Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
PUBLICATION OF THE SUPERIOR HEALTH COUNCIL No. 8858
Red meat, processed red meats and the prevention of colorectal cancer.
In this science-policy advisory report, the Superior Health Council provides an assessment of
the risk of developing bowel (colorectal) cancer attributed to the consumption of red meat and
of processed red meats; based on this evidence recommendations are given to prevent this
disease.
4 December 2013
SUMMARY
1.
Introduction
The potential for the prevention of different non-communicable chronic diseases through the
consumption of a healthy well-balanced diet is overwhelming and should complement the health
gains that are efficiently achieved through food safety measures. The latter have reached a high
degree of security because of legally compelled and efficient control. The former has received
unfortunately insufficient attention.
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in the world and in
Belgium. Its incidence is highest in the developed world and differences in incidence rates are
much larger than differences in mortality rates. The differences in incidence rates are mainly
related to dietary factors.
Key references: Pacolet et al, 2011; Ferlay et al, 2010; van Leeuwen, 2006; European Commission, 2010;
Anand et al, 2008.
2.
Research evidence
Since 1975, epidemiological evidence has been accumulating linking the consumption of red
meat to the incidence of colorectal cancer (CRC), a disease that is more common in
developed countries. This association has been observed for home prepared and cooked
fresh meat as well as for processed red meat products. Although the literature is not always
clear, the term “red meat” in this report refers to fresh red meats (mainly beef, pork, sheep or
lamb but also other meats except poultry meat) that have not been subjected to other
treatments than cooling, freezing and/or comminution for mixing with other red meats and
salt (e.g. ground meat). Processed red meat products are defined as “meat preserved by
smoking, curing or salting or by addition of chemical preservatives” by the “World Cancer
Research Fund / American Institute for Cancer Research“ (WCRF/AICR) and are here more
simply specified as ”red meats preserved by salting (mainly with addition of nitrite and/or
nitrate) and one or more other treatments”. Very convincing evidence on this association
was obtained in the “European Prospective Investigation into Cancer and Nutrition“ (EPIC)
study and in work summarized and evaluated in the WCRF/AICR report, updated in 2011.
− 1−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
The quality of the latter report has been strengthened by a multidisciplinary task force of
independent experts for collection and review of the literature and by using stringent criteria
to retain studies for review, including:
- only data published in recognized peer reviewed journals (see key references) were
selected;
- testing for heterogeneity of data, the adjustment for co-variates including age, total
energy intake, body mass index, smoking, physical activity, alcohol and other possible
confounders;
- the retention of cohort studies only in order to avoid bias more frequently observed in
case-control studies.
Up to May 2010, 13 cohort studies from 18 publications involving more than 1.500.000
subjects were available and generated a dose-response relationship in meta-analyses of the
association between red meat and processed red meat consumption and the incidence of
CRC.
Some criticisms on the observed results in these previous reports are not convincing mainly
because of questions regarding possible conflicts of interest of the authors, lack of
completeness of data used and lack of precise and coherent definition of processed red
meats used. Three large prospective studies involving a total of about 220.000 subjects did
not observe a relation between red and/or processed red meat consumption and CRC risk.
This lack of confirmation could be linked to the low intake range of red and/or processed red
meat involved, the unexpected all-cause mortality rates in the cohorts, the special social
status (health consciousness) and age range and the different ethnicities in the populations
studied.
Relevant approximate summary relative risk (RR) of CRC from the WCRF/AICR report is:
1,20 for the consumption of 50 g/d of processed red meat and of 100 g/d of red meat. Such
increase in risk has a meaningful population effect on public health, though limited when
considered for the individual. Both French and UK official guidelines have been published
advocating a reduction of both red and processed red meat consumption in reference to a
recognized increased risk of CRC.
It should be realized that the reversibility of the risk related to red and processed red meat
consumption has never been tested. Indeed, this would require randomized controlled
clinical trials with the incidence of CRC as outcome measure involving exacting
experimental requirements in terms of individuals, duration as well as control and
specification of food consumption. Such trials are very hard to achieve although intervention
trials are feasible and showed that a low-fat dietary pattern did not reduce the risk of
colorectal cancer in postmenopausal women.
Key references: Chan et al, 2001; Norat et al, 2002; Demeyer et al, 2008; WCRF/AICR, 2011; Programme
National Nutrition Santé, France, 2009; Scientific Advisory Committee on Nutrition, UK, 2010.
3.
Situating the risk within the context of other risk factors
CRC incidence is predominantly related to environmental risks mainly involving diet. Genetic
variants of genes associated with xenobiotic absorption and metabolism probably contribute
to the confounding factors affecting epidemiology but have not been clearly associated with
CRC development.
The modifiable risk factors physical activity, obesity (increased body mass index and waist
circumference), diet (red and processed red meat, fibre), smoking and alcohol are the five
main modifiable factors associated with CRC incidence. Their individual relative risks range
− 2−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
between 1.20 and 1.30. Although factors are interrelated, their individual contributions are
assumed to be additive.
Key references: Corpet, 2011; Huxley et al, 2009; Kirkegaard et al, 2010.
4.
Possible impact on prevention in Belgium
The lowering of average red and processed red meat consumption in Belgium from 95 to 50
g/d might save about 1200 cases of CRC (~ 15 % of total) through primary prevention. Such
effect
is
in
line
with
the
European
action
against
colon
cancer
(http://www.stopcoloncancer.info/) and can be considered as complementary to preventive
screening programs planned e.g. in Flanders and Wallonia.
Key references: Atkin, 1999; De Vriese et al, 2006; Pacolet et al, 2011.
5.
The importance of meat in nutrition
In Belgium, the actual and recommended daily consumption of the food group
meats/fish/eggs/legumes/meat substitutes is 161 g and < 100 g respectively according to
the information of the food consumption survey (2004) and of the dietary recommendations
of the Superior Health Council of 2009. Estimates of actual consumption of red meat and
processed red meats within this group amount to 61 and 32 g/d respectively and at the
national government level the recommended consumption of the food group
“meats/fish/eggs/legumes/substitutes” is 75-100 g/d (in “Nationaal voedingsplan voor een
betere gezondheid“ - “Plan National Nutrition pour une meilleure santé” at
http://www.belgium.be/nl/gezondheid/gezond_leven/voeding/nationaal_plan/ or
http://www.belgium.be/fr/sante/vie_saine/alimentation/plan_national/).
Red and processed red meats, are main sources of high quality protein, the minerals iron
and zinc and the vitamins B12 and D. More specifically, moderate amounts of red meat (~
100 g/d) were recently shown to be valuable sources for protein synthesis in the elderly.
Based on both health and environmental arguments it can however be expected that
lowered amounts of red meat and processed red meats will be advocated in the food group
concerned. It is shown that considerable lowering or even excluding meat intake should not
harm nutritional adequacy in industrial countries. Specifically it is now clear that iron intakes
below the WHO recommended intakes also prevalent in Belgian women, far exceed the
levels that induce anemia. Strong evidence suggests that recommended intakes should be
reviewed taking into account the tightly regulated iron absorption mechanisms varying with
the iron content of the food and the regulation of relevant gene expression mediated by
inflammation associated cytokine activity. As there is now an explicitly recognized
equivalence between iron from meat and non-meat sources and since meat and meat
products account for ~ 20 % of total iron intake, a considerable lower intake of meat and
meat products is not expected to result in “iron deficiency”. Similar arguments relate to Zn,
vitamin B12 and vitamin D where homeostatic control of absorption and/or supply by other
animal foods or enriched foods allow for a lowering of meat intake. A similar argument can
be made in relation to protein quality shown to be adequate for both high and low animal
sourced foods in Western diets. An additional argument can be made for the lowering of
processed red meat intake, a food group second in line in accounting for about 18 % of
sodium intake, an issue clearly subject to considerable lowering.
Key references: De Vriese et al, 2006; Vandevijvere et al, 2009; Millward & Garnet, 2010; Geissler &
Singh, 2011;Van Winckel et al, 2011.
− 3−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
6.
Carcinogenic mechanisms
Apart from those induced by inherited genetic mutations, the majority of CRC cases are
sporadic and thus caused by environmental factors mainly involving diet. CRC arises as a
benign adenomatous polyp that is finally transformed into an invasive cancer associated
with genomic instability. Today, three distinct molecular pathways of genomic instability in
CRC have been recognized: the chromosomal instability pathway, the microsatellite
instability pathway and the CpG island methylator phenotype pathway. Like for other types
of cancer, inflammation has been suggested to be involved in the development of CRC.
Within this context, inflammatory bowel disease (including both ulcerative colitis and Crohn’s
colitis) has been identified as an important risk factor for developing CRC. Also in the other
sporadic CRC cases, chronic inflammation is likely to be involved. Furthermore, the
intestinal microflora and the activity of Toll-like receptors on intestinal epithelial cells have
been associated with the development of CRC. In order to explain the link between the
intake of red and processed red meat and the increased risk of CRC, several hypotheses
have been proposed.
Polycyclic aromatic hydrocarbons (PAH) and heterocyclic amines (HCA) have both been
related to CRC incidence in epidemiology. Meat and processed red meats significantly
contribute to their intake. PAH and HCA may be present as contaminants in the fresh meat
and/or formed during cooking by contact with open flames (PAH) or by high temperature
treatments to the “well done” state (HCA). Both groups of compounds are however not
specific for red meat and processed red meats. They are indeed also present in fish and
poultry products, foods not found to increase or even lower (fish) the risk for CRC.
Nevertheless recommendations for meat cooking in order to minimize production of PAH
and HCA should be considered, for household cooking as well as for cooking in restaurants
and in catering.
At present, N-nitroso compounds (NOCs) and/or lipid oxidation products (LOPs) are
considered to be the compounds most probably responsible for the increased risk for CRC.
NOCs are DNA alkylating agents that may be present in meat products, especially in
processed red meat, but can also be formed endogenously. Intervention studies in human
volunteers and experimental animals both showed an increase in the intestinal production of
NOCs, measured as apparent total NOCs. However, until now, the carcinogenicity of the
ATNC (apparent total N-nitroso compounds) formed in the gut remains unknown. LOPs on
the other hand are formed during lipid peroxidation of polyunsaturated fatty acids. The
formation of LOPs and NOCs including nitrosamines has been shown to occur during nitrite
(and/or nitrate) curing of red meat and subsequent digestion. Compounds of these groups,
yet to be precisely identified, ingested with processed red meats may consequently be the
culprits of the clearly more important cancer promoting effects of processed red meats. The
presence and formation of these compounds in processed red (nitrite cured) meats
deserves extensive additional research in relation to the justification of nitrite use in meat
processing.
Evidence from both epidemiologic and experimental studies suggests that heme plays a
crucial role in the link between the risk of CRC and red and processed red meat intake. A
different promoting effect of heme and nitrosyl heme on the production of NOCs and LOPS
during both processing {nitrite (and/or nitrate) curing followed or not by cooking} and
digestion may be involved. However, the observation that pig and poultry, two meat products
with similar heme contents have different CRC promoting activities suggests that the
presence of (nitrosyl)heme alone cannot explain the increased risk for CRC. The production
of circulating anti-N-glycolylneuraminic acid antibodies in response to red and processed red
meat ingestion, leading to local chronic inflammation and a propensity to develop dietrelated carcinomas seems to offer a more plausible explanation. Indeed, this mammalian
− 4−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
cell surface sialic acid is not produced by bacteria or plants, is low or absent in poultry and
fish, but abundant in red meats (mainly beef, pork, sheep but also meats from other species)
and metabolically accumulated by humans, all genetically deficient in its production.
Considering all the different hazardous compounds present in red and processed red meat,
the increased risk for CRC may not be associated with one unique causative agent, but with
the presence of different compounds, acting on multiple stages of CRC.
Key references: Hedlund et al, 2008; Hogg, 2007; IJssennagger et al, 2012; Joosen et al, 2009; Loh et al,
011; Lombardi-Boccia et al, 2002; Mirvish et al, 2008; Rohrmann et al, 2009; Sinha et al, 2005; Terzic et
al, 2010; Westbrook et al, 2010.
7.
Possibilities for mitigation
Epidemiology indicates that dietary changes may alleviate the carcinogenic effects of red
meat and processed red meats and involve a “healthy eating pattern” characterized by
increased dietary fiber and fish, confirming the WCRF/AICR and EPIC findings. Very clear
evidence pointing to a protective effect of dairy products (yogurt) and calcium supplements
and, to a somewhat less extent, of vegetables and fruits is also available.
Experimental work with volunteers has shown that replacement of red meat with fatty fish
reduces the formation of mutagenic compounds whereas addition of cruciferous vegetables
(cauliflower, cabbage, broccoli, …), yogurt and chlorophyllin tablets to fried meat diets and
of calcium supplements or α-tocopherol to cured meat diets reduce indicators of
mutagenesis and DNA damage. Existing knowledge on the alleviating effect of resistant
starch through promotion of a butyrate type fermentation in the large intestine has been
confirmed in rats fed with red meat.
Optimization of processing technology has shown the lowering of HCA production by
addition of spices to meat cooking. The addition of α-tocopherol to meat curing solutions and
packaging of processed red meats to prevent oxidation has lowered CRC biomarkers in
volunteers. Methods are described that may potentially alleviate the CRC promoting activity
of processed red meats by the use of lower nitrite levels or nitrite alternatives. Some
evidence suggests that the introduction of “functional components” such as (long chain)
omega-3 polyunsaturated fatty acids and plant antioxidants in processed red meats through
processing and/or animal feeding may also mitigate the CRC promoting activity. Special
attention should be given to the possibility of promoting the formation of Zn-protoporphyrin,
a compound present in Mediterranean raw cured ham, known to inhibit hemin-induced DNA
damage and formed involving an iron-removal reaction inhibited by nitrite.
Key references: Pala et al, 2011; Corpet, 2011; Shaughnessy et al, 2011; Demeyer et al, 2008.
8.
The types of processed red meats involved
No systematic epidemiological studies have compared different processed red meats (mainly all
kinds of nitrite cured meats) in relation to CRC incidence. The larger incidence of CRC in
Northern Europe compared to Mediterranean countries was associated with an almost double
intake of processed red meats and a much larger proportion of cooked and cured sausages and
“minced” hamburger type products, known to be high in fat content. This finding is in line with the
established relation of lipid oxidation to the promotion of CRC by processed red meats and with
the presence of Zn-protoporphyrin in many Mediterranean raw cured ham types.
Key reference: Demeyer & De Smet (2011).
− 5−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
9.
Conclusions
For the benefit of the Spanish Governments, Bejar et al (2010) stated that “a minimal time span
of ten-fifteen years is necessary for changes in exposure to risk factors” to be able to modify the
incidence of CRC. This report confirms their conclusion that implementation of “legislative and
educational measures in the field of Health Promotion regarding the diet can therefore be
considered urgent”. Such measures should inform the consumer how to make healthy food
choices based on scientific evidence in a clear and straightforward manner not drawn in the
actual confusing information cloud (Perez-Cuero & Verbeke, 2012). Discussing guidelines for a
healthy diet from an ecological perspective, the Dutch Health Council (Health Council of the
Netherlands, 2011) concluded that “the average consumption of red meat at the population level
and the combined intake of red and processed red meat exceeded the norms set by the World
Cancer Research Fund and the British Scientific Advisory Committee on Nutrition”. Based on
one reference only (not covered by the ISI Web of Science nor by PubMed) it considers that “the
significance of this fact for questions of health is uncertain”. Nevertheless, its recommendations
for other reasons involve only “occasional consumption” of “mince, rolled beef and sausage”
(meat) and of “raw ham, smoked meat, frankfurter, shoulder of ham, sausage, bacon, pâté and
pork fricandeau” (meat products). Evaluating the “New Nordic diet”, Adamsson et al (2012) refer
to “a primarily plant-based diet ... associated with decreased morbidity and mortality”. In analogy
with more evidence based and explicit French (Programme National Nutrition Santé, France,
2009) and UK (Scientific Advisory Committee on Nutrition, UK, 2010) guidelines this report
justifies a proposal to amend the existing recommendation at the federal Government level
(“Nationaal voedingsplan voor een betere gezondheid - “Plan National Nutrition pour une
meilleure santé” at http://www.belgium.be/nl/gezondheid/gezond_leven/voeding/nationaal_plan/
or http://www.belgium.be/fr/sante/vie_saine/alimentation/plan_national/).
The epidemiological evidence is less clear when higher upper levels of intake (up to about 200
g/d) are absent and is not apparent with populations of older and health conscious individuals
(see under 2.2.2.4). Also, it has been shown that moderate amounts of red meat (~ 100 g/d for
adults ) remain valuable sources for net protein synthesis for the elderly (see under 2.2.5.2). It is
therefore proposed to maintain the actual recommended maximal intake of 100 g/d of the food
group meats/fish/eggs/legumes/meat substitutes and the adapted proposal reads : “It is
recommended to consume not more than 100 g per day (amount before preparation) of the food
group meats/fish/eggs/legumes/meat substitutes. A high consumption of red meat (mainly beef,
pork, sheep, horse, goat, …), mixed meats (with added fat and salt) and even more, of
processed red meats (mainly cured using nitrite) slightly increases the risk of colorectal cancer.
Therefore, choose preferably poultry, limit red and mixed meats and avoid processed red meats,
in particular fatty meat products of the cooked sausage type, paté and salami. When preparing
red meat (baking, roasting and cooking) make full use of vegetable spices, do not overheat the
meat to a dark brown colour but, when present, remove such parts on the plate before
consumption. Eating fish, including fat fish, once or twice a week is recommended as well as the
occasional use of vegetable meat alternatives.”
It should be remembered that “red meat” and “mixed meats” refer to fresh red meats that have
not been subjected to other treatments than cooling, freezing and or comminution for mixing with
other red meats and salt (e.g. ground meat and hamburger type products). Processed red meat
is defined as ”red meats preserved by salting (mainly with addition of nitrite and/or nitrate) and
one or more other treatments”. In quantitative terms and in accordance with the WCRF/AICR
(2007) this means that at the level of the individual who eats red meat, the recommendation is
not to exceed the consumption of 500 g/week, very little if any of which to be processed. This
should be in accordance with a public health goal for a population average consumption of less
than 300 g/week of red meat, very little if any of which to be processed; a goal aimed at effects
complementary to the screening effort planned in Flanders. In addition and in comparison to the
messages related to the abstention of smoking and excessive alcohol use, an
− 6−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
alternative/additional and more straightforward and simple message for the consumer as
inspired by Perez-Cuero & Verbeke (2012) might be:
“The best prevention of colorectal cancer is the combination of higher physical activity
with a fiber-rich diet, limiting red meat and minimizing processed red meat products.”
10. Recommendations for research
Short of inconceivable randomized controlled clinical trials with colo-rectal cancer incidence as
outcome, the colorectal carcinogenic effect of red meat and processed red meats has been
demonstrated beyond doubt, both in epidemiology as well as in experimental work with both
animals and humans. It seems clear that the major carcinogen involved is heme although
considerable evidence points to the negative effect of heterocyclic amines formed by overheating red meat and apparent from an extreme brown/charred appearance. It is not clear
however why the carcinogenic effect of fresh red meats is only about half that of processed
(cured) meats. In Belgium, cured meats are almost exclusively derived from pig meat and both
the higher fat and salt content compared to fresh meat may be involved. Further research on the
issue is clearly required.
Also, in view of the newer insights:
contrasting health effects of individual foods vs. those of a dietary pattern both in
intervention trials with animals or, preferably, humans using CRC markers and using in vitro
digestive systems;
the possibilities for animal production, meat processing and domestic food preparation to
incorporate cancer mitigating components and /or processes
(applied) research in these areas should be promoted.
Work should preferably involve:
the development of « functional meat products » incorporating components mitigating
carcinogenesis through animal (pig) feeding (e.g. plant derived antioxidants) and/or meat
processing (e.g. Calcium salts, fibrous components, minor plant components, etc.);
experiments testing such diets/products fed to animals (e.g. rodents, pigs) or to in vitro
digestive systems evaluating colon epithelial changes and/or oxidative status of digestive
contents;
intervention experiments with humans involving testing of processed red meats,
analogous to e.g. the recent work described in Windey et al (2012a).
