Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
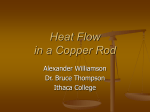
Paradoxical Embolism* An Underrecognized Problem Robert Ward, MD; David Jones, MD; and Edward F. Despite reports of the clinical presentations and dev¬ astating consequences of paradoxical embolus (PDE) to be for more than a century, this diagnosis continues missed. Because the prevalence of patent frequentlyovale foramen (PFO) is 27 to 35% in the normal pop¬ ulation and the presence of deep vein thrombosis or may not be clinically obvious, a pulmonary embolus in the event of un¬ high suspicion for PDE is needed contrast echocar¬ While occlusion. arterial explained and transcranial Doppler ultrasound have diography clinical facilitated recognition of PDE, the optimum clarification. Primary approachforto diagnosiswithrequires is PDE anticoagulation, with therapy patients selected individ¬ in considered carefully thrombolytics uals, but there is little published information regard¬ ing long-term treatment and outcomes. Prevention remains essential whenever possible. It is not yet de¬ "C^irst described by Cohnheim1 in 1877, paradoxical -*" embolism (PDE) was defined as a venous throm¬ bosis causing systemic embolization through a rightto-left shunt. Multiple autopsy-proven cases were de¬ scribed in the French and German literature until 1930 when two patients diagnosed during life were report¬ ed.23 Since then, over 170 cases have been report¬ ed,4"13 with increasing numbers recognized antemortem.5,7'9"17 Recent investigations of patients with pe¬ cerebral arterial emboli ofunknown cause ripheral and PDE is a potentially treatable problem that suggest that occurs more often than usual. We report four pa¬ tients with PDE, two of whom were diagnosed antemortem, and review the literature. Case Reports Case 1 A 30-year-old woman (gravida 2, para 1) was hospitalized while in labor at 40 weeks' gestation. During delivery, she became cyan- otic, apneic, and pulseless. Cardiopulmonary resuscitation was be¬ gun and an endotracheal tube was inserted. A viable 9 lb 10 oz in¬ fant was delivered via forceps. The patient developed ventricular fibrillation and underwent defibrillation with conversion to sinus rhythm but remained hypotensive. Arterial blood gas values dem¬ onstrated a profoundly increased alveolar-arterial O2 pressure dif¬ ference with a pH of 7.40, PaC02 of 9 mm Hg, and Pa02 of 168 mm Hg while breathing 100% O2. Initial chest roentgenogram *From the Section on Pulmonary and Critical Care Medicine, Bowman Gray School of Medicine, Winston-Salem, NC. Haponik, MD, FCCP fined whether prophylactic treatment of persons with recognized predispositions to PDE (eg, PFO and pul¬ monary hypertension) is beneficial. (CHEST 1995; 108:549-58) AFE=amniotie fluid embolism; ASD=atrial septal defect; CXR=chest x-ray; DVT=deep venous thrombosis; IVC= inferior vena cava; LA=left atrium; PAP=pulmonary ar¬ tery pressure; PDE=paradoxical embolus; PE=pulmonary embolus; PFO=patent foramen ovale; RA=right atrium; atrial pressure; RV= right ventricle; TCD= RAP=right transcranial Doppler; TEE=transesophageal electrocar¬ diogram; TTE=transthoracic echocardiogram Keywords: cryptogenic stroke; paradoxical embolus; patent foramen ovale; pulmonary embolus; transcranial doppler; transesophageal echocardiogram (CXR) was normal and ECG revealed S-T segment elevation in anterolateral leads. Laboratory studies included a platelet count of 81,000/mm3 and prolonged prothrombin and partial thromboplastin times. A transthoracic echocardiogram (TTE) showed increased echogenicity in the inferior vena cava (IVC) and right atrium (RA), which was believed to represent thrombus, and the patient received thrombolytic therapy. On transfer to our center the patient remained hypotensive, with persistent coagulopathy, bleeding, and ECG changes. An intraaortic balloon pump was inserted, and cardiac catheterization showed occlusion of the left anterior descending coronary artery. Left ven¬ tricular function was reduced and there was no evident thrombus. Coagulopathy and shock continued despite maximal support and the patient died. At autopsy,18 a cervical tear and disrupted muscular wall were found. No atrial or coronary thrombi were seen, but cardiac examination showed necrotic myocardium in the ante¬ rior left ventricular wall. The microvasculature in this region and both lungs contained scattered squamous cells consistent with amniotic fluid emboli (AFE) (Fig 1). A pencil-thick 0.8-cm patent fo¬ ramen ovale (PFO) was found (Fig 2). Case 2 A 49-year-old woman presented with a pulseless, cold left hand 10 days after open reduction of a left tibia-fibula fracture. She un¬ derwent thrombectomy of the left brachial and axial arteries. The TTE suggested a left atrial thrombus. After heparinization, the pa¬ tient was transferred to our ICU with an enlarging hematoma of the left arm. Physical examination revealed stable vital signs, a medial incision of the left upper extremity with a large hematoma and a left palsy. Irrigation and debridement of the arm were was continued. Transesophageal performed anticoagulation revealed a PFO with echocardiogram (TEE) with saline infusion thrombus but no intraatrial shunt, (Fig 3). Lower ex¬ right-to-left tremity duplex Doppler showed no deep vein thrombosis (DVT). On the third postoperative day, the patient developed hypoxemia and left-sided pleurisy. Arterial blood gas determination revealed a basilar atelectamedian nerve and Pa02 of 67 mm Hg (FIo2, 0.6). The CXR showed CHEST /108 / 2 / AUGUST, 1995 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 549 J?A A It fr' 7 fell* fei?