have been successfully delivered to the CNS using intranasal delivery in a variety of species Insulin-like growth factor I (IGF-I) could be delivered to the brain directly from the nasal cavity, even though IGF-I did not cross the BBB efficiently by itself. As a consequence, intranasal IGF-I markedly reduced infarct volume and improved neurological function following focal cerebral ischemia 19 Intranasal drug delivery to the central nervous system Research in humans has also provided evidence for direct delivery of therapeutic agents to the CNS from the nasal cavity. CNS effects of intranasal insulin in humans was demonstrated without altering plasma glucose or insulin level Intranasal administration is a promising approach for rapid-onset delivery of medications to the CNS bypassing the BBB. 20 Intranasal drug delivery : limitations One of the biggest limitations is insufficient drug absorption through the nasal mucosa. Many drug candidates cannot be developed for the nasal route because they are not absorbed well enough to produce therapeutic effects Another limitation concerning nasal administration is that a small administration volume is required, beyond which the formulation will be drained out into the pharynx and swallowed 21 22