Also in Belgium, research along these lines has recently been initiated by the Federal Public
Service (FPS) Health, Food Chain Safety and Environment: RF 11/6250 MEATNOX “Vorming en
(geno)toxische activiteit van nitros(yl)atie- en oxidatieproducten in het gastrointestinaal stelsel:
rol van nitrietgepekelde vleesproducten en preventie.”
− 7−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
Keywords
Keywords
meat
Processed
red
meats
colorectal cancer
nitrite
processing
curing
cooking
prevention
Mesh terms*
meat
meat products
Sleutelwoorden
vlees
vleeswaren
Mots clés
viandes
charcuterie
colorectal
neoplasms
nitrites
food handling
darmkanker
cancer intestinal
Stichwörter
fleisch
verarbeitete
fleischprodukte
darmkrebs
nitriet
verwerking
pekelen
koken
preventie
nitrite
transformation
saumurage
chauffer
prévention
nitrit
verarbeitung
pökeln
kochen
vorbeugung
health promotion
* MeSH (Medical Subject Headings) is the NLM controlled vocabulary thesaurus used for indexing articles
for PubMed.
− 8−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
CONTENTS
SUMMARY ................................................................................................................................................. 1
1
INTRODUCTION AND ISSUES ........................................................................................................... 11
2
FURTHER DETAILS AND ARGUMENTATION ..................................................................................... 13
2.1
METHODS......................................................................................................................................... 13
2.2
ARGUMENTATION .............................................................................................................................. 13
2.2.1 Introduction............................................................................................................................... 13
2.2.1.1
2.2.2.1
2.2.2.2
2.2.2.3
2.2.2.4
Colorectal Cancer ............................................................................................................................ 13
Earlier evidence............................................................................................................................... 15
More recent evidence ..................................................................................................................... 15
Lack of evidence and criticisms ....................................................................................................... 18
Recognition ..................................................................................................................................... 23
2.2.3 Importance of the risk associated with (processed) meat intake within the context of other risk
factors .................................................................................................................................................. 23
2.2.3.1
2.2.3.2
2.2.4
2.2.5
Possible impact on prevention in Belgium ................................................................................ 26
The importance of meat in nutrition ......................................................................................... 27
2.2.5.1
2.2.5.2
2.2.5.3
2.2.6
Consumption and recommendations.............................................................................................. 27
Sustainable meat consumption meeting dietary requirements for health ..................................... 29
Meat in essential nutrient supply ................................................................................................... 30
Carcinogenic mechanisms ......................................................................................................... 35
2.2.6.1
2.2.6.2
2.2.6.3
2.2.6.4
2.2.6.5
2.2.6.6
2.2.6.7
2.2.7
2.2.8
Genetics .......................................................................................................................................... 23
Other modifiable risk factors .......................................................................................................... 25
Unlikely hypotheses: fat, protein and thermoresistant oncogenic bovine viruses ......................... 37
Polycyclic aromatic hydrocarbons and heterocyclic amines ........................................................... 38
Nitrosamines and other N-Nitroso compounds .............................................................................. 44
Heme ............................................................................................................................................... 48
The “white meat” controversy. ....................................................................................................... 55
Effect of processing on the carcinogenic effect of red meat........................................................... 56
Summary ......................................................................................................................................... 62
Possibilities for mitigation ......................................................................................................... 64
The types of processed red meats involved ............................................................................... 67
3
CONCLUSIONS AND RECOMMENDATIONS ...................................................................................... 70
4
REFERENCES .................................................................................................................................... 72
5
RECOMMENDATIONS FOR FURTHER RESEARCH .............................................................................. 96
6
COMPOSITION OF THE WORKING GROUP ....................................................................................... 97
ABOUT THE SUPERIOR HEALTH COUNCIL (SHC) ....................................................................................... 98
− 9−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
ABBREVIATIONS AND SYMBOLS
4-HNE (4-hydroxynonenal)
ACF (aberrant crypt foci)
AICR (American Institute for Cancer Research)
ATNC (apparent total N-nitroso compounds)
BaP (benzo[a]pyrene)
BMI (body mass index)
CAC (colitis-associated cancer)
CI (confidence interval)
CRC (colorectal cancer)
CVD (cardiovascular diseases)
DAFNE (Dose Adjustment For Normal Eating)
DHN-MA (1,4-dihydroxynonane mercapturic acid)
DME (drug metabolizing enzymes)
EPIC (The European Prospective Investigation into Cancer and Nutrition)
EU (European Union)
FAO (Food and Agricultural Organization)
FFQ (food frequency questionnaire)
HCA (heterocyclic amines)
IBD (inflammatory bowel disease)
iNOS (inducible nitric oxide synthases)
IQ ( 2-Amino-3-methylimidazo[4,5-f]quinoline)
MDA (malondialdehyde)
MDF (mucin-depleted foci)
MeIQ (2-Amino-3,4-dimethylimidazo[4,5-f]quinoline)
MeIQx (2-Amino-3,8-dimethylimidazo[4,5-f]quinoxaline)
mi-RNAs (micro RNAs)
MP (myeloperoxidase)
NAT (N-acetyltransferases)
NDEA (N-nitrosodiethylamine) NDBA (N-nitrosodibutylamine)
NDMA (N-nitrosodimethylamine)
Neu5Gc (N-glycolylneuraminic acid)
NOCs (N-nitroso compounds)
NPIP (N- nitrosopiperidine )
NPYR (N-nitrosopyrrolidine)
PAH (polycyclic aromatic hydrocarbons)
PhIP (2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine)
PPAR-alpha (peroxisome proliferative activated receptor, alpha)
RSNOs (S-nitrosothiols)
SNP (single-nucleotide polymorphism)
SULT (sulfotransferases)
TBARS (Thiobarbituric acid reactive substances)
WCRF (World Cancer Research Fund)
WHO (World Health Organization)
− 10−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.css -hgr.be
1
INTRODUCTION AND ISSUES
The nutritional value of meat and processed red meats has been overshadowed for some time
now in the eye of consumers by various media reports that also point to the increased risk of
cancer associated with consuming these foodstuffs. Some of these reports have been issued by
renowned experts, others are pure fantasy but often refer to international reports that indicate that
there is a link between eating meat and processed red meats and the risk of bowel cancer, such
as e.g. the reports of the “European Prospective Investigation into Cancer and Nutrition (EPIC)”
(http://epic.iarc.fr/keyfindings.php) project and the “World Cancer Research Fund/American
Institute for Cancer Research” (WCRF) (www.dietandcancerreport.org/?p=ER). Popular reports
and recommendations often ignore the complexity of other environmental and genetic factors that
determine the risk of cancer. Moreover, insufficient attention is paid to the diverse natures,
amounts and means of preparing not only meat and processed red meats, but also other
foodstuffs. This concerns e.g. nutrients that have a protective effect (antioxidants, vitamins,
micronutrients) or other substances that are potentially harmful as a result of the manner in which
they are prepared (presence of certain additives, substances that are released when grilled,
salted foodstuffs, fried food, ...) and/or contaminated with carcinogenic substances
(environmental pollution, pesticide residues, ...). It therefore seemed useful that the SHC should
assess the scientifically based recommendations that have been made on this issue and
formulate them in such a way as to make them understandable to the general public and easy to
implement on a daily basis. Given the complexity of foodstuffs and the numerous factors that play
a part in the appearance of cancer, the decision was made to start with a case study:
“Assessment of the risk of developing bowel (colorectal) cancer attributed to eating meat and
processed red meats". Although the literature is not always clear, the term “red meat” in this
report refers to fresh red meat products (such as beef, pork, sheep or lamb but also other meats
except poultry meat) that have not been subjected to other treatments than cooling, freezing and
or comminution for mixing with other red meats and salt (e.g. ground meat). Processed red meat
defined as “meat preserved by smoking, curing or salting or by addition of chemical
preservatives” in the “World Cancer Research Fund / American Institute for Cancer Research“
(WCRF/AICR) is here more simply specified as ”red meats preserved by salting (mainly with
addition of nitrite and/or nitrate) and one or more other treatments ”.
In order to do so, the following approaches have been suggested:
1)
Assess the updated results of the WCRF and EPIC regarding the risk of developing bowel
cancer from eating meat and processed red meats, with attention paid to the following
issues:
are the results convincing enough for this risk to be acknowledged?
assess and situate the risk from eating meat and processed red meats as opposed to
their nutritional value and the other risk factors;
assess the different carcinogenic mechanisms that have been suggested;
assess the possible means of reducing the risk both when preparing and processing
meat as well as the amount and place of meat and processed red meats in a full meal.
The information from the WCRF and EPIC was updated on the basis of the Web of
Science.
2)
In addition, specific attention was devoted to the following:
compare the risks posed by the different types of fresh meat (red meat, i.e. mainly beef,
pork, sheep, horse, goat, … and white meat, i.e. poultry) with those posed by
processed red meats;
compare the risks posed by the various types of processed red meat depending on the
methods used to produce them (curing, fermenting, drying and smoking of (minced)
meat that is mixed with fat and may subsequently undergo heating);
− 11−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
the effects of the means of preparing fresh meat (frying, broiling, barbecuing,
hamburgers,...);
the effects of the simultaneous intake of other foodstuffs [that are rich in antioxidants
(vegetables, red wine, spices, dairy products,...) and calcium (dairy products)].
3)
Finally, an attempt was made to propose adjustments to the current guidelines for healthy
diets, especially as regards meat and processed red meats, with the focus on the
specification of meat products, processed red meats, etc.
4)
The manner in which the project will affect public health:
It has been estimated that around 30% of all cases of cancer have a dietary cause. The
nature and composition of the diet are believed to play a more important role than the effect
of it being contaminated by residues or harmful organisms. Cancer, which affects a great
number of people, is looked upon as one of the most serious diseases, next to
cardiovascular conditions and diabetes. There is no doubt that maintaining a healthy and
balanced diet plays an important part in preventing disease. Over the past few decades, the
scientific knowledge on cancer has increased significantly. This knowledge can certainly be
used to formulate reliable dietary recommendations that should ultimately lead to a
considerable drop in certain types of cancer. An example would be a reduction in the
incidence of colorectal cancer by some 10 to 20% as a result of recommendations
regarding the nature, the means of preparing the meat and the amounts consumed. It is
therefore clear that recommendations can be proposed that maintain the intake of meat
within an optimally balanced diet, as is also the case for e.g. the fat intake.
In order to provide an answer to the question, an ad hoc working group was set up which
included experts from the following fields: meat technology, nutrition, toxicology, pathology,
oncology, biochemistry, analytical chemistry, food technology, food composition, epidemiology
and statistics.
− 12−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2
FURTHER DETAILS AND ARGUMENTATION
2.1 Methods
The document is an advice of the Superior Health Council of Belgium. For collection, evaluation
and interpretation of information, official statistical data and health recommendations issued by
international and national governments or industrial organizations were used. Other information
was limited to scientific papers published in peer reviewed journals as traced in the major
databases Web of Science and, to a less extent, PubMed and electronically available on line or
as reprint. Quality of published research was evaluated based on a combination of journal impact
factors, frequency of citation and authority (experience/credibility) of institutes and authors. The
report uses a holistic review approach covering a diversity of expertise ranging from epidemiology
top/down to meat technology and including statistics, nutrition, toxicology, pathology, oncology,
biochemistry, analytical chemistry, food technology, food composition and nutrition.
2.2 Argumentation
2.2.1 Introduction
It has been recognized for years that “healthy food” makes an important contribution to the
prevention of chronic non-communicable disease. Based mainly on epidemiological evidence, it is
generally accepted that a diet high in saturated fat and energy-dense foods (those with high fat
and/or sugar content), and low in fruit and vegetables - along with a sedentary lifestyle and
smoking - is the major cause of cardiovascular diseases (CVD) and of certain types of cancer,
the top two causes of death in developed countries (WHO, 2003). Accordingly, it has been stated
that much greater health gains could be made through promoting a healthy diet than through
improving the high level of food safety, guaranteed by efficient and legally compelled control
(Wadge, 2004)(van Leeuwen, 2006). Estimates suggest that better diets could prevent around
30-40% of cancer cases and that poor nutrition accounts for 4.6% of all disability-adjusted lifeyears lost in the EU, with obesity and physical inactivity accounting for an additional 3.7% and
1.4%, respectively (Pomerleau et al, 2003). These findings have been translated into simple foodbased rather than nutrient based recommendations on healthy eating aimed at the general public
to
provide
a
basic
framework
for
planning
meals
or
daily
menus
(http://www.eufic.org/article/en/expid/food-based-dietary-guidelines-in-europe/) (De Henauw & De
Backer, 1999). It should be emphasized that these recommendations, that may be considered
complementary to efforts of screening for the diseases referred to, are almost exclusively based
on epidemiology, showing biologically plausible associations between food intake and chronic
disease, consistently found in both prospective observational and case-control studies. Such
studies are selected using criteria for adequate collection and treatment of data involving e.g.
length of observation period, numbers of participants and adjustment for confounding factors as
well as for the presence of dose-response relations (WHO, 2003)(Navia et al, 2010).
2.2.1.1 Colorectal Cancer
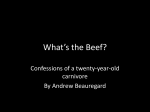
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in the world (1.23 million
or 9.7% of all cancers diagnosed in 2008) with a higher incidence in the developed world (Ferlay
et al, 2010). It is remarkable that country differences in incidence rates are much larger than
differences in mortality rates (Fig.1). In Europe, CRC is the second leading cause of cancer
deaths and in Belgium 3609 and 4378 colorectal invasive tumours were reported in 2010 for
females and males respectively, equivalent to 11,8 and 12,3 % respectively of all newly
diagnosed malignant tumours (European Commission, 2010). Age-standardised 2008 incidence
rates per 100 000 in Belgium are relatively high when compared to other European data : 42,3 for
females and 66,3 for males vs. respective minimum values of 17,1 and 24,7 and maximum
values of 52,6 and 93,8 (European Commission, 2010). More than 95% of CRCs arise in
− 13−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
individuals without a significant hereditary risk and are related to environmental risks as clearly
reflected by the changes in incidence after migration that occur rather rapidly, even among the
first generation of migrants (Parkin, 2004)(Watson & Collins 2011)(Lund et al, 2011). It is also
generally recognized that the strongest contribution to environmental risk for CRC is diet; its
contribution has been estimated as 70 % of incidence (Anand et al, 2008). It has also been
observed that within developing countries, increasing levels of urbanization and increased
consumption of meat, dairy products and processed foods have coincided with a dramatic
increase in incidence of CRC (Parkin, 2004).
Fig. 1. Estimated age-standardized incidence and mortality rates (number per 100.000) of colorectal
cancer in 2008 (Ferlay et al, 2010)
− 14−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.2 Research evidence linking red and processed red meat consumption to an
increased risk of colorectal cancer (CRC)
2.2.2.1 Earlier evidence
It is noteworthy that a significant link was observed between high meat consumption and CRC
mortality in the earlier household budget studies of the EU DAFNE projects, also involving
Belgian data (Lagiou et al, 1999). At a later date specific recommendations for the prevention of
cancer included moderation in the consumption of preserved meat, such as sausages, salami,
bacon and ham (meaning cured, smoked and nitrite treated meat products) (WHO, 2003). Using
the same research methodology, 5 CRC risk factors were deemed "convincing" by the World
Cancer Research Fund (obesity, physical inactivity, intake of red meat, processed meat, alcohol)
and the recommendations were strengthened into ‘‘limit consumption of red meats (such as beef,
pork, sheep, horse, goat, …) and avoid processed meat” (WCRF/AICR, 2007). The latter more
severe recommendation defined “processed meats” as “meats preserved by smoking, curing or
salting or by the addition of chemical preservatives” and was based on an extensive metaanalysis of cohort and case-control studies including e.g. work from “The European Prospective
Investigation into Cancer and Nutrition (EPIC)” grouping 23 research institutes and following
about 500,000 people in 10 EU member states since 1992 (Norat et al, 2002). The studies
supporting the recommendation were criticized because of the lack of precision in defining
processed meats and in the assessment of food intake by the questionnaires used as well as in
accounting for the large variability in the nature of meat and meat products and the possible
remaining confounding of the results. Nevertheless, after reviewing the available information,
including the replies to criticism, it was concluded that the link between red and processed meat
consumption and the incidence of colo-rectal cancer should be recognized and that it is
warranted to take action (Demeyer et al, 2008). Reports and recommendations refer to processed
meats but do clearly (although tacitly) not cover poultry. To prevent possible confusion with
definitions of meat covering poultry (as in Belgium) the term “processed meats” is replaced by
“processed red meats” further in this report.
2.2.2.2 More recent evidence
A search of the Web of Science since June 2008 produced the published results of 6 new large
prospective cohort studies convincingly linking red and/or processed red meat consumption to the
incidence of CRC. The sites and types of tumors investigated and the nature as well as the
measure of meat consumption varied between reports but studies involving a total of 1,707,840
individuals followed for at least 5 and up to 9 years clearly indicated that the incidence of
colorectal adenoma or cancer increases with the frequency and/or amounts of meat or diets high
in meat consumed in Korea (Shin et al, 2011) and in the US (Reedy et al, 2010; Fung et al, 2010;
Cross et al, 2010; Ferrucci et al, 2012), including intakes a decade before diagnosis (Ruder et al,
2011). Although less reliable, large scale case-control studies in the US (Fu et al, 2011), Canada
(Squires et al, 2010; Hu et al, 2008; also reported in Hu et al, 2011) and Uruguay (De Stefani et
al, 2009) involving a total of 33,140 cases and 15,179 controls yielded the same conclusion with
special emphasis on the increased risk associated with cooking temperature (Cotterchio et al,
2008; Fu et al, 2011) and with intake of processed (salted, pickled) meats. The latter was also
found to be related to an increased risk of several other cancers (Hu et al, 2011; Squires et al,
2010; De Stefani et al, 2009) in line with the findings of two large cohort studies involving 37 698
men and 83 644 women followed for more than 20 years involving dietary assessment updated
every 4 years (Pan et al, 2012). After multivariate adjustment for other major lifestyle and dietary
risk factors, the pooled hazard ratio risk for total cancer mortality (HR) (95% CI) for a 1-serving
per-day increase was 1.13 (1.07-1.20) for unprocessed red meat and 1.20 (1.15-1.24) for
processed red meat. Apart from these epidemiological observations, reviews of the literature
point to modest relative risk estimates ranging from 1.0 to 1.3 for highest vs lowest consumption
− 15−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
categories of meat or per 100 g of meat/day (Baghurst, 2007), from 1.02 to 1.35 for diets high in
meat and meat products (Randi et al, 2010) and from 1.09-1.71 for high vs low frequency of meat
consumption (Smolinska & Katarzyna, 2010) as well as suggesting a 20-50 % higher risk
associated with the highest levels of processed red meat consumption compared to non meat
eaters (Santarelli et al, 2008). A recent meta-analysis of eight cohort and eight case-control
studies addressing the association between dietary patterns and CRC concluded : “the risk of
colon cancer was increased with patterns characterized by high intake of red and processed red
meat and decreased with those labeled as ‘healthy’ ” (Magalhaes et al, 2011). This finding is in
line with a very convincing and recent meta-analysis focusing on ten prospective studies and
involving linear dose-response analyses concluding “High intake of red and processed red meat
is associated with significant increased risk of colorectal, colon and rectal cancers. The overall
evidence of prospective studies supports limiting red and processed red meat consumption as
one of the dietary recommendations for the prevention of CRC” (Chan et al, 2011). This paper
emanates from the continuous update project report on CRC (WCRF/AICR, 2011) on the
evidence relating food, nutrition and physical activity to the prevention of CRC updated in 2010.
The review added 263 papers and updated meta-analyses for whole grains, fruits and
vegetables, meat and fish, dairy foods, alcohol, dietary fiber, glycaemic index, folate, vitamin D,
heme iron, calcium, physical activity, body mass index, abdominal fatness and adult attained
height; apart from alcoholic drinks, the only foods confirmed to be associated with a “convincing”
increased risk of CRC were red meat and processed red meat. The evidence for a protective
effect of foods containing dietary fiber had strengthened and was upgraded from probable to
convincing. The search, study selection, and data extraction was conducted by several reviewers
and the work followed the earlier established stringent protocol and search strategy for selection
and evaluation of studies (WCRF/AICR, 2007a; WCRF/AICR, 2012) covering:
The independence of the systematic literature review centers and the evaluation by a 21
member expert panel was assured by the separation of the collection of evidence from
assessing and judging it.