^ * 4/ .;<^Tft:< . la lit mm .' ^ %&'**'5 *JK8§ perfusion lung scan was indeterminate. Pulmonary arteriogram demonstrated multiple bilateral pulmonary emboli (PEs) and elevated pulmonary artery pressures (PAPs) (50/19 mm Hg). An inferior vena cavagram was performed, a "bird's nest" filter was inserted and the patient recovered uneventfully. After 1 week, duplex Doppler studies remained negative, and she was discharged on a regimen of warfarin therapy. sis, and a ventilation Case 3 A 53-year-old woman with hypertension and obesity with acute respiratory failure was transferred to our institution. She had been hospitalized for 11 days previously with right upper lobe pneumo¬ nia and now had vomiting and headache and had trouble keeping her balance. In the emergency room, she developed a left progressively dyspneic, hemiparesis and right facial droop, became and was intubated. Arterial blood gas determination revealed a pH of 7.47, PaC02 of 42 mm Hg, Pa02 of 29 mm Hg while breathing room air, and after intubation fraction of inspired oxygen [FIo2], 1.0; positive end-expiratory pressure, 10 cm H20), apH of 7.58, PaC02 of 29 mm Hg, and a Pa02 of 31 mm Hg. At transfer, examination revealed a blood pressure of 132/65 mm Hg, constricted, reactive pupils, and no papilledema. There were faint bilateral wheezes. The heart had a regular rate and rhythm with a 3/6 systolic murmur along the left sternal border. The patient Figure 2. A probe is placed through a PFO which is adjacent to (Courtesy of P.E. Lantz, MD, Bowman Gray School of Medicine, Wake Forest University.) the RA. case 1, fetal squamous cells demonstrated in an intramyocardial arteriole. Ischemic myocytes are seen lif}^ m ><% I ~j« i, .<* j v adjacent to the arteriole (hematoxylin and ¦k,kVj^ eosin, original magnification x400). l^'-^- "'. Figure 1. In (arrow) were moved all extremities spontaneously and withdrew extremities when pain stimulus was induced. The ECG showed anteroseptal ventricular strain, and CXR myocardial ischemia or possible rightatelectasis. Massive PE was revealed minimal right mid-lung were not administered because of suspected, but anticoagulants a large right parietoneurologic changes. Cranial CT confirmed area adjacent to the atrium of the lateral right occipital, hypodense ventricle (RV), mass effect, and associated edema. Lumbar punc¬ ture showed no infection or bleeding. The TTE revealed an ejec¬ tion fraction of 60%, RV volume and pressure overload with RA, paradoxical septal movement, and tricuspid enlarged RV and an atrial septal defect (ASD) could not be but regurgitation, excluded. There were no pericardial effusions, intracardiac masses, or thrombi. Broad-spectrum antibiotics were started for possible sepsis, and the patient worsened with fever (38.8°C), hypotension, and progressive hypoxemia. She died within 48 h. Autopsy showed multiple PEs with associ¬ right coronary occlusion by an embolus, ated infarcts, a cerebral infarct, and a PFO. Case 4 A 49-year-old man was admitted to our institution with left leg pain and swelling. He had a history of mesenteric arterial emboli with bowel necrosis 2 years earlier, left middle cerebral arterial in¬ farction (with negative carotid ultrasound and TTE) 4 months ear¬ lier, right lower extremity DVT, and multiple bilateral segmental defects by perfusion scan 2 months earlier. Medications included and warfarin sodium (Coumadin). The blood phenytoin (Dilantin) mm Hg; heart rate, 80 beats per minute; res¬ pressure was 118/76 26 breaths rate, per minute; and temperature, 38.0°C. The piratory heart had a fixed, split S-2 without murmurs or gallops. The left lower extremity was warm, swollen, and erythematous with a "cord" medial thigh. Neurologic examination showed palpable in theTheleftCXR showed mild cardiomegaly. Arterial blood hemiparesis. gas determination showed a pH of 7.48; Pa02, 60 mm Hg; PaC02, 29 mm Hg. A ventilation perfusion scan was unchanged from pre¬ vious studies. The patient was heparinized, and leg edema improved over 4 to 5 days. The TTE showed RV overload. At right heart catheterization, passage of the catheter tip across the interatrial septum suggested a PFO or a very small ASD. The mean PAP, 44 mm Hg, and right ventricular end diastolic pressures, 10 to 12 mm Hg, were elevated. Hemoglobin oxygen saturations (95%, LA; 65%, RA) did not suggest shunt. Pulmonary arteriogram showed multi¬ ple bilateral defects indicating previous embolization with partial recanalization. 550 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 Reviews Figure 3. Top, A two-dimensional image taken from the transesophageal echocardio¬ gram TEE in case 2 demonstrates saline con¬ trast filling the RA with microbubbles in transit across the PFO (arrow) to the LA. Bottom, The two-dimensional color Doppler image demonstrates blood flow from the RA through the PFO (arrow) to the LA. After 2 weeks of anticoagulation, he underwent a macroaggrea right-to-left shunt. Sub¬ gated albumin cardiac study confirming and on sequently, a caval umbrella was inserted he was discharged a regimen of warfarin. It was concluded that the patient had had PDEs from the venous system to his cerebral circulation and also to his bowel 2 years previously. Six years later when hospitalized for pneumonia, the patient developed small-bowel obstruction and died. At autopsy, a PFO was found. Discussion The courses of these patients exemplify the clinical presentations of PDE and dilemmas in its manage¬ ment. Four elements must be present for PDE: (1) systemic embolism confirmed by clinical, angiographic, or pathologic findings without an apparent source in the left area of the heart or proximal arterial tree; (2) an embolic source within the venous system; (3) an abnormal intracardiac or intrapulmonary communica¬ tion between right and left circulations; and (4) a pressure gradient that promotes right-to-left shunting cardiac cycle. In 1951, Johnson19 "presumptive" in the presence of the first three findings and "proved" if thrombus is lodged within an intracardiac septal defect at autopsy. Sources of Paradoxical Embolus Some restrict their definition of PDE to include only emboli due to thrombotic material,4'5'20,21 whereas others include emboli of any kind.6 Most reports cite venous thrombi from branches of the IVC as the ma¬ jor source. In Loscalzo's review,5 20 patients (66%) had PE diagnosed by high-probability ventilation per¬ fusion scans, angiograms, or both, and 13 (43%) had DVT documented at venography. Recently, Stollberger et al17 reported that 19 of 29 patients (66%) with PFO and arterial embolism (without evident intraarterial or cardiac sources) had DVT at venography; two thirds of the DVT were clinically silent. Thrombogenesis