The use of stringent criteria for categorizing associations as convincing or probable (Table 1)
Testing for heterogeneity due to
Gender, geographic area, unit of meat intake used in the report (grams or
times/servings), year of publication and length of follow-up.
-
Variable adjustment for co-variates involving age and total energy intake and in many
cases BMI, smoking, physical activity, alcohol and other potential confounders. It was
found that adjustment for larger number of co-variates was more likely to yield weaker
relative risks than adjustment for smaller numbers of co-variates. Several potential
confounders were not included in the final statistical models in some studies because, as
the authors reported, their inclusion in the model did not substantially modify the relative
risk estimates.
Table 1. Criteria used to characterize associations between life-style variables and cancer
(WCRF/AICR, 2007a) (WCRF AICR, 2012)
− 16−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Recognizing the variability in the definition of red and processed red meats between the
studies. In general, the meat item was a combination of red meat, such as beef, pork, sheep,
horse, goat, … and processed red meat was generally described as processed red meat,
preserved meat or cured meat, but individual items included in the meat group could vary
between the studies including e.g. hotdogs, luncheon meat and bacon.
Limiting the evidence for exposures graded as convincing, probable or suggestive in the 2nd
Expert Report, to results of cohort studies only. These are considered more reliable than
case-control studies, obviously more prone to selection and recall bias, difficulties in
remembering past behavior and changes in that behavior with time and also because of the
high number of cohort studies existing. Thirteen cohort studies on cancer incidence were
published on red and processed red meat intake and CRC risk up to May 2010. All 13 studies
were used in dose-response meta-analyses of red and processed red meat intake and the
risk of colon, rectal and colorectal cancer.
Reports on meta-analysis (e.g. a weighted analysis of several research results) and pooled
analysis (similar to meta-analysis, but pooled data from multiple studies are analyzed as a
single dataset) were identified in the search, were not included in the database but were used
for support in the preparation of the report. No studies focusing on pre-malignant colorectal
conditions (for example colorectal adenomas) were retained and results on incidence and
mortality are presented separately. The search, study selection, and data extraction was
conducted by several reviewers.
The reported summary relative risks were:
for each 100 g/day increase in red and processed red meat consumption, 1.16 (95% CI =
1.04-1.30, I2 = 47%, P heterogeneity = 0.06, nine studies) for CRC, 1.21 (95% CI = 1.061.39, I2 = 56%, P heterogeneity = 0.04, seven studies) for colon cancer and 1.31 (95% CI
= 1.13-1.52, I2 = 18%, P heterogeneity = 0.30, five studies) for rectal cancer.
for each 50 g/day increase in processed red meat consumption, 1.18 (95% CI = 1.101.28, I2 = 12%, P heterogeneity = 0.33, nine studies) for CRC, 1.24 (95% CI = 1.13-1.36,
I2 = 0%, P heterogeneity = 0.55, nine studies) for colon cancer and 1.12 (95% CI = 0.991.28, I2 = 0%, P heterogeneity = 0.56, eight studies) for rectal cancer.
for each 100 g/day increase in red meat consumption, 1.17 (95% CI = 1.05-1.31, I2 = 0%,
P heterogeneity = 0.48, eight studies) for CRC, 1.12 (95% CI = 0.97-1.29, I2 = 0%, P
heterogeneity = 0.89, nine studies) for colon cancer and 1.18 (95% CI = 0.98-1.42, I2 =
0%, P heterogeneity = 0.67, seven studies) for rectal cancer.
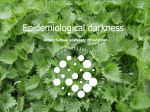
An important finding of the work as reported by Chan et al (2011), was the nearly linear relation
obtained from non-linear dose-response meta-analyses: CRC risk increased with red and
processed red meat intake up to approximately 140 g/day, where the curve approaches its
plateau (Fig. 2). The “key findings” of the EPIC project confirm these findings adding however that
the EPIC results strongly support that intake of fish decreases risk (European Prospective
Investigation into Cancer and Nutrition, 2012). Although the dangers of residual confounding in
interpreting small effects (hazard ratios between 0.6 and 1.6) calculated from observational
studies have recently been clearly presented (Sainani, 2012), publication of scientific and
convincing reports of similar and consistent effects continues. An association of red meat
consumption with colon and/or colo-rectal cancer (CRC) was confirmed in limited case-control
studies reporting that meat based diets were associated with an increased risk in both Uruguay
(De Stefani et al, 2012) and Argentina (Pou et al, 2012) whereas a plant based or “prudent” diet
respectively was protective. Danish work indicated that maternal intake of meats with dark
surface increases the bulky DNA adduct levels in both maternal and umbilical cord blood
(Pedersen et al, 2012). Increased serum C-peptide concentrations, indicative of an increased
− 17−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
CRC risk, were found to be associated with a higher meat dietary pattern in overweight female
participants in a large cohort US study (Fung et al, 2012). A meta-analysis showed that
vegetarians had a significantly lower cancer incidence than nonvegetarians (Huang et al, 2012).
In comparisons of statistical data on both food consumption and disease incidence or mortality,
Bejar et al (2012) found that increases in CRC incidence (1971-2002) paralleled increases in red
meat consumption in 8 EU countries. Zhang et al (2012) clearly related increases in colon and
other cancer mortalities over the past 40 years in several East-Asian countries to nutritional
transitions also involving increases in red meat consumption. They also noted that “these
changes in cancer mortality lagged similar to 10 years behind the inception of the nutrition
transition toward a westernized diet in selected countries or regions”. Recent work supports the
hypothesis that high consumption of red and processed red meat may also increase the risk of
colo-rectal adenoma, a benign tumor often leading to CRC (Xu et al, 2013; Aune et al, 2013) as
well as showing that a processed red meat dietary pattern prior to diagnosis is associated with
higher risk of tumour recurrence, metastasis and death among patients with CRC (Zhu et al,
2013). Rosato et al (2013) reported that high processed red meat intake increased the risk for
young-onset of CRC and even in patients with a genetically determined higher risk for developing
CRC a high meat dietary pattern was recently shown to increase colorectal adenoma incidence,
corroborating with the results for sporadic colorectal cancer (Botma et al, 2013). Van Meer et al.
(2013) recently concluded from a literature survey that meat intake also has a negative effect on
survival and mortality of CRC patients. All results clearly support the general recognition of the
problem as reflected e.g. in the statement of Lecerf (2011): “a link between high meat
consumption and cancer, particularly colorectal cancer, has been observed in nearly all
epidemiological studies”.
2.2.2.3 Lack of evidence and criticisms
The Web of Science search since June 2008 also produced a more limited number of papers
rejecting a link between red and/or processed red meat consumption and the incidence of CRC.
Observational studies.
-
A pooled analysis of food diet diary data obtained from the UK Dietary Cohort
Consortium did not find evidence of an association between red and/or processed red
meat consumption (disaggregated from composite foods) and CRC risk (Spencer et al.,
2010). Apart from the limited numbers of individuals studied (2,575), the authors
themselves stated that the null results might be due to the relatively low intake of both
red (~ 30 g/d) and processed (~ 15 g/d) meats estimated by diet disaggregation. More
surprisingly, a lower incidence of colo-rectal cancer was reported for meat eaters than
vegetarians in a large prospective study (61,566 individuals) characterized as
“descriptive” (Key et al, 2009), a finding possibly related to meat intakes below the
national average. Also, the standardized all-cause mortality rate in the population studied
was lower than that of the general UK population, reflecting that in surveys comparing
meat-eating controls with vegetarians, individuals are usually selected from similar
population groups with generally healthy lifestyles involving moderate average meat
intakes and relatively high intakes of fruit and vegetables (Millward & Garnett, 2010).
Furthermore, available evidence also suggests that self-defined vegetarians do consume
red meat and self-identification may indicate more than double the incidence of
vegetarianism than the operationalized definition (Vinnari et al, 2009).
− 18−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig. 2. Non-linear dose-response of red and processed red meats consumption and the risk of CRC
(from a meta-analysis by Chan et al, 2011).
-
In a multiethnic large scale cohort study involving 165,717 participants over 13.6 years,
Ollberding et al (2012) concluded that in basic models adjusting for age at cohort entry,
sex and race/ethnicity, there was an increased risk of CRC for participants in the highest
quintile for a dietary pattern consisting of high energy density-adjusted red meat and
energy density-adjusted total processed red meat when compared with those in the
lowest quintile. This effect disappeared however when multivariable models were used.
The contrast between this finding and “convincing” increasing risk of CRC of red and
processed red meat intake as discussed above can be explained by:
The old age range of individuals enrolled in the study (45 – 75 years), reflected in a
much higher CRC incidence rate of 151 per 100,000 as compared to 58 (in Norat et
al, 2005) and 33, the highest value reported for 2008 by Ferlay et al (2010).
The total red meat intake in the highest quintile (108.9 g/d) is in the lower range of
the mean values of the highest category of red and processed red meats intake in
the studies used by Chan et al (2011) (46 to 211 g/d ).
Construction of the food frequency questionnaire was complicated by the presence
of different food items traditionally consumed by the different populations
represented, including African Americans, Japanese Americans, Latinos, Native
Hawaiians and whites.
Different dietary patterns are associated with the different ethnicities (Park et al,
2005) that may probably differ in their genetic susceptibility to compounds in meat
− 19−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
products (Girard et al, 2008)(Satia et al, 2009)(Williams et al, 2009) (Ollberding et al,
2011).
-
In a recent follow-up study involving 53,988 participants followed over 13.4 y, no
associations were found between intake of red meat, processed red meat, fish, or poultry
and risk for colon cancer or rectal cancer (Egeberg et al ,2013). Surprisingly however,
specific associations with increased risks were found for lamb and colon cancer and for
pork and rectal cancer. The authors limit the relevance of their results and the
representative adequacy of their population however because of the low participation
rate of the population invited (35.5%) and the higher socioeconomic position of
participants than nonparticipants.
-
The lack of a significant relationship between red and/or processed red meat intake and
CRC risk reported in prospective studies from Japan (Takachi et al, 2011) and in
Singapore Chinese (Butler et al, 2008) may also be related to relatively low intakes
and/or intake differences compared to Western standards (Sato et al, 2006) as well as
limited numbers of subjects studied (Saebo et al, 2011). Apart from intake levels and
differences in meal preparation, gender differences are obviously also to be considered
when interpreting the absence of a relation of red meat intake to CRC incidence in a
prospective study of Chinese women (Lee et al, 2009).
Reviews
-
Two recent reviews of prospective studies conclude that the available epidemiologic
evidence is not sufficient to support an independent positive association between red
meat and processed red meat consumption and CRC, because of the likely influence of
confounding by other dietary and lifestyle factors, the weak magnitude of the observed
association, and its variability by gender and cancer subsite (Alexander et al,
2011)(Alexander & Cushing, 2011). The same authors reached a similar conclusion for
processed red meat (Alexander et al, 2010) although a significant summary relative risk
estimate for high (vs. low) processed red meat intake and CRC of 1.16 [95% confidence
interval (CI): 1.10–1.23] for all studies reviewed was obtained. However, these papers
are not very convincing as some bias in the authority/credibility of the papers and/or their
peer review can be suspected because:
The work was partially funded by the Beef Checkoff, through the National
Cattlemen’s Beef Association (NCBA-US), by the National Pork Board (NPB- US)
and by the Danish Agriculture & Food Council and only Alexander & Cushing (2011)
clearly disclosed ‘no conflict of interest’.
The convincing power of the papers might suffer from the specialized activities of
the senior author. He is indeed very active in refuting rather convincing evidence for
dietary factors affecting cancer and disease and published seven papers in 2010
refuting evidence for the relation of prostate, breast and colo-rectal carcinogenesis
as well as atopic dermatitis risk to consumption of red and processed red meat,
animal fat and partially hydrolyzed 100% whey protein respectively (references
available on request).
From the prospective studies retained by Chan et al (2011), three studies, dating
between 2006 and 2010 were not cited by Alexander & Cushing (2011) or Alexander
et al (2011). This may be related to the absence of a clear dose–response trend in
their work in contrast to the finding of Chan et al (2011). Also, three reports dating
between 1998 and 2009 related to processed red meats were cited by Chan et al
(2011) but not by Alexander et al (2010).
− 20−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
-
The definitions of red meat as used by Alexander & Cushing (2011) and by
Alexander et al (2011) may have included some processed red meat items. Also,
Alexander et al (2010) define processed red meats as “predominantly red meat
(although poultry and fish are sometimes included as well) that undergoes
preservation methods other than freezing” thereby including a series of non-cured
hamburger type products. In the earlier comprehensive reports however processed
red meat was clearly defined as “cured, smoked and nitrite treated meat products”
(WHO, 2003) or “meats preserved by smoking, curing or salting or by the addition of
chemical preservatives” (WCRF/AICR).
In an authoritative recent review Lund et al (2011) nevertheless refer to Alexander et al
(2010) and Alexander & Cushing (2011) as casting doubts on the WCRF findings. In a
further line of criticism they erroneously specify a limited case-control study (954 cases
and 959 controls) (Williams et al, 2010) as a cohort study and contrast it with a large
scale cohort study (300.948 individuals) (Cross et al, 2010). Such comparison is not in
line with the rigid quality criteria for data use as specified by WCRF (WCRF/AICR,
2007a; WCRF/AICR, 2011). It may be significant that the senior author has acted as
consultant for the British Pork and Beef executive. Similar criticism can be formulated in
relation to a more recent review (McNeill & Van Elswyk, 2012) where the senior author is
employed by the US National Cattlemen’s Beef Association and the argument
questioning the validity of the WCRF findings is based on an extensively cited reference
only available as Meeting abstract (Cho & Smith-Warner, 2004).
The main criticisms formulated in the review papers relate to:
The possible confounding of meat intake with other determining factors. It has
indeed been shown that persons with the highest intake of red meat compared with the
lowest consumed more total daily calories (Cross et al, 2007), were more likely to
smoke, had a higher body mass index, consumed lower amounts of fruits, vegetables,
fiber and calcium, engaged less frequently in physical activity, were less educated
(reviewed by Alexander & Cushing, 2011) and consumed more alcohol (Valencia-Martin
et al, 2011). It is however abundantly clear that the data used in the preparation of the
reports cited earlier have been corrected for such co-variates (see above). Furthermore,
the use of epidemiological data corrected for similar confoundings have led to other
generally accepted conclusions and recommendations. These include e.g. a greater
intake of fruits to five or more servings/day, the twofold increase of lung and other
cancers when smoking frequency increases from 2 cigarettes/day to between 10 and 16
cigarettes/day, the lower cardiovascular mortality with recommended fruit and vegetable
intake and the lower mortality with recommended dietary behavior as pointed out by
Demeyer & De Smet (2010).
The low relative risk measurements obtained. The often cited criterion of relative risks
<2.0 being low however does not apply to nutritional epidemiology where such values
are common. The excess risk in the highest category of processed red meat-eaters is
comprised between 20 and 50% compared with non-eaters, which is indeed modest as
e.g. Santarelli et al (2008) attributes a relative risk value of 20 to established risk factors
for lung cancer like cigarette smoking. A change of 50% in risk (e.g. a relative risk of 1.5)
may however be considered strong in nutritional epidemiology and a food associated
with a 20% increase in risk has a meaningful population effect on public health, though
limited when considered for the individual.The accurate documentation of present-day
meat intake of an individual is not easy because of the lack of precision of the dietary
assessment methods that are used in epidemiological studies. Such imprecision
systematically reduces the strength of association of determinants with the disease and
is referred to as attenuation or regression dilution bias.
− 21−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
A more reliable estimate of such “weak associations” may require estimates of the
“probability of an effect” rather than the use of statistical significance (Navia et al, 2010).
The probability of subtle bias or poor control of confounding factors. Apart from
the known confounding factors, it is possible or even likely that consumption of red
and/or processed red meats is associated with other important unknown lifestyle
behaviors and environmental factors affecting disease incidence and/or mortality not fully
accounted for in the analysis. The latter may include a limited final acceptability of
individuals and questionnaires (e.g. 47 % of the cohort approached in Ruder et al, 2011).
The importance of such confounding affecting mortality is reflected in the relation of a
higher intake of red meat to increased general mortality (cfr. “inverse causality” !) as
discussed by Mozzafarian (2009), de Abreu Silva & Marcadenti (2009) and Sinha et al
(2009). In agreement with Mozzafarian (2009), the importance of such residual
confounding in causing erroneous estimation of associations may be less than that of
other errors, such as random error in intake and outcome assessments. The latter may
include the site and type of tumor registered as molecular mechanisms underlying
tumours in the colon and rectum may be different (Li & Lai, 2009) and the former may
include e.g. the adequacy of the dietary questionnaires used and the precise
identification and measurement of meat in the diet involving e.g the transformation of
“servings/d” into g/d and the disaggregation of meat dishes (Prynne et al, 2009).
Correction based on validation of dietary food questionnaire results by comparison with
24-hr dietary recall values may indeed attenuate the statistical significance of relative
risk values (Parr et al, 2013). Last but possibly not least, residual confounding may be
related to the large variability in composition and processing of “processed red meats”,
reflecting the cultural characteristics of the study population, within or between
geographic locations.
Finally it may be worthwhile to remark that some papers are available not supporting the
hypothesis that meat consumption is a risk factor for CRC mainly based on case/control studies
however subject to effects of recall and selection bias because of a limited number of participants
studied over brief periods (e.g. in Tabatei et al, 2011; Williams et al, 2010). It is of course clear
that a definite proof based on a reversibility of the risk related to red and processed red meat
consumption has never been tested. Randomized controlled clinical trials with colo-rectal cancer
incidence as outcome measure indeed involve experimental requirements in terms of individuals,
duration as well as control and specification of food consumption. Such trials are very hard to
achieve although intervention trials are feasible and have shown that a low-fat dietary pattern
intervention can be maintained (Lanza et al, 2001) and did not reduce the risk of colorectal
cancer in postmenopausal women (Beresford et al, 2006).
Good alternatives for more reliable experimental evidence correctly refer to the need for the
development of meaningful biomarkers to more precisely reflect the nutritional factors relevant to
carcinogenesis (Boyle et al, 2008) (Altorf-van der Kuil et al., 2013). It is difficult to follow the
authors’ arguments however using the lack of a “convincing” association between fruit and
vegetables with cancer incidence and their covering of all cancers and carcinogenic factors in a
single discussion in rejecting recognition of an increased risk of colo-rectal cancer because of red
and processed red meat consumption (Ferguson, 2010). It is also striking and really not
acceptable that a limited number of recent review reports were published on meat and/or diet and
cancer or health not only without any reference to WCRF/AICR (2007) (e.g. Wicki & Hagmann,
2011; McAfee et al, 2010) but also lacking precision and completeness in the presentation and
discussion of data as pointed out elsewhere (Demeyer, 2010).
− 22−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.2.4 Recognition
Although it is clear from these arguments that residual confounding and methodological error
cannot be completely excluded in the 13 observational studies used (WCRF/AICR, 2011), it
should be reconfirmed that they are the only ones available allowing exploration of the complex
links between diet, physical activity and the development of cancer in free-living human
populations. They used a methodological framework to evaluate causality of the associations
found by exploration of key characteristics such as the effect size, the presence of a biological
gradient, the consistency of the effect, or the biological plausibility (WCRF/AICR, 2007a; Navia et
al, 2010). To cite Mann (2010) the WCRF “recommendations are based on clearly defined
'convincing' or 'probable' relationships between nutritional variables and disease outcomes”. Also,
because of the analogy with the evidence underlying the generally accepted recommendation for
an increased consumption of fruit and vegetables, it can be concluded that recognition of an
increased risk of colo-rectal cancer associated with red and processed red meat consumption is
based on “evidence based nutrition” and is therefore justified. It should also be recognized
however that:
accumulated evidence for a significantly increased CRC risk is without discussion only when
comparing relatively wide differences in intake with high upper levels (up to about 200 g/d);
evidence has been presented suggesting that other factors may be more important in an
elderly and ethnically diverse population (Ollberding et al, 2012).
Whether and to what extent this should lead to nutritional recommendations requires further
evaluation related to the nutritional and socio-economic importance of meat and meat products
and the nature of meat and meat products involved on the one hand and the magnitude and
position of the recognized risk within the overall risk pattern and the health costs of colo-rectal
cancer on the other hand. The epidemiological evidence presented has sofar inspired the
publication of both French (Programme National Nutrition Santé, France, 2009) and UK (Scientific
Advisory Committee on Nutrition, UK, 2010) official guidelines advocating a reduction of both red
and processed red meat consumption in reference to the increased risk of colorectal cancer.
Accordingly, a recent “position statement” of “The EU Eco-Management and Audit Scheme
(EMAS)” (Lambrinoudaki et al, 2013) providing “guidance concerning the effect of diet on
morbidity and mortality of the most frequent diseases prevalent in midlife and beyond” clearly
states that “The consumption of red or processed red meat is associated with an increase of
colorectal cancer.”
2.2.3 Importance of the risk associated with (processed) meat intake within the
context of other risk factors
2.2.3.1 Genetics
Although it is recognized that the incidence of CRC is predominantly related to
environmental/dietary factors it is also accepted that the genetic background plays a role in
modulating individual CRC risk factors. Genetic variants of the many genes investigated involved
in xenobiotic absorption and metabolism, DNA repair, insulin resistance, obesity and glucose
levels and inflammation may interact with the association of intake of meat and/or meat-related
carcinogens and the increased CRC risk (Landi et al, 2008). Genetic variants of drug
metabolizing enzymes (DME) (Fig. 3) involved in general pathways that bring about activation
and detoxification of carcinogens are often involved and cover at least 15 xenobiotic metabolizing
enzymes including cytochrome P450, glutathione S-transferase, UDP-glucuronosyltransferases,
sulfotransferases (SULT) and N-acetyltransferases (NAT).
− 23−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig.3. Schematic representation of the phase I and phase II drug-metabolizing enzymes (DMEs) and
the receptors that sometimes up or down regulate DME levels (From Nebert et al, 1999).
There is evidence of possible interactions between intake of meat and/or meat-related
heterocyclic amines (HCA) and polycyclic aromatic hydrocarbons (PAH) and genetic variants of
these enzymes with risk of CRC or advanced colorectal adenoma (Yoshida et al, 2008). Morita et
al (2009) from data obtained in a Japanese case-control study stated that colon cancer risk was
increased in relation to red meat intake only in individuals carrying a specific polymorphism of the
cytochrome P450 2E1 gene. Significant interactions between gene polymorphisms of enzymes
controlling intestinal absorption of HCA and tumor suppressor protein driving multiple cellular
responses to oxidative stress are associated with 50-60 % of CRC cases. The pattern of CRCassociated TP53 mutations was found to be geographically clustered as well as related to
availabilities of the Western energy-dense foods meat, milk, sweeteners and animal fats, in a
study involving 2,572 CRC-associated mutations from 12 countries/geographic areas (Verginelli
et al, 2009). Inherited polymorphisms of key genes may be involved but more commonly
spontaneously arising mutations affecting genetic control of all processes determining cellular
growth induce CRC. More intricate relationships involving such epigenetics were recently
demonstrated between CRC incidence and polymorphisms of both untranslated regions of
messenger RNAs and the small endogenous micro-RNA molecules binding to these regions
thereby regulating mRNA cleavage or repression of protein synthesis (Landi et al, 2008; Landi et
al, 2011). It is clear that geographic and individual differences in exposure to and repair of DNA
damage due to foods relate to the extreme complexity and variability of food production,
processing, preservation, and preparation. Citing Verginelli et al (2009) the latter add to “the
complexity of interactions determining intestinal mutagenesis modified by nutrient/nutrient,
nutrient/microflora, nutrient/cell metabolism, nutrient/gene and nutrient/DNA repair interactions,
and affected by epigenetic modifications, transit time of dietary residue, inflammatory and
endocrine responses, body mass and energy consumption through physical activity” underlying
the variability and inconsistency of the reported (epi)genetic interactions with the association of
meat(products) with CRC risk. Limited and inconsistent relationships of metabolic gene
polymorphisms with the meat associated CRC risk have been reported. (Ferrucci et al, 2010)
(Zhao et al, 2012) and epigenetics contribute undoubtedly to the complexity of interactions
involved and underlying the many possible errors and confounding factors affecting epidemiology.
Nevertheless, Hutter et al (2012) recently concluded from a survey of nine cohort and case
control studies that single-nucleotide polymorphisms (SNP) at 10 loci associated with colorectal
cancer (CRC) were not associated with other risk factors. A similar study concluded that NAcetyltransferase 2 phenotypes may not be associated with colorectal cancer development
(Zhang et al, 2012a). Meta-analysis suggests a lack of association between N-acetyltransferase 1
NAT1 polymorphisms and individual risk to CRC (Cai et al, 2012). Only a NAT1 polymorphism
modified the association between MeIQx intake and colorectal adenoma (precursor of CRC) risk.
− 24−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
By the same token, the results of a Swiss case-control study (Barbir et al, 2012) indicated that
HCA intake is positively associated with colorectal adenoma risk, regardless of phenotypes
involved in the xenobiotic metabolizing enzyme genes. Cytochrome P450 2E1 (CYP2E1) is a
natural enzyme involved in the metabolic activation of many carcinogens and meta-analyses
have shown association between some cytochrome P450 polymorphisms and CRC risk (Qian et
al, 2013) but not with others (Mei et al, 2012) (Zhao et al, 2013) (Peng et al, 2013). Another metaanalysis confirmed that the NAT1 genotype was not significantly associated with an elevated
CRC risk but suggests that individuals with NAT2 genotype had an elevated risk of CRC (Liu et
al, 2012), confirmed by the higher susceptibility for CRC of NAT2 carriers with high HCA intake
(Voutsinas et al, 2013). Meta-analysis also showed that a polymorphism of a microsomal
epoxide hydrolase may have a potential protective effect on CRC (Liu et al, 2012a) whereas from
a limited case-control study involving 264 individuals, Bajro et al (2012) suggest that a
polymorphism involved in the promotion of the uridine diphosphoglucuronate
glucuronosyltransferase 1A1 gene, a key hepatic detoxification enzyme, is a risk factor for
colorectal cancer in a Macedonian male population.
It can be concluded that in spite of some inconsistency, the majority of recent reports suggest that
gene polymorphisms of major detoxifying enzymes do not modify meat consumption related CRC
incidence: in a large and comprehensive study relating xenobiotic metabolizing enzyme gene
polymorphisms, meat mutagens and the risk of colorectal tumors Gilsing et al (2012) could not
find modifying effects of gene polymorphisms on CRC incidence and only limited suggestions for
diet-gene interactions and CRC risk were obtained in a recent meta-analysis (Andersen et al,
2013). In an analogous consideration Yarnall et al (2013) have suggested that modification of
behaviour, including consumption of red and processed red meat, alleviates genetic risks. It
should be realized however that genetic investigations into meat induced increased susceptibility
to CRC may need studies of combined rather than indidual SNPs. Indeed, although Küry et al
(2007) confirmed that such increase was not affected by individual SNPs of cytochrome P450
genes, three allelic variant combinations however, present in around 4% of the population
studied, were associated with a 50-fold increased CRC risk because of red meat consumption
over five times per week. Also, newer cell structure related gene polymorphisms associated with
CRC risk warranting further research were recently identified in a large genome-wide metaanalysis (Colon Cancer Family Registry and the Genetics and Epidemiology of Colorectal Cancer
Consortium, 2013).
2.2.3.2 Other modifiable risk factors
WCRF/AICR (2007, 2011) studied diet (food and nutrition) and physical activity but also
recognized that (cigarette) smoking is an important established carcinogenic factor, also for CRC
(Liang et al, 2009). Socio-economic status, another confounding factor possibly affecting the
relation diet~CRC has been ruled out by Major et al (2011). This may be associated however with
eating behavior and it has been shown that “eating anything at anytime” increases risk of CRC
incidence in another large American prospective cohort study, independent of other potential risk
factors (Bao et al, 2012). In line with the effects of “Westernization”, physical activity, obesity
{using BMI (body mass index), waist circumference or other indices of body fat}, diet, smoking
and alcohol intake are the main five factors that have been associated with the development of
CRC. In an extensive review, Huxley et al (2009) used reports identified between 1966 and
January 2008 through EMBASE and MEDLINE including 103 cohort studies. They concluded that
individuals consuming the most alcohol (> 60 g/d) had a 60% greater risk of CRC compared with
non- or light drinkers whereas smoking, diabetes, obesity and high meat intakes were each
associated with a significant 20% increased risk (comparison of individuals in the highest and
lowest categories for each). Relative risk factors, recently estimated and compared from metaanalyses involving studies on 12 established CRC risk factors suggested that the consumption of
red meat is associated with a much lower risk than inflammatory bowel disease and a history of
CRC in first-degree relatives. The risk is similar to increased BMI, cigarette smoking, low physical
activity and low vegetable and fruit consumption (Johnson et al, 2013). Such data are in line with
− 25−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
estimates shown in Table 2 illustrating e.g. that the convincing risks associated with alcohol use
and processed red meat consumption are similar. The independent relative importance of these
factors has been estimated using multivariate statistical models but this has limitations because
of the interrelationships between these factors: a high meat intake is associated with high alcohol
consumption (Valencia-Martin et al, 2011) whereas animal protein consumption, mainly from red
and processed red meat and poultry, is associated with body weight gain both in Europe
(Halkjaer et al, 2011; Romaguera et al, 2011) and the US (Wang & Beydoun, 2009), a finding
corroborated in Belgium where “plant protein could offer a protective effect in the prevention of
overweight and obesity” (Lin et al, 2011). However, it should again be realized that these findings
require a specification of “meat” as differential effects on BMI were observed for several subtypes
of meat (Gilsing et al, 2012a). The need for specification of meat and meat products is perhaps
best illustrated by the recent consideration of “meat” as “a low-fat food” associated with lowered
BMI values (Mullie et al, 2012). In spite of these limits, Parkin et al (2009) proposed potential
contributions of separate individual lifestyle recommendations for prevention of CRC in the UK.
Their results as reported for males indicate that a lowering of the consumption of meat and meat
products from 90 g/d to 80 g/d would save 2129 cases equivalent to an 8 % lowering of the
incidence, compared to an overall lowering of 31.5 % when all recommendations are met. A
similar conclusion was reached by Kirkegaard et al (2010): in a Danish prospective cohort study
involving 55 487 men and women 13% of CRC cases were attributable to lack of adherence to
only one recommendation of five proposed: physical activity, waist circumference, smoking,
alcohol intake and diet. The latter involved a “dietary index” covering consumption of fruit,
vegetables, fat and fiber as well as consumption of ≤500 g of red and processed red meat per
week.
Table 2. Summary estimates of convincing relative risks of CRC from cohort studies (adapted from
Corpet, 2011 and WCRF/AICR , 2011).
Factor
% changea
Relative risk
Per
Waist to hip ratio
Red meat
Alcohol
Smoking
Processed red meat
Body mass index
Dietary fiber
Adult attained height
30
29
27
25
21
15
10
9
1.30
1.29
1.27
1.25
1.21
1.15
0.90
1.09
0.1 increase
100 g/d
30 g/d
Ever vs never
50 g/d
5 kg/m2
10 g/d
5 cm
a
100 times the absolute value of (relative risk – 1)
2.2.4 Possible impact on prevention in Belgium
A conservative and rough application of these estimates to the Belgian situation suggests that the
lowering of average fresh red and processed red meat consumption from 95 g/d (Data in table 5
estimated from De Vriese et al, 2006) to 50 g/d might save about 1200 cases (~ 15 %) out of the
total of 7790 (for 2006 from Pacolet et al, 2011). Such intervention agrees with the aims of a
European action against colon cancer (http://www.stopcoloncancer.info/) and with similar
effectiveness as the saving (~ 20 %) associated with preventive screening for the disease as
discussed by Atkin (1999) and Frew et al (1999). It is of course clear that primary prevention
through nutritional strategy cannot be an alternative to the latter secundary prevention. At least
one argument is: the latter immediately detects unrecognized disease whereas the preventive
effect of the former may require a minimal time span of ten to fifteen years (Bejar et al, 2010). It
has been suggested that justified and efficient official recommendations for dietary interventions
− 26−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
should involve cost-benefit analyses based on cost estimates of disease treatments as well as
the disability-adjusted life years lost and their impact on workforce participation and productivity
(Lenoir-Wijnkoop et al, 2013). Such approach within “nutrition economics” could even incorporate
genetic and ethnic differences in disease susceptibility of target populations (Bhopal et al, 2012)
(Lang & Barley, 2013) but is considered to exceed the available expertise of the authors as well
as lacking justification because of the limited precision of the information and importance of the
possible impact.
2.2.5 The importance of meat in nutrition
2.2.5.1 Consumption and recommendations
Meat and processed red meat products are important dietary components in Western
industrialized countries and represent on average about 11 and 5 % of total dietary energy intake
respectively (Table 3).
Table 3. The contribution of meat to total dietary energy intake (Linseisen et al, 2002)
Greece
Spain
Italy
France
Germany
The Netherlands
UK
Denmark
Sweden
Norway
Total meat
(% of total energy)
Women
Men
7.0
8.1
13.5
16.0
10.4
10.7
11.4
10.8
14.9
11.4
14.5
8.5
9.3
9.5
11.9
10.8
12.8
10.5
-
Processed red meat
(% of total energy)
Women
1.0
6.2
3.6
3.9
6.2
5.3
2.8
3.3
5.3
5.9
Men
1.2
7.5
4.4
9.4
7.5
3.7
5.2
6.4
-
EU
10.4
4.4
5.7
12.3
Similar data can be calculated from the results of the 2004 Belgian National Food Consumption
Survey (Food Consumption Survey, Belgium, 2004) discussed in terms of energy and
macronutrient intake by Temme et al (2010) and Lin et al (2011) (Table 4).
− 27−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 4. Contribution of fat and protein in meat products and processed red meats to total energy
intake in Belgium [approximate estimates calculated from Temme et al (2010) and Lin et al (2011)].
Contribution to total
energy intakea
Fat
Protein
Carbohydrates
Total Macronutrients
37 %
16 %
47%
100 %
Meat Products
(Processed red
meats)
6.9
(2.6)
5.2
(1.6)
NE (low)b
12.1
(4.2)
Dairy and butter
8.7
5.3
NE (low)
14.0
Plant products
8.8
(margarine;oils)c
5.5
(cereals)
25
(cereals)
39.3
12.6
NE (low)
22
(drinks, sugar)
34.6
37%
16%
47%
100.0 %
Contribution of food
groups
Energy-dense
micronutrient poor
foodsd
a
b
8560 kj/d (value corrected for underreporting = 9496 kJ/d) value considered to be low and not
c
d
estimated () = main food groups involved groups cakes; condiments; sauces; sugar; drinks
From the arguments presented above, it is clear that recommendations on eating for prevention
of CRC require a food-based formulation based on nutrient intake and reference values, in
analogy with the development of dietary guidelines for healthy eating.
The latter values are described by the national health authorities (Hoge Gezondheidsraad –
Conseil Supérieur de la Santé, 2009) and have been translated in largely similar food-based
dietary guidelines developed by the regional health authorities. From a comparison of food
consumption data with the Flemish food-based dietary guidelines (Vanhauwaert, 2012)
(Vandevijvere et al, 2009), it can be calculated that the average consumption of meat and meat
products (including poultry) exceeds the recommended value of 100g (Table 5), a value
recommended for the food group meats/fish/eggs/legumes/substitutes.
Table 5. Recommended and actual consumption of food groups in Belgium for 2004 (From
Vandevijvere et al, 2009)
Food group
Recommended (g/d)
Consumed (g/d)
Meats/fish/eggs/legumes/substitutes
Meats and meat productsa
fresh beef, veal, pork, sheep,
horse and goat
processed red meats
poultry
<100
161
121b
61b
Nutrient-poor foods (alcohol excluded)
<100c
Nutrient-poor foods (alcohol included)
<100c
a
32b
19b
b
295
529
c
including poultry From Food Consumption Survey, Belgium (2004) According to the recommendations,
this intake should be 0.
− 28−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
The excess (61 %) is not as high as for nutrient-poor foods (195 or 529 % without or with
inclusion of alcohol) indicating that the latter food group may be more important in relation to
energy intake and obesity incidence than meat and meat products as discussed elsewhere
(Demeyer, 2008). The estimated consumption of 121 g/d meat and meat products (for 2004,
including poultry) compares with consumption data calculated from data provided by the meat
industry
and
agricultural
organizations
(http://archive-be.com/page/49027/2012-0611/http://www.vlam.be/facts/info_nl.phtml?id=7) : ca. 134 g/d including ca. 90 g/d total fresh red
meat (data for 2010 excluding poultry) and 44 g/d for processed red meat (“charcuterie”
consumption over the last decade). It is however lower than the data reported earlier for 19801985 (Dehenauw & De Backer, 1999): 178 g/d including 157 g/d of fresh meat and 21 g/d of
processed red meat, illustrating a shift towards processed red meat consumption. There is a clear
regional government support for the recommended maximal value of 100 g/d “total meat”
consumption although the difference between “total meat” and the food group
“meats/fish/eggs/legumes/substitutes” is not consistently present in the arguments
(http://www.vilt.be/index.php/nl_BE/news/show/id/108094) and at the national government level
the value is lowered to 75-100 g/d (in “Nationaal voedingsplan voor een betere gezondheid“ “Plan
National
Nutrition
pour
une
meilleure
santé”
at
http://www.belgium.be/nl/gezondheid/gezond_leven/voeding/nationaal_plan/ or
http://www.belgium.be/fr/sante/vie_saine/alimentation/plan_national/)).
2.2.5.2 Sustainable meat consumption meeting dietary requirements for health
An important part of the industrialized population has lowered or considers to lower meat
consumption, to a large extent based on legislations limiting meat production to reduce
greenhouse gas emissions (see e.g. Mithril et al, 2012) as discussed in detail by Millward &
Garnett (2010). Recent evaluation of the water footprint of EU food consumption has led to a
similar intention (Vanham et al, 2013). Nevertheless, apart from ecological considerations,
healthiness was the most salient stated reason for the intention of 52 % of the Finnish consumers
to lower meat consumption (Latvala et al, 2012). de Boer et al (2013) recently concluded that for
motivation of consumer food choices it is preferable not to isolate the meat-climate issue but to
develop an approach combining multiple values, including health. Combining health and
environmental arguments McMichael et al (2007) e.g. recommended a global lowering of red
meat intake coming from ruminants to 50 g/d. In authoritative approaches covering all meat
related disease effects, detailed modeling by both epidemiologists and ecologists (Scarborough
et al, 2012) (Powell & Lenten, 2012)( Macdiarmid et al, 2012) has integrated and evaluated
harmful effects of Western high meat diets and the trend to higher meat diets in e.g. East-Asia
and India for both human health and climate change. Scarborough et al (2012) conclude a 50%
reduction in meat and dairy replaced by fruit, vegetables and cereals would result in a 19%
reduction of greenhouse gas emissions as well as in the delay or aversion of about 37000 deaths.
Recently, Aston et al (2012) estimated that moving from the higher to the lower fifth of existing
red and processed red meat consumption level in the UK would lower CRC risk by about 16 and
25 % for women and men respectively, associated with a 3 % reduction in the current GHG
emission level. Even in the US, environmental considerations generated a USDA proposal for a
“Meatless Monday” similar to and even inspired by an initiative in Flanders (e.g.
http://www.vilt.be/Gentse_Veggiedag_krijgt_navolging_in_wereldsteden). This proposal was
withdrawn however after vigorous protest by the US National Cattlemen’s Beef Association
(http://www.beefusa.org/newsreleases1.aspx?newsid=2560) also stating that health concerns of
meat “are not based on facts but statistics and rhetoric generated by anti-animal agriculture
organizations”. From a public health perspective it is hard to accept such statements and it has
been argued that reactions to the situation should be based on science based education on
health of the consumer, highlighting ample scientific research indicating that red meat can be
consumed daily (Schonfeldt & Hall, 2012). It should also be recognized however that the need to
“feed more people better, with less environmental impact“ does not only pose challenges to
production and consumption but also involves socio-economic challenges, requiring “changes in
− 29−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
how the food system is governed” (Garnett, 2013). Similar considerations, involving both
moderation of meat consumption and production balanced by a “fair price“ policy for the farmer
were
recently
also
proposed
by
the
Flemish
farmers
organization
(http://www.vilt.be/Matiging_vleesconsumptie_en_correcte_voedselprijzen).