associated with Swan-Ganz catheters has at some point in the categorized PDE as CHEST /108 / 2 / AUGUST, 1995 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 551 been well documented.22 At least two cases6,23 of PDE to a coronary artery have occurred during cardiac catheterization, with thrombus forming along the venous catheter. Unusual PDE have included two cases of fat embolism after long bone fracture,24,25 brain tissue tumor emboli from a ma¬ complicating birth injury,26 teratoma,2 and the current case of AFE. lignant Definitive diagnosis of the latter rare obstetric com¬ fetal squamous plication is based oronvernix demonstrating in the pulmonary vascula¬ cells, mucin, hair, ture at autopsy.27 Extrapulmonary AFE have occurred in capillaries of the heart, kidney, brain, previously small intestine, liver, spleen, pancreas, adrenal glands, gallbladder, and the retina,28"32 attributed primarily to passage of fetal debris via the pulmonary vascular bed. We suspect that initial increased right-sided pressures due to pulmonary AFE predisposed to PDE via a PFO in case ARTERIAL EMBOLUS OF UNCERTAIN CAUSE Stroke orTIA Peripheral Embolus TTE, TTE, Carotid Ultrasound Peripheral Arteriogram, and Abdominal Aortic Ultrasound Diagnostic Diagnostic Diagnostic 1. Eleven cases of paradoxical air embolism have been Accidental introduction of air may com¬ reported.6,33 intravenous injection, hemodialysis, induction plicate of pneumothorax owing to central line placement, trauma, or any surgical procedure where the wound is above the heart (most often during craniotomies per¬ formed with patients in the sitting position). Compli¬ cations include decreased right heart filling (potentially with cardiac arrest), noncardiogenic pulmonary edema, and PEs. With the latter, increased mean PAP and right-heart pressures might predispose to PDE.34 The true incidence of PDE due to air is unknown, and it is controversial whether PDE occurs primarily via the circulation or owing to an intracardiac de¬ pulmonary fect. Among 11 case reports, 5 had intracardiac defects.6,33 Cardiac and Vascular Communications Most PDEs have been associated with a PFO, a finding in all inourwhom patients. Among 25 cases diagnosed the interatrial defect was char¬ antemortem acterized, 18 (72%) had a PFO, 3 had an ASD, 3 had a pulmonary arteriovenous malformation, and one had a ventricular septal defect.5 There also has been a case with Ebstein's anomaly35 and patent truncus arteriosus.23 The PFO has been known to be a very common since 1930, when Thompson and Evans3 finding identified a "pencil patent" defect (0.6 to 1.0 cm in diameter) in 6% of unselected autopsies and a "probe patent" foramen (0.2 to 0.5 cm) in 29%. Although most PDE are associated with the former, some have occurred with a PFO smaller than 0.6 cm.2 Moreover, PFOs have allowed passage of massive emboli that in three cases resulted in aortic occlusion.36 Hagen et al37 found PFO in 27.3% of 965 autopsied hearts. The in¬ cidence and size of PFO did not differ with gender but varied significantly with age: 34.3% occurred in the Diagnostic Non-Diagnostic TEE Contraindicated Figure 4. Potential strategy for diagnosis of patient with arterial embolus of uncertain cause. TIA=transient ischemic attack. PARADOXICAL ARTERIAL EMBOLUS ? Candidate for Anticoagulation IVC Filter Placement Anticoagulation Therapy ? Impending PDE by Echocardiogram JL Yes Consider Intracardiac ? Peripheral Embolus with Limb Viability in Jeopardy No ? Right Atrial Hypertensionand Acute PE Embolectomy, Defect Repair and IVC Filter Placement Consider Thrombolytics and/or Embolectomy Consider Thrombolytic Therapy or Pulmonary Embolectomy if if No Contraindications Indicated No: Eisenmenger's Complex, Other Inoperable Intracardiac Defect, Unresectable Pulmonary AVM, or COPD with Chronic Pulmonary HTN PFO Present: No Further Therapy IVC Filter Placement and Chronic Anticoagulation 1.5:1 Pulmonary to Systemic Bloodflow ASD Present with Surgical Repair after Resolution of PE Figure 5. Potential strategy for management of patients with ar¬ terial PDE. AVM=arteriovenous malformation; HTN= hyperten- 552 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 Reviews first three decades, 25.4% in the 4th to 8th decades, and 20.2% in the 9th and 10th decades. The PFO to 19 mm (4.9 mm, mean) and increased ranged from 1from a mean of 3.4 mm in the first de¬ progressively mm in the 10th, perhaps because smaller cade to 5.8 defects seal with age. Among 30 patients diagnosed life, Loscalzo5 found the mean age to be during 44.3±16.1 years, with a 2:1 female-to-male predomi¬ nance. The precise frequency of PDE complicating PFO is unknown. The PDE occurs in a minority of the 27 to 35% of patients with venous thromboembolic disease who also have a PFO, because normally the foramen ovale is closed by the left atrial pressure-right atrial pressure (RAP) gradient.37 The ASDs are the most common form of congeni¬ tal heart disease in adults, comprising one third of cases. The direction and severity of shunt depends on ASD size, left ventricular and right ventricular com¬ diastole, and the ratio of pulmonarypliance during de¬ to-systemic vascular resistance. Size1 is 2not a major terminant for defects more than to cm.2 Patients with thromboembolism and ASD have a small but definite risk of PDE, depending on the degree of shunt.38 In patients with left-to-right shunt, right-to-left dilutional studies also have shown small right-to-left shunt due to streaming of venous blood from the IVC toward the fossa ovalis and across the defect.39 Even in the absence of ventricular hypertension, the pressure gradient may reverse transiently before or during atrial systole.40 Hunter41 first hypothesized that PDE would be fa¬ cilitated by shunting through the low resistance com¬ munication of a pulmonary arteriovenous malforma¬ tion. The latter are very uncommon, with only 3 PDE reported.5 Thrombosis within the fistula is common and 10% are reported to cause bland and septic cere¬ bral emboli.42 However, there is a 37% incidence of abnormalities ranging from mild sensory neurologic and motor deficits to severe hemiplegia, often ascribed