It has been authoritatively confirmed that “appropriately planned” vegetarian and even vegan
diets “are healthful, nutritionally adequate, and may provide health benefits in the prevention and
treatment of certain diseases” (Craig & Mangels, 2009) whereas a “well-balanced lacto-ovovegetarian diet, including dairy products, can satisfy all nutritional needs of the growing child”
(Van Winckel et al, 2011). Camilleri et al. (2013) recently demonstrated that plant protein is a
robust marker of a healthy diet, different subtypes of animal protein largely vary in their
relationschip with diet quality. It should be realized however that such statements refer to
effectively controlled diets in industrialized countries and it has also been shown that moderate
amounts of red meat (~ 100 g/d for adults) remain valuable sources for net protein synthesis for
the elderly (Symons et al, 2009) and improve development of breast fed infants (Krebs &
Hambidge, 2006), toddlers (Krebs et al., 2011) and children in developing countries (Mills et al,
2007). Recently, McEvoy et al (2012) recognized the convincing link between red meat and
particularly processed red meat intake and disease, in support for a plant-based diet. They also
concluded however that prudent plant-based dietary patterns that allow small intakes of red meat
besides fish and dairy products have demonstrated significant improvements in health status. It
should therefore be accepted that a sustainable diet lowering greenhouse gas emissions and
meeting dietary requirements for health can be achieved without complete elimination of meat
(Macdiarmid et al, 2012). In addition, practical dietary and culinary recommendations should be
made for cancer prevention involving e.g. practices to lower heterocyclic amine formation during
cooking (Lecerf, 2012). Extreme reactions from the “meat world” may generate and conflict with
more science based arguments in favor e.g. of a tax on meat consumption to reach significant
mitigation of climate change (Nordgren, 2012).
It is therefore appropriate to briefly review how a lowered red meat intake may affect the intake of
the major energy dense essential nutrients present in red meat and processed red meats.
2.2.5.3 Meat in essential nutrient supply
Iron (Fe): Apart from protein, Fe is probably the nutrient most discussed in relation to red
meat intake focusing on iron deficiency-anemia and the difference in absorption of heme-Fe
and non-heme plant Fe as e.g. in Hoge Gezondheidsraad – Conseil Superieur de la Santé
(2009). Both items are however subject of reconsideration because recent newer insights
have made clear that:
-
The incidence of Fe deficiency as reflected in low circulatory Fe values (e.g. transferrin
saturation) or iron intakes below the WHO recommended intakes (20 and 9 mg/d for
women and men respectively) far exceeds the incidence of anemia (Stoltzfus, 2001):
only 50% of anemia is associated with Fe deficiency. It has recently been reported that
borderline levels of circulatory iron may be related to brain iron deficiency, as reflected
in fatigue of nonanemic menstruating women (Vaucher et al, 2012) and in ADHD of
children (Cortese et al, 2012). However neurodegeneration with brain iron accumulation
also occurs (Schipper, 2012). Nevertheless it has been reported that no clear functional
disabilities have been associated with Fe intakes below the recommended values
(Millward & Garnett, 2010) whereas it has been suggested that UK dietary iron
requirements may be too high and should be reviewed (Scientific Advisory Committee on
Nutrition, UK, 2010). In this respect, it is quite striking that in the 2004 consumption
survey Fe consumption was below recommended values in 70 % of the female
population (Food Consumption Survey, Belgium, 2004) whereas Huybrechts et al (2012)
found that “almost half of the Flemish preschoolers do not comply with the dietary iron
recommendations”.
− 30−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
-
The above may be related to the single value of Fe availability (15%) used in the
development of recommended intake values for Western countries whereas it is now
clear that intestinal absorption of Fe and its further metabolism is tightly regulated by
very complicated mechanisms related to the Fe and general metabolic state of the
individual. From the average adult intake of 10-15 mg/d, 1-2 mg is absorbed in the
enterocyte involving reduction of Fe3+ to Fe2+ and facilitated transport by metal and heme
(?) transporter proteins to be stored as ferritin or transferred across the cell membrane
involving the transporter protein ferroportin and bound to transferrin in plasma. The
synthesis of ferritin and transferrin varies with the size of Fe stores through the variable
binding of Fe regulatory proteins to Fe responsive elements in the mRNA’s controlling
expression of proteins such as ferritin and transferrin (Hentze et al, 2010). The synthesis
of ferroportin and transporter proteins is controlled by hepcidin, a key peptide in Fe
homeostasis, synthesized in the liver. Its synthesis and that of other interacting Fe
metabolism proteins such as hephaestin, a Cu containing ferroxidase, is itself controlled
by complex modulation of the relevant gene expressions mediated by cytokines
(Interleukin-6) and Fe homeostasis related formation of labile radicals formation
(Crichton et al, 2002; Andrews, 2005; Weiss, 2009; Tussing-Humphreys et al, 2012) (see
e.g. Fig. 4). Hepcidin expression is increased in chronic inflammation and obesity and is
associated with Fe deficiency observed in overweight children, irrespective of Fe intake
and availability of supply (Hurrell & Egli, 2010). Another process necessitating effective
control of Fe absorption as well as inter- and intracellular transport is the potential
toxicity of Fe2+ mediated through hydroxyl radical formation via the Fenton reaction. It
has therefore been proposed to develop a range of iron bioavailability factors based not
only on diet composition but also on subject characteristics, such as iron status and
prevalence of obesity (Hurrell & Egli, 2010).
-
As discussed by Millward & Garnett (2010) and Hurrell & Egli (2010) hepcidin is mainly
involved in the up-regulation of non-heme Fe absorption at low heme Fe (meat) intakes
associated with low iron stores (ferritin) compared to higher meat intakes. Apart from
dietary Fe absorption effectors inhibiting (phytate, polyphenols and Ca) or stimulating
(ascorbic acid) Fe absorption, this is obviously an effective mechanism as vegetarians in
developed countries do not have a greater incidence of Fe-deficiency anemia, reflecting
the existence of another but effective Fe homeostatic equilibrium. The above reasoning
has been developed in evidence-based detail by Geissler & Singh (2011) and supports
the conclusion of the UK Scientific Advisory Committee on Nutrition (2010) that even at
zero meat intake the impact on Fe intake is very little, with the implicit equivalence of Fe
from meat and from non-meat sources (Millward & Garnett, 2010). In line with this, a
meat consumption effect on iron absorption was not supported by the absence of an
effect of meat intake on anemia in children and/or adolescents in Japan (Kunitsugu et al,
2012) and in developing countries (Krebs et al, 2012a). According to Food Consumption
Survey, Belgium (2004), meat and meat products account for 20 % of total Fe intake and
the above reasoning allows for the conclusion that the intake of meat and meat products
can be lowered considerably without negative effect on the incidence of anemia. Some
consideration should perhaps be given to consumers at higher risk for iron deficiency:
children, women of reproductive age and adults aged over 65 y.
− 31−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig. 4. Regulation of body iron homeostasis by hepcidin (From Collins et al, 2008).
Protein: The population daily total protein intake as recently reported for Belgium (Lin et al,
2011) amounts to 85 and 50 g/d for males and females respectively, representing about 15 %
of energy intake, in line with the upper levels of recommendations (10-15%). As shown in
Table 6 fresh and processed red meat represent 22 and 10 % of total protein intake
respectively. Although it is recognized that protein quality expressed as the protein
digestibility corrected amino acid score (PDCAAS) is lower for plant than for meat proteins,
mainly because of a lower digestibility, it has been established that essential amino acid
content (mg/g protein) for both high- and low animal sourced foods exceeds the requirement
pattern in Western diets (Fig.5).
Soy protein in particular approaches the PDCAAS of lean meat, in contrast to cereal proteins.
For all practical purposes plant and animal proteins can thus be considered equivalent at the
total intakes and food diversities observed in developed countries. This is indeed reflected in
the Flemish food-based dietary recommendations where meat, fish, eggs and alternatives
(soy products) are grouped in the same recommended daily intake of 100 g (Vanhauwaert,
2012) (Vandevijvere et al, 2009). Nevertheless, convincing evidence has been presented for
a superior effect of beef compared to soy protein on protein turnover in the prevention of
sarcopenia, e.g. the age related gradual loss of skeletal muscle mass (Phillips, 2012). It has
indeed been shown that the fast speed of meat protein digestion, affected by cooking
temperature (Bax et al, 2013) or mincing (Pennings et al, 2013), stimulates protein synthesis
more efficiently than slow proteins after exercise or in the elderly (Rémond et al, 2007). Such
higher rate of digestion may contribute to the need for adequate meat intake to ensure
appropriate supply of high quality protein as well as of other key micronutrients especially for
individuals most at risk of malnutrition. These include adolescents, women of childbearing
age, pregnant women, the elderly, and those individuals with a high level sport activity
(Bourre, 2011) as well as populations with deficient nutritional status in developing nations
(McNeill & Van Elswyk, 2012). In this respect it can e.g. be mentioned that in Belgium, meat
− 32−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
and meat products are major sources (31%) of a selenium intake considered to be at the
lower end of the recommended value (Waegeneers et al, 2013).
Table 6. Intake of protein (g/d) from different foods in Belgium for 2004 (Lin et al, 2011)
Protein Sources
Males
Age (years)
15-18
>75
15-18
>75
Animal
56
15
36
19
8
8
4
1
29
22
58
13
36
19
10
8
7
2
28
18
33
10
19
10
5
5
3
1
18
13
35
9
22
12
5
6
4
1
15
9
85
86
51
50
Dairy
Meat & Meat Products
Fresh
Processed
Poultry
Fish & Shellfish
Eggs & Egg products
Plant
Cereals
Total
Females
Fig.5. Amino acid pattern (mg/g protein) of high (
) and low (
) animal sourced food diets and
the requirement patterns for adults ( ) and children (1-2 years old) ( ) (From Millward & Garnett,
2010).
Zinc (Zn) : In a typical Western diet, red meat makes a greater contribution to total Zn than to
total Fe intake indicating that a lowered intake of red meat and processed red meats may be
more critical for Zn than for Fe supply. Regular consumption of either meats or zinc-fortified
foods was shown to meet required zinc absorption (Krebs et al, 2012) and a positive
relationship between red meat intake and hair zinc levels was observed (Ozden et al, 2012).
Both Zn and Fe are ‘‘problem nutrients’’ for breastfed infants in developing countries and
supplementation with beef compared to a Fe fortified cereal (Krebs & Hambidge, 2006) or Zn
sulfate (Kumar & Ramji, 2012) have improved infant development. Overt Zn deficiencies have
− 33−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
however not been observed in developed countries and, analogous to Fe, plasma Zn
concentrations are not consistently or significantly correlated with Zn intake, indicating that an
efficient homeostatic control ensures “a normal range” of plasma Zn levels (Hoge
Gezondheidsraad – Conseil Supérieur de la Santé, 2009)(Millward & Garnett, 2010). There is
evidence of up-regulation of Zn absorption at low intakes and plasma Zn levels do usually not
differ between meat eaters and vegetarians (Hunt, 2003). Nevertheless, Belgian
recommendations (Hoge Gezondheidsraad – Conseil Supérieur de la Santé, 2009) refer to a
30 % average absorption of dietary Zn, to be lowered to 20 % for a diet poor in animal source
foods. Recommended intake levels are therefore increased for diets low in animal sourced
foods and even more for vegetarians. Millward & Garnett (2010) report that reducing the
intake of red meat and processed red meats to 70 g/d would increase the percentage of the
population with Zn intakes below the lower reference intake to 4-5. However, entirely plantbased dietary Zn and the presence of other animal sourced foods would “in reality” maintain
near normal levels of plasma Zn because of the control of homeostasis although there may
be a problem for children.
Vitamin B12 (B12): It is evident that B12 has to be considered in an evaluation of nutrient
supply by red meat and processed red meats as animal foods are the only source of this
vitamin. The lowest B12 concentration is present in milk and dairy products (0.3–0.4 μg/100 g)
a value lower than for eggs (0.9–1.4 μg/100 g) or meat and fish (3 and 33 μg/100 g) (Van
Winckel et al, 2011). The B12 intake in Europe ranges between 2 and 6 µg/d compared to a
recommended intake of 1.4 (Hoge Gezondheidsraad, 2009) or 2,4 (WHO/FAO, 2004) µg/d for
adults, to be increased for pregnant and breast feeding women. There is therefore little
evidence for symptoms of B12 deficiency (megaloblastic anemia and various neurological
disorders including dementia) in Europe, apart from the elderly population because of
malabsorption of food-bound B12 caused by gastritis and in some groups of vegans because
of the total absence of animal sourced foods. Plasma B12 levels however are a poor indication
of functional B12 deficiency and functional indicators such as plasma or urinary methylmalonic
acid suggest that B12 deficiency may be more common and cognitive decline associated with
methylmalonic acid has been observed in high proportions of institutionalized elderly. Plasma
B12 levels do however reflect intake of supplements, fortified cereals and milk but less so
intake of meat, poultry and fish suggesting a higher availability of B 12 from dairy products. The
promotion of a high intake of dairy products to ensure adequate B12 intake has therefore been
suggested, not able however to compensate a lowering of the overall intake in the total
absence of fish and meat (Millward & Garnett, 2010). Accordingly Van Winckel et al (2011)
state “all persons consuming fish or meat less than once weekly are at risk of vitamin B 12
deficiency” . The proportion of red meat and processed red meat products representing 58 %
of “Meats/fish/eggs/legumes/substitutes” consumption (calculated from Table 5), the
consumption of dairy products and the availability of B12 enriched soy products and cereals
therefore allows for a substantial lowering of red meat and processed red meat consumption
without risk for B12 deficiency. An exception should perhaps be made for vegans, that have to
obtain B12 from regular use of B12-fortified foods.
Vitamin D: In view of the recent report demonstrating suboptimal blood levels of 25hydroxycholecalciferol (25(OH)D) in 80 % of 1006 European adolescents (Gonzalez-Cross et
al, 2012), considerable attention should also be given to the dietary supply of vitamin D by
meat.
Sodium (Na): Na represents a special case as a lowering of processed red meat
consumption may indeed lower Na intake, a desirable effect. Indeed, evidence based
nutritional recommendations do advocate a limitation of salt intake to 5 g/d ( about 2 g of
Na/d) (Hoge Gezondheidsraad, 2009). Vandevijvere & Van Oyen (2008) estimated a mean
Na intake of 2.7 g/d from the 2004 food consumption survey but this excluded added salt in
the kitchen and on the table. A later limited study of 24 h-urinary samples showed that the
− 34−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
actual salt intake amounted to about 9-12 g/d (Vandevijvere et al, 2010). A recommendation
for salt reduction in foods was therefore officially issued recently by Belgian Health authorities
(Advisory report SHC 8663 Reformulation of foodstuffs – salt reduction at www.css-hgr.be).
Second in line after bread and cereals, meat products (processed red meats ?) were found to
contribute about 20 % of total Na intake, a value close to the 18 % found for the contribution
of processed red meats to Na in purchased foods in the UK (Mhurchu et al, 2011).
Accordingly, Schmid et al (2011) considered the salt content of Swiss cured cooked meats
high enough to recommend their “restricted” consumption. It should however be realized that
the Na content of processed red meats very often exceeds that accounted for by salt (NaCl)
(Vandendriessche, 2008). This issue supports a limitation of processed red meat intake quite
apart from the CRC issue, parallel with initiatives of the meat industry to lower the use of salt
in food technology
(http://www.fenavian.be/uploads/documentenbank/b6d4e6664bfb8230d8a231c117fea823.pdf
2.2.6 Carcinogenic mechanisms
Recognition of an increased risk of CRC linked to red and processed red meat consumption is
based on “evidence based nutrition”. Such observational evidence however does not explain how
red meat and processed red meats can increase CRC risk, a problem to be solved only using
experimental evidence based on hypotheses. Excluding “inverse causality” hypotheses should
obviously involve the presence of specific components in red meat and processed red meats
inducing the accumulation of the typical events characterizing the development of CRC.
Approximately 5% of all CRC cases are due to inherited genetic mutations, including many
syndromes such as Familial Adenomatous Polyposis and Lynch syndrome (Al-Sohaily et al,
2012). However, most cases of CRC are termed sporadic and have been linked to environmental
causes including the consumption of red and processed red meat rather than to heritable genetic
changes. Like other types of cancer, the development of CRC is a multistep process. CRC arises
in the majority of the cases as a benign adenomatous polyp, which develops into an advanced
adenoma with high-grade dysplasia and finally progresses to an invasive cancer (Sanford &
McPherson, 2009). Genomic instability appears to be an integral part in this transformation
processs (Al-Sohaily et al., 2012). In an initial attempt to characterize multistep carcinogenesis,
Fearon and Vogelstein proposed a model in which specific genetic alterations are associated with
the sequential evolution of the neoplastic phenotype in the colon (Boland & Goel, 2010).
According to this model (Fig. 6), a mutation of the adenomatous polyposis coli (APC) gene is the
earliest genetic change in CRC leading to the initial appearance of the adenoma from normal
colonic mucosa. In the absence of the functional APC protein, the Wnt signaling pathway,
passing signals from receptors on the cell surface to the nucleus, will be inappropriately and
constitutively activated. This pathway is normally initiated by the oncoprotein beta-catenin and
results in the transcription of several genes affecting proliferation, differentiation, migration and
apoptosis (Al-Sohaily et al, 2012). As the APC protein is a component of the complex that
stimulates the proteasomal degradation of beta-catenin, changes in its gene will result in an
unregulated production of beta-catenin stimulating proliferation of epithelial cells (Tudek &
Speina, 2012). Some hereditary cases of CRC are associated with germ-line APC mutations. In
carriers of the mutant gene, the risk of CRC by the age of 40 years is close to 100% (references
in Markowitz Bertagnolli, 2009). During the further progression of the adenoma, Fearon and
Vogelstein observed other changes in genetic regulation, such as induction of the KRAS
oncogene resulting in growth of the adenoma and loss of function of tumor suppressor genes on
chromosome 18q inducing further adenoma growth and progression. In the model of Fearon and
Vogelstein, loss or inactivation of p53 gene function takes place in a late stage and is believed to
be the defining event that drives the adenoma to carcinoma (Itzkowitz & Yio, 2004). Although this
model has been useful, combination of mutations of these genes in the same cancer is
uncommon and CRC pathways beyond the Fearon and Vogelstein model have been identified
(Al-Sohaily et al, 2012). Today, three distinct molecular pathways of genomic instability in colon
− 35−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
carcinogenesis have been recognized: the chromosomal instability pathway, the microsatellite
instability pathway and the CpG island methylator phenotype pathway (Itzkowitz & Yio, 2004).
Tumors can occasionally display features of several of those pathways.
Fig. 6. Sequence of mutational events that characterize the transition from normal colonic mucosa
to colonic adenocarcinoma first described by Vogelstein. In this model, the APC and KRAS gene
mutations are suggested to play a key role in the development of colorectal cancers (From Hasan et
al, 2010)
The following factors have been linked to the development of CRC:
Inflammation
Like for other types of cancer, inflammation has been suggested to play a role in the development
of CRC. Not only has epidemiologic observation identified inflammatory bowel disease (IBD,
including both ulcerative colitis and Crohn’s colitis) as an important risk factor for developing CRC
(Itzkowitz & Yio, 2004), also in other forms of sporadic as well as heritable CRC, inflammation is
likely to be involved (Terzic et al, 2010). Indeed, robust inflammatory infiltration and increased
expression of proinflammatory cytokines have been reported in colorectal tumors that are not
associated with clinically detectable IBD (Clevers, 2004; Terzic et al, 2010). The development of
colitis-associated cancer (CAC), the CRC subtype associated with IBD, displays many similarities
with other types of CRC although some different pathogenic sequences have been proposed
including chronic inflammation and injury-dysplasia carcinoma, which arises without the formation
of well-defined adenomas (Terzic et al, 2010). Nonetheless, the three main molecular pathways
involved in sporadic CRC have also been identified in CAC. The presence of chronic
inflammation however, appears to alter the timing and the frequency of these pathways (Hartnett
& Egan, 2012).
Chronic intestinal inflammation is characterized by dysfunction of multiple pathways, including
innate and regulatory functions of the immune response, epithelial-barrier function, signal
transduction, and stress response/DNA repair in response to persistent antigens derived from
food and the luminal bacteria (Westbrook et al, 2010). Considering the large number of pathways
disturbed, chronic inflammation has been proposed to affect the three stages of cancer: tumor
initiation, tumor promotion and tumor progression.