to polycythemia and hypoxia.43 Mechanisms of Right-to-Leji Pressure Gradients The PE is the most common cause of acutely elevated RAP and right-to-left shunt in patients with PFO or ASD, and occurs in at least 60% of PDE (5). The frequency with which PDE occurs in patients with PE is unknown. In the investigation of Sharma and concerning acute hemodynamic alter¬ colleagues44 ations after PE, PAP rose in proportion to the extent of pulmonary vascular obstruction in 21 patients with¬ out preexisting pulmonary vascular disease. Obstruc¬ tion of 25 to 30% of the pulmonary vasculature was associated with pulmonary hypertension, although no patient had a mean PAP over 40 mm Hg despite mas¬ sive (>50%) embolic obstruction. The RAP was ele¬ vated only occasionally for mean PAP less than 30 mm Hg, but it rose consistently for mean PAP more than 30 mm Hg. Similar observations have been made by other investigators.45"47 Such data suggest that in patients without preexisting pulmonary vascular dis¬ ease, acute PE may result in PDE if mean PAP increases to at least 30 mm Hg and there is a 35 to 40% vascular obstruction and an intracardiac pulmonary defect such as an ASD or PFO. When PDE occurs in the absence of PE, chronic lung disease with pulmonary hypertension has usually been present.4 The frequency of PDE in this setting is unknown. In the report of Sharma et al44 on 30 patients with chronic pulmonary vascular disease and acute PE, mean PAP of 40 mm Hg was seen, reflecting preex¬ isting RV hypertrophy. Also, acute elevations of RAP in a Valsalva maneuver or cough have been associated with 15% of PDE cases.5 On release of the Valsalva maneuver, RAP momentarily exceeds left atrial pres¬ sure due to a sudden rush of blood into the RV and has been useful in diagnosing intracardiac defects. In some circumstances, superimposed acute respiratory illness and its treatment may accentuate the potential hazard of PFO: patients with acute respiratory failure who receive positive end expiratory pressure may experi¬ ence shunting across a PFO. Cujec et al48 reported these effects of positive end-expiratory pressure in patients with acute respiratory failure and compared patients with PFO with those without PFO. The TEE showed increased right-to-left shunt in 28% of 46 pa¬ tients; nearly half of these individuals had a PFO. Other causes of elevated RAP facilitating right-to-left shunt include idiopathic pulmonaryhypertension, pul¬ monary valve stenosis, congestive heart failure, after¬ math of an RV infarction, cardiopulmonary bypass, air embolism, and platypnea orthodeoxia.49 Stroke and other neurologic deficits are common in patients with COPD; the role of PDE in those with pulmonary hy¬ pertension is unknown. Sequelae of Paradoxical Embolus As seen in our patients, PDE can have catastrophic review of 30 patients by Loscalzo,5 sequelae. In theemboli included 20 peripheral (49%), sites of arterial 15 cerebral (37%), 4 coronary (9%), 1 renal (1%), and 1 splenic (1%). In addition, PDE have been reported to cause brain abscess.43 The relationship of PDE to embolic stroke, present in two of our patients, merits particular attention. Forty percent of cerebral infarcts are of undetermined cause despite comprehensive evaluation.50 The PDE via a PFO has been suggested persons. In 1988, Webster potential causehalfinofsuch 40 stroke patients less than 40 found that years of age had a PFO, in contrast to only 15% of control subjects. Among 34 patients with cryptogenic 56% PFO. Lechat et al15 found PFO in as a et al stroke, had CHEST /108 / 2 / AUGUST, 1995 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 553 Table 1.Prevalence of Patent Foramen Ovale (by Transthoracic Echocardiogram With Contrast and Valsalva Maneuver) in Stroke Patients Variable Investigation Reference I- DiTullio et al16 Webster et al14 Age, yr (x±SD) <40 Patients, No. 40 20/40 (50) 1/6 (17) NI* 19/34 (56) 6/40 (15) Overall, No. (%) Stroke, determined origin Stroke, cryptogenic controls with risk factors for stroke Stroke, cryptogenic Control subjects (31±6) Lechat et al15 <55(36±10) 60 24/60 (40) 4/19 (21) 6/15 (40)f 14/26 (56) 10/100 (10) 45 11/45 (24) 1/24 (4) NI* (48) 10/21 101 15/101 (15) 6/77 (8) NI* 9/24 (38) *NI=not identified. *Risk factors in this study included mitral valve prolapse, migraine, use of contraceptives. None presented with hypertension or diabetes. +Patent foramen ovale was inversely associated with the presence of hypertension and diabetes, but the number of cryptogenic stroke patients with combination of risk factors and PFO was not specifically provided. 40% of 60 patients aged less than 55 years with stroke 10% of control subjects. In the first PFO prevalence report in older persons with stroke, Di Tullio et al16 evaluated 146 stroke patients of all ages with contrast TTE and found PFO in 18%. Thirty-one percent of vs cryptogenic; these were associated with higher frequencies of PFO in both younger (<55 years; 48 vs 4%; p<0.001) and older (>55 years; 38 vs 8%; p<0.001) patients when compared with those with strokes were identifiable causes of stroke. The differences remained significant after controlling for hypertension and dia¬ betes. These associations of PFO with cryptogenic stroke suggest that a larger proportion of such events maybe secondary to PDE than is generally appreciated (Table 1). Paradoxical coronary embolism is a rare diagnosis first reported by Marchand in 1894.51 In the recent review of 27 cases by Jungbluth et al,6 9 were diagnosed antemortem. Of the 18 thrombotic PDE, the rightto-left communication was via PFO in 13, an ASD in 4, and a patent truncus arteriosus in 1. The remaining cases were caused by air embolism, and an eight abnormal intracardiac defect was found in only three. Five air emboli involved the left coronary artery, per¬ haps related to its anterocranial position. Diagnosis of Paradoxical Embolism potentially devastating effects of PDE, early diagnosis and treatment are essential in order to manage the current event and to prevent re¬ currence. The high prevalence of anatomic (eg, PFO) and hemodynamic (eg, pulmonary hypertension due to acute or chronic respiratory illness or both) predispo¬ sitions to PDE present unresolved diagnostic and dilemmas. The PDE should be suspected therapeutic in any patient with unexplained arterial embolism. Al¬ obvious, simultaneous pulmonary and though clinically embolism should strongly suggest PDE, but systemic it is not prerequisite for the diagnosis. The PE may go Because of the DVTs are often undiagnosed, and as noted previously, also is hindered asymptomatic.17,52 Diagnosis by the variable manifestations of systemic emboli, which also maybe asymptomatic,53 and the presumptive nature of the diagnosis of PDE when it occurs. Moreover, shunt may be transient and occur only right-to-left Valsalva or other inciting maneuvers; if the pa¬ during tient is studied after the acute event, both the PE and the right-to-left shunt may have resolved.9 The weight to assign to coexisting carotid disease in the decision whether or not to pursue PDE as a diagnostic consid¬ eration is also unclear. The differential diagnosis of arterial embolism in patients with temporally associated PE or DVT in¬ cludes (1) cardiomyopathy with right ventricular and left ventricular mural thrombi; (2) emboli from biatrial myxomas; (3) mitral and tricuspid valve disease (with or without atrial fibrillation); (4) myocardial infarction with a left ventricular thrombus and congestive heart failure predisposing to DVT; (5) emboli via right- and left-sided infective endocarditis; and (6) emboli related to prosthetic replacement of both mitral (and/or aor¬ tic) and tricuspid valves.9 In patients with cyanotic heart disease and arterial embolism, PDE is congenital in other settings, the diagnosis may be difficult likely; to establish. Because of the importance of DVT as or¬ igin of PDE, vigorous exclusion of DVT (eg, with contrast venography) assumes special importance in patients with unexplained stroke or other embolic events. Stroke patients with COPD and pulmonary have vigorous assessment for hypertension also shouldcommunication and venous coexisting intracardiac disease. Diagnostic Techniques Before availability of contrast TTE and TEE, many were used to demonstrate right-to-left approaches shunt. Following the use of oximetry to document a drop in oxygen saturation during the Valsalva maneu- 554 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 Reviews ver, in cators the study by Lee and Gilmette,54 various indi¬ including ascorbate, hydrogen, krypton, freon, and indocyanine green were injected into the right side of the circulation, with their early systemic appearance signifying a right-to-left shunt.4'21,55,56 Accurate antecon¬ diagnosis has beenSixfacilitated greatly byPDE of cases echocardiography.57 impending (with the clot visualized within the intracardiac defect), "embolism interruptus," have been reported during life, three each by TTE5,7 and TEE.913 The contrast effect is achieved by microcavitation bubbles produced during rapid injection of 10 mL of agitated contrast solution (eg, 9 mL of saline and 1 mL of air) into a peripheral vein. Various contrast agents may be used, including indocyanine green, dextrose water, normal saline solution, or autologous blood. Usually, contrast TTE is obtained using an apical four-chamber view. At least four saline injections are in quiet breathing and after the Valsalva performed maneuver. The study is considered positive if microbubbles appear either in the LA or left ventricle no later than two to three cycles after their initial appear¬ ance in the RA.58 Another maneuver, the cough test, has been reported to be superior to the Valsalva ma¬ neuver in diagnosis of PFO in TEE.59 Three to five rapid, successive coughs are performed immediately after opacification of the RA with contrast. In 73 con¬ secutive patients, PFO was detected during the cough test in 32 (43.8%), significantly more often than in the Valsalva maneuver (32.9%) or quiet breathing (24.7%). Contrast TTE is more sensitive than oximetry and dye curves, but its sensitivity is only 64%.60 Technical limitations relate to spontaneous variations in right-toleft shunt during normal breathing, the quality of the Valsalva maneuver, uneven distribution of contrast solution, and missing the sampling site of the M-mode beam. Contrast shunting is apparent immediately in patients with cyanotic heart defects but is often subtle in patients with uncomplicated ASD. Contrast shunt¬ ing may become evident during the Valsalva maneuver, but this part of the tracing often is technically unsat¬ and difficult to interpret. The most important isfactory moment is thus the first diastole following the Valsalva maneuver release. The TTE also frequently demon¬ strates echo dropouts because the ultrasonic beams do not generally hit the interatrial septum with a perpen¬ dicular orientation and may result in false-positive ap¬ pearances of ASDs. Since the degree of contrast shunt is independent of defect size, TTE cannot reliably differentiate ASD from PFO.60 By contrast, TEE is unrestricted by lung tissue or thoracic malformations, providing superior imaging of the atrial septum and a clear view of the foramen ovale.61 The prevalence of PFO detected by TEE has ranged from 8 to 63% because of varying study populations, techniques, and defining criteria.14,58"64 In the first mortem trast report validated by catheterization or operative results, Chen and coworkers58 documented PFOs with con¬ trast TTE and TEE in 32 patients. A right-to-left shunt was seen by TEE in 14 in normal breathing and 20 with the Valsalva maneuver and by TTE in 8 with normal and 12 with the Valsalva maneuver. All PFOs breathing seen by TTE were also seen by TEE, and all but one of the PFOs seen by TEE were confirmed by cathe¬ terization or surgery. The false-positive patient had a right atrial myxoma, the highest RAP of the group; shunt was accentuated by presumably, right-to-left "communications other than PFO." The diagnostic sensitivity (100 vs 63%) and accuracy (97 vs 78%) of TEE were higher than with TTE. Although such ini¬ tial observations suggest that TEE provides superior imaging, even in the strain phase, and higher sensitiv¬ ity in the detecting PFO, TEE has the disadvantages of semiinvasiveness, higher