Tumor initiation, the process by which a normal cell becomes malignant, is associated with
accumulation of genetic alterations (Grivennikov et al, 2010; Westbrook et al,2010). Research
data indicate that inflammation can induce genetic alterations through several mechanisms.
Activated inflammatory cells (macrophages) for example trigger oxidant-generating enzymes
such as NADPH oxidase and myeloperoxidase to produce high concentrations of reactive oxygen
species (ROS) and reactive nitrogen species (RNS). While these ROS and RNS are important for
execution of physiological functions, excessive production can disturb the delicate balance
between ROS/RNS and antioxidant defense mechanisms inducing oxidative and nitrative base
damage as well as DNA single- and double-strand breaks (Coussens & Werb, 2002; Murata et al,
2012). Nonetheless, it is rather unlikely that ROS produced by immune cells diffuse and induce
mutations in adjacent epithelial cells. A more plausible hypothesis is that the cytokines and other
factors released by activated immune cells stimulate ROS production within epithelial cells.
− 36−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
In CAC, chronic inflammation precedes colitis-associated tumor development and therefore
oxidative damage to DNA, due to chronic inflammation, may be responsible for tumor initiation.
However, in sporadic CRC, it is rather unlikely that inflammation triggers tumor initiation because
most intratumoral immune cells are recruited after the tumor is formed. Consequently, chronic
inflammation does not precede but follows tumor development. After tumor formation however,
the localized inflammatory microenvironment can promote accumulation of additional mutations
and epigenetic changes (Terzic et al, 2010). Also during tumor promotion and progression,
cytokines released by activated immune cells can play a role by stimulating angiogenesis and
suppressing immune-mediated tumor elimination (Karin, 2006; Yu et al, 2009; Grivennikov et al,
2010).
Intestinal microbiota
Results of animal studies indicate that the intestinal microflora influences the development of both
sporadic CRC and CAC. In normal conditions, the intestinal microflora has important homeostatic
immune and metabolic functions, affects the proliferation and survival of epithelial cells and
provides protection against pathogens. Disruption of the homeostasis (both qualitatively and
quantitatively) of the intestinal microflora could promote cancer through different ways. In case
the number, diversity, and stability of commensal bacteria is altered, normal physiological
processes can be disturbed and trigger disease. Furthermore, pathogens (i.e. Bacteroides
fragilis) or conditional commensals can also contribute to tumorigenesis (Terzic et al, 2010).
Mechanisms might include induction of inflammation or production of mutagenic toxins. However,
a complex interplay between bacterial inflammation, toxin production and subsequent cellular
responses exists and complicates the understanding of the different mechanisms involved
(Collins et al, 2011).
Toll-like receptors
Toll-like receptors are single membrane-spanning, non-catalytic proteins which are mostly
expressed on intestinal epithelial cells, in addition to resident innate immune cells (RakoffNahoum & Medzhitov, 2008). Like other pattern recognition receptors they become activated by
components of bacteria and viruses, products of tissue damage, and necrosis, stress or other
signals (Terzic et al, 2010; Hartnett & Egan, 2012). Although Toll-like receptors might be involved
in the development of CRC, the overall contribution of pattern recognition receptors to epithelial
cells compared with immune or inflammatory cells remains still unclear (Terzic et al, 2010).
Several hypotheses underlying the link between the intake of red and processed red meat and
the increased risk of CRC have been proposed and the most important ones will be discussed. It
should be realized however that besides the compounds mentioned, other compounds may be
important and it was e.g recently reported that smoked meat products contained high
concentrations (up to 125 mg/kg wet weight) of formaldehyde, a recognized carcinogen (Zhu et
al, 2012).
2.2.6.1 Unlikely hypotheses: fat, protein and thermoresistant oncogenic bovine viruses
2.2.6.1.1 Excess of protein and fat intake
A diet high in red meat and/or in processed red meats potentially contains high levels of saturated
fat. High fat intake increases the secretion of secondary bile acids in the gut. These bile acids can
promote tumor formation by acting as aggressive surfactants for the mucosa thus increasing cell
loss and proliferation (Corpet, 2011). Furthermore, a high fat diet results in an increased amount
of free fatty acids in the colonic lumen. These free fatty acids may damage the colonic epithelium
and increase proliferation as discussed in more detail under 2.2.6.4.2. Finally, high fat diets favor
obesity, a status associated with CRC and other diseases. Meat is also a rich source of dietary
protein. Fermentation of the excess of proteins in the gut yields metabolites such as NH 3 and
H2S, compounds known to be toxic to the mucosa. However, neither an excess of fat nor protein
− 37−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
can explain the link between consumption of red and processed red meat and CRC since these
macro-nutrients are also present in dairy products, fish and poultry, foods not found to be
associated with CRC incidence in epidemiology. Furthermore, human epidemiologic studies do
not support an association between protein intake and CRC (Windey et al, 2012). Although
Padidar et al (2012) have shown in mice that susceptibility to azoxymethane (AOM)-induced
precancerous lesions is increased by high fat feeding, a meta-analysis, though subject to some
criticism, showed that nor animal fat nor animal protein are CRC risk factors (Alexander et al,
2009).
2.2.6.1.2 Thermoresistant oncogenic bovine viruses
An elegant hypothesis links red meat to CRC through “thermoresistant potentially oncogenic
bovine viruses” (zur Hausen, 2012). The hypothesis however is not based on experimental work
and does not explain a more outspoken cancer inducing effect of processed (cured) meats. The
latter indeed mainly consist of pig meat, rendering such hypothesis improbable though elegant.
2.2.6.2 Polycyclic aromatic hydrocarbons and heterocyclic amines
Polycyclic aromatic hydrocarbons (PAH) and heterocyclic amines (HCA) can be formed when
meat is cooked using high-temperature methods, such as pan frying or grilling directly over an
open flame. The amount of PAH and HCA produced depends on the cooking method, the
temperature used and the degree of doneness (Anderson et al, 2002). In animal studies, both
types of compounds have been shown to be carcinogenic through the induction of mutations.
However, before they can react with DNA, HCA and PAH require metabolic activation. The
compounds can also be detoxified and excreted, thus diminishing the degree of DNA damage
induced by them (Wang et al., 2012).
2.2.6.2.1 Polycyclic aromatic hydrocarbons
PAH are ubiquitous environmental toxicants produced by incomplete combustion of organic
compounds. They can be emitted during processing of coal, crude oil, petroleum, and natural
gas, as by-products of industrial production, from heating in power plants and homes (oil, gas,
charcoal-fired stoves, wood stoves), burning of refuse, wood fires, and from motor vehicle
exhausts. Humans are exposed to PAH through different routes since they enter the body by
consumption of contaminated foods or drinking water, inhalation of cigarette smoke, automobile
exhausts, and contaminated air from occupational settings (Alexander et al., 2008). For nonsmoking humans, the major routes of exposure to PAH are food and to some extent inhaled air.
In cigarette smokers, the contributions from smoking and food may be of a similar magnitude.
Food can be contaminated both with PAH from environmental sources and PAH formed during
food cooking. In case meat is grilled over a direct flame, fat/meat juices often drip onto the hot
fire, yielding flames containing a number of PAH which can adhere to the surface of the food.
However, PAH can also be produced during the curing and the processing of the food, for
example, when smoking is used as a preservation method (Cross & Sinha, 2004). The best
studied PAH is benzo[a]pyrene (BaP), recognized since 1987 as a probable human carcinogen,
and recently upgraded to Group 1 based on mechanistic and other relevant data by the
International Agency for Research on Cancer (IARC). In addition, three PAH have been
categorized as probably and twelve PAH as possibly carcinogenic to humans (IARC, 1993). PAH
are not genotoxic as such, but are activated after metabolisation. During the metabolisation
process of different PAH, reactive metabolites are formed which can covalently bind to DNA
(mainly to the guanine bases), inducing DNA damage. If the DNA damage is not or incorrectly
repaired, mutations can be induced.
Risk evaluation of long-term adverse health effects following dietary intake of PAH often
considers the total of up to 8 of these compounds. In Table 7, the 4 major structures often
considered together are presented (Alexander et al., 2008). Although PAH are mainly present in
− 38−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
meat and meat products, they are usually not considered as a specific causal agent for the
carcinogenic activity of meat and meat products as they are present in all foods as shown for a
recent Italian study in Table 8. In a limited clinical based case/control study (374 subjects) and
after correction for possible confounders, Sinha et al (2005) found that BaP intake was
associated with colorectal adenoma incidence. Dietary BaP intakes were derived from previously
established databases and from information on meat cooking methods and degrees of
doneness/browning obtained in preparation as collected from the literature and illustrated by
photography of the prepared meat (Augustsson et al, 1997) (Fig.7). Data should be available at
http://dceg.cancer.gov/tools/design/charred developed by the U.S. National Cancer Institute
(Sinha et al, 2005). The relation was stronger for BaP intake from all foods than for BaP from
meat with relative risk rates (highest vs lowest intake) of 5.60 and 2.82 respectively. Meat and
meat products represented 19 % of total dietary BaP intake. In line with earlier work, only
grilling/barbecuing (gas barbecue unit with ceramic briquettes) but not cooking increased PAH in
meat (Fig. 8) and the major source of meat associated BaP intake was grilled steak and
hamburger (69 %) whereas grilled chicken represented 23 %. In related work, Gunter et al.
(2005) confirmed their results and stated that “an incremental increase of 10 g of barbecued red
meat per day was associated with a 29% increased risk of large adenoma” specifying that the
barbecuing process involves exposure “to a naked flame”. In similar Australian work involving
1280 subjects however, a risk of CRC could not be associated with BaP intake (Tabatabaei et al.,
2010). The authors relate this contradiction to the possible differences in fat content of the meat
consumed. Also, in a recent case/control study, no relation was found between the urinary
concentration of a biomarker of PAH exposure and CRC incidence in women (Hofmann et al,
2013). Based on this information, it would seem that concern for PAH as a clear causal agent of
an increased risk of CRC through meat consumption should be limited to the “naked flame
contact” during the barbecue process.This information, as well as the simple but efficient method
to reduce exposure to PAH (and also HCA) by mechanical removal of charred and blackened
material from the surface of broiled meat and fish on the dish, can be easily communicated to the
consumers (Sugimura, 1997). It should be realized however that comparable levels of PAH (also
as environmental contaminant) are found in cereal products and in grilled poultry and fish, foods
not found to be associated with an increased risk for CRC.
Table 7. Some major carcinogenic polycyclic hydrocarbons (Alexander et al, 2008)
Common name
Chemical Structure
Abbreviation
Benz[a]anthracene
BaA
Benzo[b]fluoranthene
BbFA
Benzo[a]pyrene
BaP
Chrysene
CHR
− 39−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 8. Concentration means of BaP and PAH4 (BaA +BbFA + BaP + CHR) (ng/kg) in food groups
(From Cirillo et al, 2010)
BaP
PAH4
Milk
60
870
Cereal based foods
270 – 720
980 – 1980
Fish and Fish products
580
2220
Dairy products
130
600
Fresh and cooked
vegetables
180
2390
Meat and meat products
580
3970
Fig. 7. Method used to estimate intake of mutagens (Sinha et al, 2005).
− 40−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig. 8. BaP content of hamburger and steak cooked by different methods to varying degrees
of doneness (from Kazerouni et al, 2001).
2.2.6.2.2 Heterocyclic Amines
The formation and final concentration of heterocyclic amines (HCA) formed in heated meat and
fish via the Maillard reaction with creati(ni)ne, amino acids, and sugars depend on many factors
including cooking method, cooking time and temperature, the concentration of precursors, and
presence of water and fat in the raw product. More than 25 HCA have been isolated from different
cooked muscle foods and IARC (1993) categorized eight of them [including 2-Amino-3,4dimethylimidazo[4,5-f]quinoline (MeIQ), 2-Amino-3,8-dimethyl imidazo[4,5-f]quinoxaline (MeIQx)
and 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine (PhIP)] as possibly carcinogenic to
humans and 2-Amino-3-methylimidazo[4,5-f]quinoline (IQ) as a probable human carcinogen (Fig.
9). The nitrenium ion formed during metabolization is considered the likely ultimate genotoxic
compound binding to the DNA bases producing DNA adducts through the formation of N-C bonds
at guanine bases (Jägerstad & Skog, 2005; Goldman & Shields, 2003). The most abundant HCA
in cooked meat are PhIP and MeIQx. They are also the two major absorbed HCA after intake of a
cooked meat meal (Cross & Sinha, 2004). Table 9 gives some indication on the effects of type of
cooking on HCA levels. These results indicate that levels of MeIQx and PhIP, two HCA
considered most relevant in relation to the risk for CRC, are similar if not lower in beef and pork
compared to those found in cooked poultry and fish. For both poultry and fish, epidemiology did
not show an association with CRC risk. By the same token, Viegas et al (2012) demonstrated that
whereas quantitative HCA and PAH profiles were different for barbecued beef and salmon using
the same type of charcoal, higher levels of HCA and PAH were found in salmon samples.
Nevertheless, several studies provide some evidence for a positive association of well-done meat
intake and HCA exposure with the risk of CRC. In a German EPIC observational study involving
25540 participants followed between 1998 and 2007, dietary HCA (PhIP but not MeIQx) were
found to be significantly associated with the CRC incidence (relative risk: 1.47, highest vs lowest
intake), even after adjustment for total red and processed red meat consumption. This suggests a
− 41−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
specific effect of PhIP that cannot be completely explained by other components in red or
processed red meat (Rohrmann et al, 2009). In a somewhat smaller US scale case-control study
involving 6307 subjects between 2003 and 2010 (Fu et al, 2011), a significant positive association
was found between exposures to all meat-derived HCA studied and risk of colorectal polyps,
again after adjusting for potential confounders (relative risk: 1.3 – 1.4, highest vs lowest intake).
As described above for PAH, HCA intake levels were derived in both studies from information on
cooking methods and the degree of doneness/browning obtained in preparation as collected from
the literature and illustrated by photography of the prepared meat (Sinha et al, 2005). For EPIC,
similar data are available in relation to cooking method at European Prospective Investigation into
Cancer and Nutrition (EPIC) (2012a) and photographs illustrating “meat doneness” were
developed for the European environment by e.g. Augustsson et al. (1997). It is clear that the latter
concept is evaluated differently as illustrated e.g. by the range of HCA intake in the US and
German observations (Table 10). Furthermore, Deziel et al. (2012) demonstrated that estimates
for dietary HCA exposure obtained from food frequency questionnaire (FFQ) collections, diary
collections, and measurements of urinary PhIP were not related. More consistent cancer risk
estimates of dietary HCA exposure may therefore require improved HCA assessment tools.
Results from animal experiments do not fully explain the role of HCA in the increased risk of CRC
related to consumption of red and processed red meat either, as the well-known carcinogenic
effects of HCA have been demonstrated in rodents, at levels more than 1000 times higher than
HCA levels found in foods. For these reasons, HCA are generally not considered very important
in relation to the carcinogenic properties of meat (Corpet, 2011a). Furthermore, as HCA require
metabolic activation to function as mutagens/carcinogens, the carcinogenic potential of HCA may
depend on the extent of metabolisation (Cross & Sinha, 2004). Cancer risk posed by dietary HCA
was indeed shown to vary with genetic differences in the drug metabolizing enzymes involved
e.g. in acetylation and sulfonation (Fig. 3) (Le Marchand et al, 2002; Zheng& Lee, 2009).
Besides genetic factors, evidence is available that individual differences in the intestinal micro
flora may affect HCA carcinogenic activity (Vanhaecke et al., 2008). In a comprehensive review
Alaejos et al. (2008) therefore conclude that there is no sufficient scientific evidence to definitely
accept that dietary HCA intake specifically causes cancer but that “Epidemiological evidence
points to genetic predisposition as the main factor in meat associated HCA related cancer
development”.
The evidence listed above clearly indicates that both HCA and PAH intake is determined by the
meat-cooking technique and doneness level. Although both types of compounds may not be the
major causative agent for the CRC inducing effect of red and processed red meats, the
formulation of guidelines for meat cooking could be considered appropriate. For industrially
cooked meat products, a decrease of HCA content could be aimed at using processing variables
that minimize HCA production as determined e.g. by Dundar et al. (2012). In this respect, the
finding that the ripening time of meat affects HCA formation during heating (Szterk et al., 2012)
may also be relevant. People involved in meat preparation in restaurants and catering should also
consider such information as it has been shown that cooks are potentially exposed to relatively
high levels of airborne HCA (Thiébaud et al, 1995). For household cooking, an efficient method to
reduce exposure to PAH and HCA consists of the mechanical removal of charred and blackened
material from the surface of broiled meat and fish on the dish (Sugimura, 1997). Furthermore,
discouragement of “well done meat” should be considered and longer time/lower temperature
treatments should be encouraged.
− 42−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig. 9. Structures of heterocyclic amines categorized by the International Agency for Research on
Cancer (1993) as possible (IQ, MeIQ and MeIQx) or probable human carcinogen (PhIP) (From
Murkovic, 2004)
Quinolines: IQ 2-Amino-3-methylimidazo[4,5-f]quinoline ; MeIQ 2-Amino-3,4-dimethylimidazo[4,5f]quinoline
Quinoxaline: MeIQx 2-Amino-3,8-dimethylimidazo[4,5-f]quinoxaline
Pyridines: PhIP 2-Amino-1-methyl-6-phenylimidazo[4,5-b]pyridine
− 43−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 9. Heterocyclic amine contents of cooked meat and fish (Puangsombat et al., 2012)
Heterocyclic amines in meat (ng/g)
Cooking methoda
Beef
MEIQx
PhIP
Total
Fried
medium rare
well done
1.75
3.33
0.94
5.27
2.73
8.92
Broiled
medium rare
well done
Baked
0.08
0.12
0.33
1.58
5.63
1.49
1.72
6.04
2.34
Pork
Fried
Baked
2.39
0.23
9.20
2.20
13.91
3.29
Poultry breast
+ skin
- skin
Fried
0.23 (0.31)b
0.46
2.61 (2.72)
6.06
2.89 (3.13)
7.06
Fish
Baked
Fried
1.27-2.95
2.31-3.11
4.40-5.67
9.11-10.89
7.85-8.70
13.09-16.29
a
Frying = in a Teflon-coated frying pan without adding oil at a surface temperature of 204 °C. Meat was
fried, turned once, and removed from the pan when the desired temperature was reached.
Broiling = Oven (convection, top and bottom heat) was preheated to 232 °C (monitored with oven
thermometer). The meat was placed on a broiler pan to keep the broiled beef out of the drippings. The
meat was removed when a final internal temperature (51° C medium rare - 71 ° C well done ) was achieved
Baking : Oven (convection, top and bottom heat) was preheated to 177 °C (monitored with oven
thermometer). The meat was placed on a baking pan. The meat was removed when a final internal
b
temperature was achieved. () = in meat and skin
Table 10. HCA intake in German and US observational studies
1
HCA intake (ng/d)
Rohrmann et al (2009)
Fu et al (2011)
PhIP
< 6.5 - >41.4
< 73.3 - >339.4
MeIQx
<3.8 ->19.9
<12.2 - >70.1
1
Levels of lowest - highest quartiles
2.2.6.3 Nitrosamines and other N-Nitroso compounds
The general term ‘N-nitroso compounds’ (NOCs) covers all substances with N-nitroso groups,
including N-nitrosamines and N-nitrosamides. Twenty years ago Tricker and Preussmann (1991)
referred to established carcinogenic activities of over 300 NOCs in one or more animal species
including higher primates. Since NOCs are alkylating agents that can react with the DNA of the
target tissue, they can induce mutations and therefore could potentially initiate carcinogenesis.
Alkylation of the O6-position of guanine by NOCs may lead to G → A transitions (Saffhill et al.,
1985) a common mutation in CRC found in codons 12 or 13 of ki-Ras (Bos, 1989). Nnitrosamides spontaneously form alkylating agents, and thus are more likely to cause damage at
the site of exposure. In contrast, N-nitrosamines require metabolic activation to be mutagenic and
− 44−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
have thus the potential to cause damage at any activation site (Jägerstad & Skog, 2005; Cross &
Sinha, 2004).