cost, and limited availabil- ity. Transcranial Doppler (TCD) ultrasound of the middle cerebral artery in contrast injection is another noninvasive method that may enhance detection of interatrial right-to-left shunt.65 Nemec et al66 com¬ TTE, TEE, and TCD in 32 patients, 21 ofwhom pared had unexplained arterial emboli; TEE showed intera¬ trial shunt in 13 and intrapulmonary shunt in 6. Using TEE as the gold standard, TCD had a sensitivity and of 100% and identified 3 of the intrapul¬ specificityshunts. Thus, TCD provides a useful alterna¬ monary tive for excluding interatrial right-to-left shunt when TEE is unavailable. This role of TCD warrants further investigation because of its wide availability.66,67 Diagnostic Approaches Evaluation Integrated use of these tools in diagnostic evaluation of an arterial embolus varies considerably with insti¬ tutional resources and clinicians' preferences. Because arterial emboli most often originate in the heart or arteries, evaluation often begins with Mproximal mode two-dimensional TTE, arteriogram or abdomi¬ nal aortic ultrasound (for abdominal or lower extrem¬ ity peripheral emboli),59 or carotid ultrasound (for stroke or transient ischemic attack [Fig 4]). If no source is found, or if DVT or PE or both are associated, then contrast TTE with Valsalva maneuver or cough test or contrast TEE rule out (if TTE is negative) are performed to shunt. If TEE cannot be per¬ right-to-left These approaches focus¬ TCD is considered. formed, and the embolus possible intracardiac com¬ ing upon munications should be coordinated with vigorous exclusion of associated venous disease. The optimum, most cost-effective means of detecting PFO requires further clarification. CHEST /108 / 2 / AUGUST, 1995 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 555 Management Issues and Challenges Various therapeutic strategies have been used in patients with PDE (Fig 5). A multifaceted approach is necessary since no single algorithm is appropriate for all individuals; the heterogeneity and complexity of patients, together with their acuity of illness, makes management highly individualized. There are no pub¬ lished investigations comparing patient outcomes or showing the superiority of any one strategy. Most au¬ thorities5,9,36 agree that anticoagulation should be ini¬ tiated immediately on diagnosis of arterial emboli un¬ less there are major contraindications. Interestingly, strategies for long-term management anticoagulation PDE or for these diverse issues related of patients with PDE are seldom addressed. Although to specifically and risk of recurrent emboliza¬ the long-term courses PDE are tion in patients with unknown, it seems rea¬ should have lifelong antico¬ that such sonable patients in of the absence contraindications. Even agulation to difficult is the more approach persons with DVT and a documented intracardiac communication or that to patients with other combinations of predispositions to PDE (eg, PFO and pulmonary hypertension). Prophy¬ lactic anticoagulation appears reasonable in such indi¬ viduals but data documenting its benefit are unavail¬ able. In this regard, the risk posed by echocardiodetected PFO in the absence of PDE graphicallydelineation. Without the benefit of large requires clinical trials, it is unclear whether long-term antico¬ would benefit stroke patients with therapy agulant PFO and no cardiac source of embolism, particularly in the presence of COPD and pulmonary hyperten¬ sion. Because PE is a major problem likely to accompany PDE, its management is another important related is¬ In the special circumstance ofcombined PDE and PE, the greatest danger of further PDE seems to oc¬ cur in the few hours after the initial episode, when RAP is highest. Thus, thrombolytic agents might be con¬ sue. sidered in carefully selected patients with suspected PDE and significant RA hypertension due to PE even when systemic hypotension is absent, in an effort to reduce RAP and the likelihood of recurrent PDE.5,36 Evidence ofcerebral emboli may be a contraindication to thrombolytic therapy, although use of lytic therapy for such cases has been reported.62 Thrombolytics and, pe¬ occasionally, embolectomy are consideredlimbwhen ripheral arterial obstruction jeopardizes viabili¬ ty.36The role of caval interruption in patients with PDE are If unclear. is also thrombolytics or ofanticoagulation filter is an IVC then contraindicated, placementof DVT. in the recommended Occasionally, presence considered. In the rare embolectomy isPDE pulmonary discovered at echo¬ case of an "impending" intracardiac embolectomy may be at¬ cardiography, tempted, together with correction of the intracardiac defect and placement of an IVC filter.5 If PDE occurs via an unresectable pulmonary arteriovenous malfor¬ mation or in the presence of inoperable, irreversible intracardiac right-to-left shunt, then an IVC filter is considered. Long-term anticoagulant administration as well because of the po¬ generally is recommended effects of even very small PDE.36 tentially devastating of the is unnecessary after PDE, closure PFO Usually, if RA particularly to be hypertension and right-to-leftofshunt are thought temporary.36 Surgical repair iso¬ lated ASD has been advocated when the ratio of pul¬ monary to systemic blood flow is 1.5:1. In persons with Eisenmenger's complex (irreversibly elevated mean PAP and right-to-left shunt), surgery is contraindicated because the severe pulmonary hypertension causes heart failure upon closure of the ASD.68 If an ASD patient has a right-to-left shunt due to an acute PE, RA may be self-limited and surgical repair hypertension still be may possible.36 Comment of PDE have been descriptive, pro¬ reports information about its natural history, out¬ viding little comes, and effects of various therapeutic approaches. The long-term management of survivors of the acute PDF is unclear from the literature. More epidemio¬ logic data are needed to delineate these issues. The 27 to 35% prevalence of PFO in the general popula¬ tion,3,37 and the association of cryptogenic strokes with PFOs14"16 suggests that PDE is frequently missed. This impression is supported by the