During food consumption, humans can be exposed to NOCs both of exogenous and endogenous
origin.
2.2.6.3.1 Exposure by exogenous routes
As recognized e.g. by Hebels et al (2012), meat products, and especially processed or heattreated foods, often contain pre-formed NOCs. NOCs have for example been detected in foods
processed by smoking or direct fire-drying. When these production processes are performed at
high temperature, molecular nitrogen can be oxidized forming nitrogen oxides, compounds able
to nitrosate amines present in foods such as meat. NOCs can also be formed in meats containing
nitrite. Nitrite is the common additive used in meat processing (meat curing) as an anti-bacterial
agent, specifically active against Clostridium botulinum, and/or to produce the characteristic redpink color of cured meats originating from its reaction with myoglobin. In acidic conditions such as
those often found in food processing operations, nitrite can be transformed to dinitrogen-, tri- or
tetraoxides which are all potent nitrosating agents (Cross & Sinha, 2004). In case a nitrosonium
ion NO+ is added to an amine -NH2 and nitrosamines are formed (nitrosation):
NO2- + 2 H+ → NO+ + H2O and R2NH + NO+ → R2N-NO + H+
The nitrosyl ion NO− on the other hand can be added to a metal (e.g. iron) or a thiol, leading to
nitrosyl iron Fe-NO (e.g., in nitrosylated heme = nitrosylheme) or S-nitrosothiols (RSNOs)
(nitrosylation). The complex reactions characterizing meat curing are discussed in more detail
under 2.2.6.6.
An important group of NOCs in food are the volatile N-nitrosoamines including Nnitrosodimethylamine (NDMA) and N-nitrosodiethylamine (NDEA), two compounds classified by
IARC as probably carcinogenic to humans, and N-nitrosopyrrolidine (NPYR), N- nitrosopiperidine
(NPIP), and N-nitrosodibutylamine (NDBA) which are considered as possible human carcinogens
(International Agency for Research on Cancer, 1978; Jägerstad & Skog ,2005). Tricker (1997)
estimated that dietary sources accounted for about 70% of exogenous human exposure to Nnitrosamines, the rest being due to occupational exposure (20%), smoking (2%) and various
sources (8%). The data assembled in Table 11 illustrate that processed and heated meats (e.g.
heated bacon) are indeed major dietary sources of these volatile NOCs but dairy products, fish
and products such as spices may also be important contributors. Despite the fact that most
information is available on volatile nitrosamines, the main forms of NOCs occurring in food are
non-volatile NOC including for example N-nitrosoproline. Non-volatile NOCs have not been
reported as mutagenic or carcinogenic, but they might act as precursors to volatile carcinogenic
nitrosamines (Jägerstad & Skog, 2005).
Although it has been clearly demonstrated that levels of volatile nitrosamines in a cured meat
model increase with temperature and amounts of nitrite added during processing, they stay < 10
µg/kg as long as the nitrite level of 120 mg/kg was not surpassed (Drabik-Markiewicz et al, 2009).
This observation justifies strict regulations on the use of nitrite in meat processing as well as the
often used addition of ascorbate to food in order to reduce N-nitroso reactions. Indeed, according
to Skibsted (2011), the addition of 500 mg/kg of sodium ascorbate or erythorbate (isoascorbate)
to meat selected for good reducing capacity and appropriate low pH from non-stressed animals
may prevent formation of potentially carcinogenic N-nitroso compounds as ascorbate reacts
faster than secondary amines with the nitrosating agent N2O3. Furthermore, ascorbate in batters
reduces the toxin production by proteolytic clostridium botulinum types A and B together with
nitrite and salt (Honikel, 2008).
A striking finding is the possible presence of NDMA in fresh and minced meat (European
Prospective Investigation into Cancer and Nutrition,2012a). As almost no amines are present in
− 45−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
fresh meat and its nitrite concentration is rather low, formation of nitrosamines in fresh meat has
indeed been considered to be rather unlikely (Honikel, 2008). Nevertheless, values of NDMA up
to 14 µg/kg have been reported for bulls but were shown to originate from contamination in meat
production systems (Rywotycki, 2003). Heating of such meat (muton) further increases the levels
of nitrosamines, mainly present in the fat, increasing rapidly in range from 40 to 100°C and then
staying stable, indicating that formation takes place in temperatures below 100°C (Fig.10). In line
with established carcinogenic activities, a significant positive association was observed between
intake of NDMA and subsequent occurrence of CRC in a large scale Finnish study (Knekt et al,
1999). However, within the various sources of NOCs, intake of smoked and salted fish was
significantly and intake of cured meat was non-significantly associated with risk of CRC.
Table 11. Levels of Nitrosamines in foods
Nitrosamines
Foods
Ref. (1)
N-Nitrosodimethylamine
(NDMA)
N-Nitrosodiethylamine (NDEA)
Meat
Cured meats
Fried Bacon
Frankfurt
Dried Fish (Japan)
Dairy products
Cheese
Non fat milk
Ref. (3)
0 - 4.0
1.0 - 5.0
4.0
4.5
3.0 - 38.0
1.0 - 6.0
1.9
0 - 84
0.5 - 5.0
0 - 4.5
Cured meats
Ham
< 2.4
Cured meats
Smoked chicken
Bacon
1.0 - 56.0
< 5.3
N-Nitrosopyrrolydine (NPYR)
Cured meats
Fried bacon
Mixed spices
1.0 - 5.0
< 130.0
< 10.0
N-Nitrosopiperidine (NPIP)
Cured meats
Fried bacon
< 20.0
< 9.2
N-Nitrosodibutylamine (NDBA)
µg/kg
Ref. (2)
1.5
13.6
Ref. (1) Tricker & Preussmann (1991)
Ref. (2) Stuff et al (2008)
Ref. (3) Jakszyn et al., (2004); European Prospective Investigation into Cancer and Nutrition (2012a)
− 46−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig. 10. Influence of frying temperature on the content of volatile nitrosamines in mutton
(Yurchenko & Mölder, 2007)
NDMA=N-nitrosodimethylamine
NPYR = N-nitrosopyrrolidine
NPIP = N- nitrosopiperidine
NDEA = N-nitrosodiethylamine
NDB = N-nitrosodibutylamine
2.2.6.3.2 Endogenous production of NOCs
About 45-75% of the total NOC exposure is estimated to result from endogenous production
(Tricker, 1997). Besides secondary amines, other nitrosatable precursors present in food are
essential nutrients such as proteins and trace compounds including urea derivatives (de Kok &
van Maanen, 2000). Endogenous formation of NOCs may occur through several mechanisms
including acid catalyzed, bacterial or colon cell-mediated pathways (Cross & Sinha, 2004).
Acid catalyzed endogenous NOC formation is considered to occur mainly in the stomach and the
nitrosating agent, nitrous acid, may be derived from the considerable intake of nitrate, mainly with
vegetables. About 5% of the exogenous nitrate is absorbed in the small intestine, recirculated into
the saliva and reduced to nitrite by oral bacteria. In the acidic environment of the stomach, the
salivary nitrite is transformed into the nitrosating agent. In conditions where the pH is too high for
nitrous acid mediated nitrosation, NOC formation may result from biological catalysis by bacterial
growth (de Kok & van Maanen, 2000). Considering the neutral pH of the bowel, the bacteria
mediated NOC formation is most likely. The involvement of the colonic flora in the NOC formation
was supported by the observation that in germ free rats, nitrate did not stimulate endogenous
ATNC formation (Massey et al, 1988). However, little is known regarding the bacterial species
involved in endogenous nitrosation and different bacterial enzymes responsible for the nitrosation
reaction have been described. A recent study in a pig cecum model indicated that intestinal
formation of NOCs depends on the intake of nitrate and the capacity of the microbiota to reduce
nitrate into nitrite (Engemann et al, 2013). In the colon cell-mediated catalysis, nitric oxide formed
via the inducible form of NO synthase appears to act as the nitrosating species. Nitrosation of
amines by activated macrophages has been reported (de Kok en van Maanen, 2000) and may
thus occur at sites of (low-grade) inflammation. As discussed in more detail under 2.2.6.4.1.,
heme present in red and processed red meat has been suggested to stimulate endogenous
production of NOCs.
− 47−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.6.4 Heme
Evidence from both epidemiologic and experimental studies suggests that heme plays a crucial
role in the link between the risk of CRC and red and processed red meat intake. Heme consist of
an iron atom contained in the center of a large heterocyclic organic ring called a porphyrin
(Santarelli et al, 2008). It is associated with globin polypeptides, similar but different between
hemoglobin, the blood oxygen carrier and myoglobin, the muscle oxygen carrier. In red meat,
heme is present in high concentrations in the form of myoglobin, resulting in the red color. Due to
the nitrate and nitrite present in the curing salt, heme iron occurs in its nitrosylated form in
processed red meat (Bastide et al, 2011). Four large prospective studies found that a high intake
of heme iron was associated with a higher risk of CRC (Lee et al, 2004; Larsson et al, 2005;
Cross et al, 2010; Ferruci et al, 2012), a finding confirmed by a recent meta-analysis also
reporting a significant inverse dose-response association of zinc intake with risk of CRC (Qiao et
al, 2013). No evidence for an association with intake of heme iron was obtained in two other
studies (Kabat et al, 2007; Zhang et al, 2011). Estimation of heme-iron from food intake is
however difficult and subject to error as the proportion of heme-iron in total Fe decreases with
aging in beef (Ramos et al, 2012) and with heat treatment (D’evoli et al, 2009; Purchas et al,
2004; Lombardi- Boccia et al, 2002) (Table 12).
An association with a polymorphism of heme-oxygenase-1 was not found in a limited case/control
study in Denmark, suggesting that heme from meat is not important in CRC development
(Andersen et al, 2011). In a recent study involving 185 archival CRC samples collected from
participants of the European prospective Investigation into Cancer (EPIC)-Norfolk study, Gay et
al. (2012) found that CRC cases associated with APC gene aberrations consumed higher levels
of processed red meat and iron from red meat and red meat products. A perhaps striking finding
is the absence of an association between heme iron intakes and CRC risk in Japanese men or
women as reported from a large population based prospective study (Hara et al, 2012). However,
lower intakes and different major food sources of heme iron may explain the lack of association.
Indeed, fish was the main food source of heme iron in the study, whereas maximal daily intakes
of fish and red meat were 123 and 86 g respectively.
As discussed by Corpet (2011), animal studies published before 2004 did not show red meat
promotion of CRC because of the high calcium content of experimental diets, known to suppress
heme induced colon carcinogenesis (Sesink et al, 2001). In a series of later experiments on low
calcium diets however the research group of Fabrice Pierre (Toulouse, FR) linked red meat
consumption to the development of aberrant crypt foci (ACF) and mucin-depleted foci (MDF),
precancerous lesions, in the colon of azoxymethane sensitized rats. The development of
precancerous lesions was shown to be related to red meat intake in a dose-response manner and
the effect was mimicked by heme (Pierre et al, 2004). It should be noted that very large amounts
of “freeze dried beef “, chicken or “black pudding” were included into the experimental diets (600
g/kg). Later, the same research group demonstrated that also processed red meat products
promote colon carcinogenesis in a rodent animal model (Santarelli et al, 2010).
Three mechanistic hypotheses have been proposed underlying the promotion of CRC by heme:
(1) the catalytic effect of heme iron on the endogenous formation of NOC, (2) the catalytic effect
of heme iron on the formation of lipid oxidation endpoints (Bastide et al, 2011) and (3) the
metabolization of heme in the gut into a cytotoxic and promoting factor (Sesink et al, 1999).
− 48−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 12. Total iron and heme iron (mg/100 g) in raw and cooked meats (from Lombardi-Boccia et al,
2002)
Raw
Cooked
Total Fe
Heme Fe (a)
Total Fe
Heme Fe (b)
(b)/(a)
Chicken
Breast
Thigh
0.40
0.70
0.12 (30)a
0.20 (28)
0.58
1.34
0.16 (28)
0.30 (22)
0.93
0.78
Turkey
Breast
Thigh
0.50
0.99
0.14 (28)
0.49 (49)
0.79
1.46
0.21 (26)
0.57 (39)
0.92
0.79
Pork
Loin
chop
0.36
0.49
0.20 (55)
0.32 (65)
0.46
0.79
0.21 (46)
0.56 (71)
0.83
1.09
Rabbit
0.45
0.25 (55)
0.60
0.31 (52)
0.94
Veal filet
0.85
0.71 (83)
1.58
1.33 (84)
1.01
Lamb chop
2.23
1.68 (75)
3.20
2.25 (70)
0.93
Horse fillet
2.21
1.75 (78)
3.03
2.16 (71)
0.91
Beef
Fillet
Roast beef
2.35
2.04
2.11 (90)
1.77 (87)
3.88
3.74
2.86 (74)
3.14 (84)
0.82
0.96
a
as % of total Fe
2.2.6.4.1 Effect of Heme on the endogenous production of NOC
In a series of human intervention studies, the research group of the late Sheila Bingham
(Cambridge, UK) related the extensive fecal excretion of endogenously produced NOCs to red
meat and processed red meat consumption. They demonstrated a dose-response increase in
fecal excretion of NOCs with red meat intake, not observed with vegetable proteins, white meat or
an Fe2+ supplement but clearly mimicked by a heme supplement (Table 13). Also in animal
studies, inclusion of red or processed red meat into the diet increased the fecal concentration of
ATNC (Parnaud et al, 2000)(Mirvish et al, 2003). However, the analytical method used to analyze
NOCs did not differentiate between N-nitrosamines and other compounds such as S-nitrosothiols,
O-nitroso compounds and nitrosyl iron. As discussed previously, certain N-nitroso species such
as most of the N-nitrosamines, are known to be profoundly tumorogenic through the formation of
DNA adducts, whereas such activity has not been reported for iron nitrosyls and S-nitrosothiols,
compounds that are continuously formed in biological systems through the action of nitric oxide
synthase (Hogg, 2007). Given the lack of specificity of the technique, the term ATNC (apparent
total N-nitroso compounds) was used to describe the substances measured by this technique.
Several hypotheses have been put forward to explain the effect of heme and heme-containing
meat products on the fecal ATNC content. First, the increased fecal ATNC content may be
related to heme-induced changes in microbiota. In a recent study, dietary heme changed the
microbiota with a major increase in the ratio of Gram-negative to Gram-positive bacteria.
(IJssennager et al, 2012b). However, the selective shift to gram-negative bacteria was not
− 49−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
accompanied by a functional change in the mucosal sensing of the bacteria, thereby giving no
support for the suggested role of microbial pathogens in colorectal carcinogenesis (Collins et al.,
2011)(Jeffery & O'Toole, 2013). Recently however, it was suggested that alteration of the
irontrophic luminal bacterial population by dietary heme may be associated with red meat induced
CRC risk (Kato et al, 2013). Also, microbiota are mainly active in the colon whereas fecal ATNC
content was comparable between healthy and ileostomized volunteers (Lunn et al, 2007),
indicating endogenous formation of NOC after red meat intake occurs in the small intestine. By
using an improved analysis technique, the research group was also able to show that nitrosyl
heme and nitrosothiols are major constituents of both fecal and ileal ATNC (Kühnle et al, 2007).
According to their hypothesis, acid-catalyzed thionitrosation in the stomach is the initial step in the
endogenous formation of NOCs. Under the alkaline and reductive conditions of the small and
large bowel, NO can be released from S-nitrosothiols to be taken up by heme.
Both nitrosyl heme and S-nitrosothiols can act as nitrosating agents, promoting the formation of
potentially carcinogenic NOCs in the gut epithelium. However, S-nitrosothiols and iron nitrosyls
may also act as a protective mechanism by capturing NO thereby limiting the formation of DNA
alkylating agents and facilitating excretion (Hogg, 2007). Further investigation towards the relative
role of the different ATNC involved and the origin and regulation of the NO supply is thus
required.
1
Table 13. Fecal excretion of total apparent N-nitroso compounds (ATNC) and red meat intake .
Meat consumed (g/d)
Fecal ATNC
ng/g
µg/d
Red meata
240
None
0
60
444 + 60
54 + 7
347 + 61
52 + 11
1516 + 414*
159 + 33*
420-600
White meatb
420-640
2104 + 1524*
249 + 167*
759 + 528
87 + 55
Meat and supplements consumed (/d)
60 g Red meat
Fecal ATNC
ng/g
µg/d
766 + 233
77 + 9
60 g Red meat + hemec
1438 + 345**
157 + 23**
60 g Red meat + Fe2+
d
852 + 393
61 + 10
1
Adapted from Steinberg (2009) using data (mean values + SD) from Hughes et al (2001), Bingham et al
a
(2002) and Cross et al (2003) 0-100 g roast beef at lunch, 0-320 g beef (lasagne or steak) or pork (sweet
b
c
and sour pork) at dinner Chicken, turkey or white cod 7.8-mg heme iron, as 50-gram liver pate and 70d
gram blood sausage, to match the iron content of the 420-gram red meat diet (17.7 mg/day) A daily 300mg ferrous gluconate tablet (35 mg of ferrous iron) supplement * significant differences with values of no
meat or white meat ** significant differences with other groups
Carcinogenicity of ATNC
Despite the data from human intervention and animal studies showing an increase in ATNC after
the consumption of red or processed red meat, the carcinogenicity of ATNC formed in the gut
remains unknown. Fecal colon cells containing an O6-methylguanine DNA adduct, a
characteristic promutagenic and toxic adduct formed by many NOCs, have been numbered and
found to be significantly related to fecal excretion of ATNC in the stool of volunteers consuming
meat in various diets as shown in Fig. 11 (Lewin et al, 2006). Furthermore, the mutations induced
by diazoacetate, nitrosated glycine, in a yeast functional assay, are very similar to those observed
in colorectal tumors, suggesting that NOCs may be involved in CRC (Gottschalg et al, 2007).
However, in the dietary intervention studies of Bingham’s group (Cross et al, 2006; Joosen et al,
− 50−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2009 & 2010), no difference in fecal water genotoxicity in relation to meat intake was detected
despite the increased fecal ATNC concentrations. Both masking of the genotoxic effect by
genoprotective compounds present in the complex mixture of the fecal water and the inability of
the used Comet assay in human-derived colonocyte cell lines to detect genotoxic chemicals in
fecal water have been suggested in order to explain this unexpected result (Gratz et al, 2011). In
contrast, a red-meat intake-induced increase in fecal water genotoxicity which was not related to
fecal ATNC content nor influenced by inflammation of the colon was observed in patients
suffering from intestinal inflammation as compared to inflammatory bowel disease (Hebels et al,
2011). Based on these results, the authors suggested that the increased genotoxicity is linked to
heme-catalyzed oxidative stress rather than to heme-stimulated NOC formation.
Fig. 11. Correlation between fecal total ATNC concentration and percent cells staining positive for
the O6-methylguanine DNA adduct in exfoliated colonic cells isolated from fecal extracts (n = 55)
(from Lewin et al, 2006).
In 2011, a large prospective study investigating the relation between dietary NOCs and the risk
for cancer was performed (Loh, 2011). Exposure to endogenous NOCs was estimated based on
the estimated iron content from meat intake considering the relationship between the fecal ATNC
and iron intake observed in several human controlled-diet studies (discussed above). Dietary
NDMA intake (ng/d) was calculated using a food database of potential carcinogens (European
Prospective Investigation into Cancer and Nutrition, 2012a). Whereas dietary NDMA intake was
associated with a higher incidence of rectal cancer, this association could not be found neither for
endogenous NOC exposure nor for dietary nitrite. Large errors associated with the various
estimates calculated can explain the lack of a relationship between endogenous NOC exposure
and rectal cancer. Furthermore, it cannot be excluded that although the study confirms the
previously reported carcinogenic activity of exogenous exposure to NDMA, other food sources
than red and processed red meats may be involved.