review ofAbuRahma et had a al9 of 41 cases of arterial embolism: 20 Most (49%) cardiac thrombus or other cardiac disease, 7 (17%) had a proximal arterial thrombus by arteriogram or ab¬ dominal aortic ultrasound, 5 (12%) had "possible" or "probable" PDE, and another 9 individuals (22%) had emboli of unknown source after negative or incom¬ plete evaluations. Five of 9 patients (56%) less than 50 years old had "probable" or "possible" PDE. To improve recognition of PDE, clinicians should maintain a high suspicion for this event whenever neurologic changes complicate cardiovascular events, DVT or PE, or any unexplained arterial occlusion oc¬ curs (particularly in young or postoperative patients). When the source of an embolus is not identified by M-mode and two-dimensional echocardiogram, ab¬ dominal ultrasound, or arteriogram, contrast TTE with cough test or Valsalva maneuver should be considered, followed by a TEE or TCD if necessary. The most cost-effective diagnostic strategy remains to be deter¬ mined, and approaches will vary with the institutional resources available to the clinician. Anticoagulation is the mainstay of therapy. Unless contraindicated, a lower threshold for use of thrombolytics may be con¬ sidered in selected cases. It seems reasonable that an- 556 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 Reviews for patients predisposed to PDE should ticoagulation continue as long as the predisposition is present. For many patients (eg, individuals with COPD-induced hypertension, PFO) this recommendation pulmonary would be lifelong. The benefits of this approach are undocumented and require definition before making firm guidelines. Prevention of PDE is especially desirable. Although there is no information regarding specific measures to reduce PDE risk, improved application of already val¬ idated prophylaxis when predispositions to DVT occur in patients with known PFO or other intracardiac communications would appear especially worthwhile. Even less is known if prophylactic anticoagulation of persons with recognized risks for PDE (eg, PFO and chronic pulmonary hypertension) is beneficial. If fu¬ ture reports confirm that PDE occurs as often as the might suggest, then high frequency of predispositions of current thresholds and antico¬ major adjustments In will be the absence of necessary. agulation strategies contraindications, lower thresholds for anticoagulating patients at risk might be needed, but documentation of benefits of this approach may be difficult. References J. Thrombose und Embolie. In: Vorlesungen iiber Allgemeine Pathologie, vol 1. Berlin: Hirschwald, 1877; 134 2 Dahl-Iverson E. Embolie paradoxale de l'artere iliaque externe gauche-embolectomie. Lyon Chir 1930; 1:39-42 3 Thompson T, Evans W. Paradoxical embolism. Quart J Med 1930; 1 Cohnheim 23:135-0. 4 Meister SG, Grossman W, Dexter L, et al. Paradoxical embo¬ lism.diagnosis during life. Am J Med 1972; 53:292-98 5 Loscalzo J. Paradoxical embolism: clinical presentation, diagnos¬ tic strategies, and therapeutic options. Am Heart J 1986; 112: 141-45 6 Jungbluth A, Erbel R, Darius H, et al. Paradoxical coronary em¬ bolism: case report and review ofliterature. Am Heart J1988; 116: 879-85 7 Spechly-Dick ME, Middleton SJ, Foale RA. Impending para¬ doxical embolism: a rare but important diagnosis. Br Heart J 1991; 65:163-65 8 Nelson CW, Snow FR, Barnett M, et al. Impending paradoxical embolism: echocardiographic diagnosis of an intracardiac throm¬ bus crossing a patent foramen ovale. Am Heart J 1991; 122:859-62 9 AbuRahma AF, Lucente FC, Boland JP. Paradoxical embolism: an underestimated entity.a plea for comprehensive workup. J Cardiovasc Surg 1990; 31:685-92 10 Movsowitz C, Podolsky LA, Meyerowitz CB, et al. Patent foramen ovale: a nonfunctional embryological remnant or a potential cause of significant pathology? J Am Soc Echocardiologists 1992; 5:259-70 11 Nellessen U, Daniel WG, Matheis G, et al. 14 Webster MW, Chancellor AM, Smith HJ, et al. Patient foramen ovale in young stroke patients. Lancet 1988; 2:11-12 15 Lechat P, Mas JL, Lascault G, et al. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med 1988; 318:1148-52 16 Di Tullio M, Sacco RL, Gopal A, et al. Patient foramen ovale as a risk factor for cryptogenic stroke. Ann Intern Med 1992; 117: 461-65 17 Stollberger C, Slany J, Schuster I, et al. The prevalence of deep thrombosis in patients with suspected paradoxical embo¬ lism. Ann Intern Med 1993; 119:461-65 18 Prahlow JA, Lantz PE. Amniotic fluid embolism with paradoxi¬ cal embolization. Forensic Pathol 1993; 35:1-4 19 Johnson BJ. Paradoxical embolism. J Clin Pathol 1951; 4:316-32 20 Silverman ME. Paradoxical embolus. N Engl J Med 1993; venous 329:930 Cheng TO. Paradoxical embolism.a diagnostic challenge and its detection during life. Circulation 1976; 53:565-68 22 Hoar PF, Stone JG, Wickes AE, et al. Thrombogenesis associated with Swan-Ganz catheters. Anesthesiology 1978; 48:445-47 23 From AHL, Wang Y, Eliot RS, et al. Coronary arterial embolism 21 following cardiac 24 Pell ACH, Hughes D, Keating J, et al. Brief report: fulminating fat embolism syndrome caused by paradoxical embolism through a patent foramen ovale. N Engl J Med 1993; 329:926-29 25 Etchells in persistent truncus arteriosus, report of a case catheterization. N Engl J Med 1965; 272:1204 EE, Wong DT, Davidson G, et al. Fatal cerebral fat embolism associated with a patent foramen ovale. Chest 1993; 104:962-63 26 Abrikossoff AJ. Zur kasuistik der Parenchymembolien: Kleinhirngewebeembolie der arteria coronaria cordis beim neugeborenen. Zentrabl Allg Pathol 1913; 23:244 27 Clark SL, Pavlova Z, Greenspoon J, et al. Squamous cells in the maternal pulmonary artery circulation. Am J Obstet Gynecol 1986; 154:104-06 28 Liban E, Raz S. A clinicopathologic study of fourteen cases of amniotic fluid embolism. Am J Clin Pathol 1969; 51:477-86 29 Price TM, Baker W, Cefalo RL. Amniotic fluid embolism: three case reports with a review of the literature. Obstet Gynecol Surv 1985; 40:462-75 30 Chang M, Herbert WNP. Retinal arteriolar occlusions following Ophthalmology 1984; 91:1634-37 EP, Taylor HB. Amniotic fluid embolism. Obstet Gynecol 1970; 35:787-93 amniotic fluid embolism. 31 Peterson 32 Attwood HD. Fatal pulmonary embolism by amniotic fluid. J Clin Pathol 1956; 9:38-46 33 Marquez J, Sladen A, Gendell H, et al. Paradoxical cerebral air embolism without an intracardiac defect. J Neurosurg 1981; 55: 997-1000 34 Brogno D, Lancaster G, Rosenbaum M. Embolism interruptus. N Engl J Med 1994; 330:1761-62 1982; JL, Pennington WS, Isobe JH, et al. Paradoxical embolization with Ebstein's anomaly. Arch Surg 1983; 118:1101 Leonard RCF, Neville E, Hall RJC. Paradoxical embolism: a re¬ view of cases diagnosed during life. Eur Heart J 1982; 3:362-70 Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades oflife: an autopsy study of 965 normal hearts. Mayo Clin Proc 1984; 59:17-20 Kopf GS, Laks H. Atrial septal defects and cor triatriatum. In: Baue AE, ed. Glenn's thoracic and cardiovascular surgery. 5th ed, vol 2. East Norwalk, Conn: Appleton and Lange, 1991; 995-1005 Swan HJC, Burchell H, Wood E. The presence of venoarterial shunts in patients with interatrial communications. Circulation 35 Mathews 36 37 38 39 1954; 10:705-13 40 1991; 121:1552-54 13 Venous air embolism. Arch Intern Med 142:2173-76 Impending paradox¬ ical embolism from atrial thrombus: correct diagnosis by transe¬ sophageal echocardiography and prevention by surgery. J Am Coll Cardiol 1985; 5:1002-04 12 Nagelhout DA, Pearson AC, Labovitz AJ. Diagnosis of paradox¬ ical embolism by transesophageal echocardiography. Am Heart J O'Quin RJ. 41 Steiger BW, Libanoff AJ, Springer EB. Myocardial infarction due to paradoxical embolism. Am J Med 1969; 47:995-98 Hunter DD. Pulmonary arteriovenous malformation: an unusual case of cerebral embolism. Can Med Assoc J 1965; 93:662-65 CHEST /108 / 2 / AUGUST, 1995 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 557 Pulmonary hypertension and cor pulmonale. In: Fishman AP, ed. Pulmonary diseases and disorders. 2nd ed, vol 2. New York: McGraw-Hill, 1988; 1043-45 43 Sisel RJ, Parker BM, Bahl OP. Cerebral symptoms in pulmonary arteriovenous fistula. Circulation 1970; 41:123-28 44 Sharma GVRK, Mclntyre KM, Sharma S, et al. Clinical and he¬ modynamic correlates in pulmonary embolism. Clin Chest Med 42 Fishman AP. 1984; 5:421-37 45 Dalen JE, Banas JS, Brooks HL, et al. Resolution rate of acute pulmonary embolism in man. N Engl J Med 1969; 280:1194-99 46 Mclntyre KM, Sasahara AA. The hemodynamic response to pulmonary embolism in patients without prior cardiopulmonary disease. Am J Cardiol 1971; 28:288-94 47 Jardin F, Duboura O, Gueret P, et al. Quantitative two-dimen¬ sional echocardiography in massive pulmonary embolism: em¬ phasis on ventricular interdependence and lefthand septal dis¬ placement. J Am Coll Cardiol 1987; 10:1201-06 48 Cujec B, Polasek P, Mayers I, et al. Positive end-expiratory pres¬ sure increases the right-to-left shunt in mechanically ventilated patients with patent foramen ovale. Ann Intern Med 1993; 119:887-94 49 Seward JB, 50 Hayes DL, Smith HC, et al. Platypnea-orthodeoxia: clinical profile, diagnostic workup, management, and report of seven cases. Mayo Clin Proc 1984; 59:221-31 Sacco RL, Ellenberg JH, Mohr JP, et al. Infarcts of undetermined cause: the NINCDS Stroke Data Bank. Ann Neurol 1989; 25: 382-90 51 Marchand F. Zur Kennthis der embolie und thrombose der Ge- hirnarterien, zugleich ein beitrag zur casuistik der primaren herztumoren und der gekreuzten embolien. Berl Klin Wochenschr 1894; 31:36 52 Moser KM. Venous thromboembolism. Am Rev Respir Dis 1990; 141:235-49 53 Edwards EA, Tilney N, Lindquist RR. Causes of peripheral em¬ bolism and their significance. JAMA 1966; 196:119-24 54 Lee G, Gimlette T. A simple test for interatrial communication. BMJ 1957; 1:1278-81 55 Tracy GP, Smulyan H, Potts JL, et al. One angiographic diagno¬ sis of patent foramen ovale in paradoxical embolism. Catheter¬ ization Cardiovasc Diagnosis 1976; 2:137-42 56 Banas J, Meister S, Gazzaniga A, et al. A technique for detecting small defects of the atrial septum. Am J Cardiol 1971; 28:467-71 57 Valdez-Cruz LM, Pieroni DR, Roland JMA, et al. Echocardio¬ of intracardiac right-to-left shunts following graphic detection vein peripheral injections. Circulation 1976; 54:558-62 58 Chen W, Kuan P, Lien W, et al. Detection of patent foramen ovale by contrast transesophageal echocardiography. Chest 1992; 101:1515-20 59 Stoddard MF, Keedy DL, Dawkins PR. The cough test is supe¬ rior to the Valsalva maneuver in the delineation of right-to-left ovale during contrast shunting through the patent foramen Am Heart J 1993; 125:185-89 transesophageal echocardiography. 60 Kronik G, Slany J, Moesslacher H. Contrast M-mode echocardi¬ ography in diagnosis of atrial septal defect in acyanotic patients. Circulation 1979; 59:371-78 Langenstein BA, et al. Detection of osseptal defects by transesophageal crosssectional echocardiography. Br Heart J 1983; 49:350-58 62 Wittlich N, Kramer M. Diagnosis of patent foramen ovale by transesophageal contrast echocardiography [abstract]. Circula¬ 61 Hanrath P, Schliiter M, tium secundum atrial tion 63 Lee 1988; 78:11-441 RJ, Bartzokis T, Yeoh T, et al. Enchanced detection of int¬ sources of cerebral emboli by transesophageal echo¬ cardiography. Stroke 1991; 22:734-39 64 Archer SL, Kvernen LR, James K, et al. Does warfarin reduce the atrial fibrillation? a prevalence of left atrial thrombus in chronic double blind, placebo controlled study. Circulation 1991; 84:11693 65 Teague SM, Sharma MK. Detection of paradoxical cerebral echo contrast embolization by transcranial doppler ultrasound. Stroke racardiac 1991; 22:740-45 66 Nemec JJ, Marwick TH, Lorig RJ. Comparison of transcranial and transesophageal contrast echocardiog¬ Dopplerin ultrasound of interatrial right-to-left shunts. Am J the detection raphy Cardiol 1991; 68:1498-1502 67 Herderschee D, Limburg M, Hijdra A, et al. Recombinant tissue basilar artery occlusion. plasminogen activator in two patients with 54:71-3 Neurol 1991; Neurosurg Psychiatry J 68 Borow KM, Karp R. Atrial septal defect: lessons from the past, directions for the future [editorial]. N Engl J Med 1990; 323:1698-1700 simple 558 Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21718/ on 05/10/2017 Reviews