2.2.6.4.2 Effect of Heme on the oxidation of polyunsaturated fats
In rats, carcinogenesis promotion by dietary heme was found to be associated with the urinary
excretion of 1,4-dihydroxynonane mercapturic acid (DHN-MA), a fat peroxidation biomarker
(Pierre et al, 2004). An increase in this biomarker was also observed in the urine of volunteers
given black pudding, a heme loaded blood sausage (Pierre et al, 2006), suggesting that the
consumption of red and processed red meat stimulates the fat peroxidation pathway. During lipid
peroxidation, polyunsaturated fatty acids derived from the phospholipids within the intestinal
contents and/or colonocyte cells are oxidized by ROS and RNS. Due to abstraction of a hydrogen
− 51−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
atom from the fatty acid carbon chain, a carbon radical is formed that tends to be stabilized by
production of a conjugated diene. The latter rapidly reacts with 02 to give a hydroperoxy radical
that oxidizes other lipid molecules and continues the chain reaction of lipid peroxidation. Lipid
peroxides are further degraded generating reactive aldehydes of three to nine carbons in length
unsaturated in alpha, beta- positions which are relatively stable and can diffuse throughout the
cell (Halliwell & Gutteridge, 1984; Bartsch & Lair, 2004)(Fig. 12).
Reactive aldehydes, among which malondialdehyde (MDA) and 4-hydroxynonenal (4-HNE) are
the two most important ones, can either interact directly with DNA and proteins, or undergo
further oxidation to more reactive epoxy derivatives (Fig.12). MDA forms adducts with DNA, such
as the 1,N2-malondialdehyde-deoxyguanosine adduct and increased levels of this adduct have
been found in cells of colorectal biopsies from adenoma patients compared with adenoma-free
subjects (Leuratti et al, 2002). 4-HNE has weak mutagenic activity but induces apoptosis killing of
normal but not precancerous cells, possibly explaining tumor promotion by a selection process
(Baradat et al, 2011).
Heme has been demonstrated to catalyze lipid (per)oxidation in several conditions including
digestion as well as processing of food. MDA levels in human plasma increase following meat
consumption (Gorelik et al, 2013). A meat dietary pattern was found to be significantly associated
with increased plasma levels of F-2 isoprostanes, compounds produced by the free radicalcatalyzed peroxidation of arachidonic acid and considered to be the most reliable marker of
oxidative damage (Meyer et al, 2013). In a simulated gastric compartment (Lorrain et al, 2010)
and in the rat stomach (Kanner et al, 2012), heme compounds such as myoglobin or
metmyoglobin were found to accelerate further degradation of lipid peroxides, either ingested with
the diet or formed in the stomach (Kanner, 2007). The resulting aldehydes, considered as
ultimate mediators of toxic effects, may be transported to the intestines and then incorporated into
the body (Kanazawa & Ashida, 1998).
An analogous myoglobin-induced oxidation/peroxidation of polyunsaturated fatty acids during the
conversion of muscle to meat is also widely recognized but the very complex mechanisms
involved are a matter of dispute (Baron & Andersen, 2002; Carlsen et al, 2005). An elegant model
proposed by Faustman et al (2010) involves mutual activation of both membrane lipid and
myoglobin oxidation (Fig. 13). Possible mechanisms have been classified into four types
changing in relative importance of prooxidative capacity with low pH, high prevalence of
deoxygenated heme pigment, oxidative modification of the heme pigments and proteolysis. Nitric
oxide modifies and in most cases moderates the prooxidative activity of the heme pigments
(Carlsen et al, 2005) as will be discussed more under 2.2.6.6.
The link of lipid peroxidation with heme in relation to CRC has been further supported by the
observation that hemoglobin treatment promoted DNA damage induced by linoleic acid
hydroperoxide derived compounds in colon adenocarcinoma cells (Angeli et al., 2011). In a more
general context, lipid hydroperoxides of dietary origin have been identified as an important driving
force for liver carcinogenesis (Rohr-Udilova et al, 2008) whereas unsaturated fatty acid oxidation
contributes to the inflammatory response (review in Marnett, 2012), a condition associated with
CRC (Tudek & Speina, 2012).
Cholesterol oxides
It is striking that little attention has been given to cholesterol oxides, oxidation products of
cholesterol grouping about 70-80 different compounds. Some have been linked to colon
carcinogenesis producing a specific pro-apoptotic effect on human colon cancer cells and
presenting possibilities for new insights on strategies in anticancer therapy (Biasi et al, 2012). A
number of those were shown to be produced in processed red meats be it at very low levels
(Chizzolini et al, 1999; Zanardi et al, 2004).
− 52−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig.12. Summary of intermediate and end product formation during peroxidation of polyunsaturated
fatty acids (from Marnett & Plastaras, 2001 and Marnett, 2012)
peroxylradicalshydroperoxides
lipoxidative reactive carbonyl species detected in biological systems.
− 53−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig.13. Model for mutual activation of membrane phospholipid and myoglobin oxidation in meat
(from Faustman et al, 2010).
2.2.6.4.3 Metabolization of heme in the gut into a cytotoxic and promoting factor
A third possible explanation for the role of heme in the increased risk for CRC involves a direct
effect of heme on colonic cells and was formulated by the research group of Vandermeer. They
showed that addition of hemin (a chemical derivative of myoglobin formed by removal of the
protein part of the molecule, oxidation of the iron atom, and combination with an acid to form a
salt (see further Fig. 14)) to a low-calcium diet in rats increased epithelial proliferation in the
colonic mucosa and induced cytotoxicity of fecal water. Hyperproliferation was considered as a
compensation for cytotoxicity (Sesink et al, 1999). Furthermore, hemin-fed rats excreted much
less host DNA in feces compared to controls, suggesting that hemin decreased cell differentiation
and exfoliation of colonocytes in the gut lumen (Van Lieshout et al, 2004). Recently, the research
group investigated the role of the PPARα, a nuclear hormone receptor known to protect against
oxidative stress and lipid peroxidation, in heme-induced hyperproliferation and hyperplasia. Since
the five investigated PPARα target genes did not respond to heme, they concluded that probably
not ROS-induced stress but cytotoxicity-induced stress initiates colonic hyperproliferation
(IJssennagger et al, 2012). This hypothesis was further supported by the later observation that
not ROS production but luminal cytotoxicity coincided the changes in crypt signaling and
hyperproliferation in heme-fed mice (IJssennagger et al, 2013). However, it is not clear in all
these studies, whether hemin or food heme was used. Furthermore, the speculated heme-based
cytotoxic factor has not yet been identified (Santarelli et al, 2008).
− 54−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.6.5 The “white meat” controversy
Accepting heme as the major responsible carcinogenic compound in red meat (mainly beef and
pork) to explain the increased incidence in CRC appears to be subject to some doubt. Indeed, it
has been reported that heme contents of chicken and pork are of similar magnitude and both
lower than beef (Table 12). Red meat is a culinary term indicating meat which is red when raw,
and not white when cooked. It includes the meat of most adult mammals and some fowl (e.g.
ducks). In a more precise manner, the terminology “red” and “white” reflects the relative
proportion of red and white muscle fibers known to be more in favor of white fibers in pigs than in
beef. This finding is reflected in pig meat iron contents which are more similar to poultry than to
beef as e.g. also reported in Belgian nutrition advice (De Geeter, 2009). It also lead to the U.S.
National Pork Board advertising campaign positioning pork as "the other white meat”, a slogan
retired in 2011 (see e.g.http://en.wikipedia.org/wiki/White_meat) as pork is clearly considered as
red meat by the USDA (http://askkaren.custhelp.com/app/answers/detail/a_id/1357/~/is-porkwhite-meat%3F)
Red meat has been defined as meat derived from cattle (including calves), sheep (including
lamb) and pigs (European Prospective Investigation into Cancer and Nutrition, 2012) and from
cattle, goats, sheep and pigs (WCRF/AICR - World Cancer Research Fund/American Institute for
Cancer Research, 2007).
A wider literature survey nevertheless suggests that iron contents of chicken (0.40 – 5.40
mg/100g) and pig (0.30 – 4.15 mg/100g) muscle are of similar magnitude, although widely
varying with the nature of muscle and the type of production. The results also suggest that the
proportion of heme iron in total iron is lower in chicken (23-39 %) than in pig (23-60 %) muscle
because of the more glycolytic nature of muscle (Table 14). Such difference does not seem large
enough however to account for the consistent absence of a carcinogenic effect of chicken
consumption in contrast to beef and pork consumption and it has to be accepted that heme
contents of poultry are similar to the values for pork and, although lower than beef, still significant.
Within this context, the increased risk of CRC associated with the consumption of red meat may
be related to a specific component of red meat (mainly beef and pork) other than heme: the
mammalian cell surface sialic acid N-glycolylneuraminic acid (Neu5Gc). This compound is not
produced by bacteria or plants, is low or absent in poultry and fish, but abundant in red meats
(beef, pork, sheep but also meats from other species) and in bovine milk (Byres et al, 2008).
Humans however are genetically deficient in Neu5Gc production and instead metabolically
accumulate it from dietary sources, particularly red meat and milk products. This metabolicallyaccumulated dietary Neu5Gc results in the production of circulating anti-Neu5Gc antibodies
leading to local chronic inflammation and a propensity to develop diet-related carcinomas
(Hedlund et al, 2008). The near absence of Neu5Gc in poultry and fish may explain some
inconsistencies.
− 55−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 14. Total iron (mg/100 g) and heme iron (% of total) in raw and cooked chicken and pig
a
meats .
Chicken (1)b
Legs
Breast
(5)
(8)
(9)
(11)
Pig muscle (2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
a
Raw
Cooked
Total Fe
Total Fe
Heme Fe (%)
1.93 + 0.22
0.65 + 0.20
0.58 - 1.34
39
26
0.65 - 1.43
23 - 39
0.40 - 0.70
0.40 - 5.40
0.50 – 1.20
0.41 - 0.50
1.00 - 2.79
0.46 + 0.07
0.49 - 0.70
2.65 + 0.54
2.65 - 4.13
0.30 - 3.00
0.63 ± 0.04
0.68 - 1.09
0.64 - 1,60
23 - 60
0.90 - 1.30
0.70 – 1.30
b
minimum - maximum values or means + SE references (1) Clark et al (1997) (2) Tomovic et al (2011)
(3) Dannenberger et al (2007) (4) Greenfield et al (2009) (5) Lombardi-Boccia et al (2005) (6) López-Alonso
et al. (2007) (7) López-Alonso et al. (2012) (8) Rooke et al (2010) (9) Schönfeldt et al (2011) (10) Ventanas
et al (2006) (11) Gerber et al (2009)
2.2.6.6 Effect of processing on the carcinogenic effect of red meat
The risk of CRC incidence is higher per g of processed (cured) red meat than per g of
unprocessed red meat (see also Table 2) (Santarelli et al, 2008) as clearly recognized also by
e.g. van den Brandt & Goldbohm (2006), Boyle et al (2008) and Moore (2010). In line with
arguments discussed under 2.2.6.2, Parr et al (2013) did not find an association between intake
of red meat or meat cooking methods and CRC risk but a high processed red meat intake was
associated with increased risk of CRC in a detailed and careful cohort study involving 84.538
Norvegian women. The effect of processed red meat was mainly driven by the intake of sausages
confirming earlier work (Gaard et al, 1996). In a recent report summarizing evidence of the EPIC
study involving 448,568 men and women, Rohrmann et al (2013) concluded that after correction
for measurement error, higher all-cause mortality was significantly related only to processed red
meat and not to red meat intake. The authors even estimated that 3.3% (95% CI 1.5% to 5.0%) of
deaths could be prevented if all participants had a processed red meat consumption of less than
20 g/day. The important impact of these findings justifies a closer look at meat processing and the
reactions involved. In Western meat technology processed red meats are predominantly prepared
from pig meat. As the latter contains less heme iron than beef, the presence of heme cannot be
the sole factor responsible for the increased risk of CRC associated with processed red meat as
compared to fresh meat. Possible explanations obviously relate to the changes provoked by the
addition of processing additives and by processing conditions and it has been suggested that
nitrosyl heme present in processed red meat and hemin used in experimental diets are more toxic
than the native heme from fresh meat myoglobin (Santarelli et al, 2008; Pierre et al, 2010).
− 56−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
The curing process
Apart from smoking, meat processing basically involves “curing”, a process dating back to ancient
times and mainly characterized by the addition of salt (NaCl) containing sodium nitrite (and/or
potassium nitrate as a source of nitrite). Whole meat cuts (hams) are cured by covering with dry
salts, by immersion in brines or, when cooked after curing, by injection of brines. Minced
(ground) meat is cured by mixing (“cuttering”) meat and fat with dry salts. Sodium nitrite (maximal
level 150 ppm in the EU) should be added as a mixture with NaCl (nitrite or curing salt e.g. NaCl
containing 0.6 % NaNO2) in order to prevent instantaneous production of toxic nitrous vapors
(NO2). Other additives often used are ascorbate or erythorbate and sugars. The presence of salt
dissolves proteins and leads to osmotic drying followed by coagulation of proteins and weight loss
during further air drying for periods ranging from some weeks to several months.
Nitrite is mainly used for its anti-bacterial effect, specifically against Clostridium botulinum, and/or
the production of the characteristic bright red (pink when cooked) color originating from its
reaction with myoglobin. However, the possible seven states of oxidation of N ranging between -3
(NH3 ) and +5 (HNO3) associated with the existence of intermediate per-ferryl ions (Fe: +IV and
Fe: +V) (Qian and Buettner, 1999) apart from the ferrous (Fe: +II) and ferri (Fe: +III) ions results
in a very complex set of possible reactions involving interactions with numerous food components
and environmental conditions as described e.g. by Honikel (2008) and Skibsted (2011).
Major reactions can be listed as follows:
Nitrite added to meat primarily acts as an oxidant following:
NO2- + H2O + e- → NO + 2OHinvolving oxidation of reductants such as:
- NADH or added ascorbate and mainly the anhydrous form of nitrous acid N2O3.
- Myoglobin to yield metmyoglobin following
Mb(FeII) + NO2- + H2O → Mb(FeIII) + NO + 2OHThis reaction is responsible for the initial colour change from fresh red {MbFe(II)O2 in
equilibrium with violet MbFe(II) depending on oxygen pressure} to the brown colour of
MbFe(III).
- Subsequently MbFe(III) is reduced to MbFe(II) by reductants like NADH or added
ascorbate.
NO binds strongly to MbFe(II) (but not to MbFe(II)O2) following:
Mb(FeII) + NO → Mb(FeII)NO
causing a second colour transformation to yield the characteristic red colour of cured meat.
This compound loses the globin bond to iron upon heating (Sun et al, 2009) resulting in
nitrosylmyo- or hemochromogen (or nitrosylprotoheme), the pigment changing the product
color from bright red to the characteristic pink color of cooked cured meat (Fig. 14).
Fig. 14. Heme compounds associated with the carcinogenic effects of processed red meats
(Pegg et al, 1997).
Hemin
Nitrosylhemochromogen
Nitrosomyoglobin
− 57−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Apart from these well studied reactions, the use of 15N-labelled sodium nitrite has shown that 73 87% of added nitrite is retained in the muscle proteins of bacon (Woolford & Cassens, 1977). This
underlines the importance of residual nitrite in cured meat proteins as a “hidden NO generating
pool providing nitric oxide for the numerous reactions occurring during storage and cooking of
cured meats” (Skibsted, 2011). These may be analogous to the reactions with iron-sulfur proteins
(enzymes) responsible for the anti-bacterial activity of nitric oxide (Morita et al, 2004) and were
shown e.g. to involve reactions with thiol groups, tryptophan (Nakai et al, 1978) and ascorbic acid
(Izumi et al, 1989) as illustrated in Fig. 15. At pH values relevant for meat, N 2O3, the anhydrous
form of nitrous acid, probably acts as nitrosating agent and reacts faster with ascorbate than with
secondary amines such as proline thus preventing formation of potentially carcinogenic N-nitroso
compounds (Skibsted, 2011).
Fig.15. NO formed from nitrite during meat curing can participate in numerous reactions modifying
proteins and pigments (from Skibsted, 2011)
Residual nitrite in processed red meat is however not limited to the protein fraction as added 15Nlabelled sodium nitrite was recovered in cured whole adipose tissue (Goutefongea et al, 1977)
and for up to 20 -25 % in the adipose part of cured bacon (Woolford & Cassens, 1977). Later
work in model systems has demonstrated the formation of nitrosated lipids by addition of nitro
groups to double bonds (Mouloud et al, 1992). These compounds were recognised as agents
responsible for nitrosamine formation during frying of cured meat (Ross et al, 1987) and acting as
cell signalling molecules in biological systems (Lim et al, 2002). In a more extensive approach,
Nicolescu et al (2004) concluded that the reaction of NO derived from nitrite, with the free radical
intermediates in lipid oxidation acts as as a lipid radical chain termination agent. The “lipid nitrites”
are labile and will function both as NO donors and antioxidants. Both these aspects are obviously
more important for minced cured meat products, containing large amounts of adipose tissue
susceptible to oxidation and possibly acting as NO donors during processing and conservation
but also during digestion. Production of lipid nitrites contributes to the well-recognized antioxidant
effect of nitrite that effectively controls rancidity in processed red meats by inhibiting lipid
peroxidation (Freybler et al, 1993). It is indeed remarkable that in spite of the oxidative properties
of nitrite, and their possible strengthening by the presence of iron and chloride, little lipid oxidation
is observed in processed red meats. It should however be clear that the oxidation status of lipids
− 58−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
is also determined by other reactions involving nitrosomyoglobin with depletion of oxygen or
peroxides and production of NO as described in detail by Skibsted (2011). Peroxynitrite, formed
by the reaction of NO with the superoxide radical anion (NO + O2.- → ONOO- → NO3-) may initiate
lipid oxidation. Antioxidant activity on the other hand also involves NO binding to the heme
ferrous ion forming nitrosomyoglobin and to other non-heme iron proteins preventing pro-oxidant
iron release (e.g. from the porphyrin) (Morrissey & Tichivangana, 1985) during an attack of H2O2
or hydroperoxides (Kanner, 1994). The importance of the latter mechanism is suggested by the
antioxidant effect of the isolated cured meat pigment in the absence of nitrite (Shahidi et al.,
1987). Many other possible reactions may be involved however as e.g. a contribution to an
antioxidant medium by initial oxidation of NO2 in the presence of oxygen (Honikel, 2008). Also,
the pro-oxidant activities of heme pigments present are strongly affected by low pH, the initial
prevalence of deoxygenated heme pigment and the oxidative modification of the heme pigments
as well as the degree of proteolysis (Carlsen et al, 2005). Last but not least, it is clear that during
conservation of processed red meats, the presence of O2 and temperature conditions affect
further oxidation reflected in browning of the products. Exposure to light intensifies oxidation but
only in the presence of O2 as discussed in detail by Skibsted (2011).
Results of dietary intervention studies
Most of the available evidence supports an enhancing effect of nitrite on the formation of NOCs
both in food and endogenously. As discussed above, the presence of nitrite in processed red
meat enhances the formation of NOCs in the food. Indeed, Haorah et al (2001) showed that
hotdogs contained 10 times more NOCs than fresh red meat. Furthermore, ATNC derived from
nitrosation of NOC precursors present in hotdogs induced colonic aberrant crypts in the mouse
colon (Davis et al., 2012). Several studies indicate that the presence of nitrite in processed food
can also increase endogenous formation of NOCs. As for red meat, diets based on processed red
meat have been reported to increase the fecal ATNC content but the effect of processed red
meat appeared to be more pronounced. In mice, diets containing 18 % hot dogs increased fecal
ATNC excretion 3.7-5.0 times compared to controls whereas equal amounts of beef resulted in a
2.6-2.9 fold increase (Mirvish et al, 2003). As fecal ATNC contain both unabsorbed dietary NOC
and endogenously formed NOC, it was not clear if the observed increase was related to the
increased dietary NOC content of processed red meat. In a later experiment, the same research
group (Mirvish et al, 2008) showed that fecal ATNC excretion in mice increased with nitrite in the
drinking water (Fig. 16), an effect even more increased by the presence of heme, whereas there
is no or inconclusive evidence for nitrite being a colon carcinogen.
Fig. 16. Fecal concentration of NOCs for mice fed various doses of NaNO 2 in drinking water (from
Mirvish et al, 2008).
− 59−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Such finding is not surprising as humans are exposed to 4.5 – 13.5 mg nitrite/d from the saliva
(derived from nitrate reduction in the oral cavity) and such levels would increase colonic levels of
ATNC. Endogenous production of nitrite and the important intake of nitrate with vegetables
considerably reduce the probability of a carcinogenic nature for these compounds and arguments
are indeed available to consider them as healthful dietary components (Hord et al, 2009). The
general safety and even beneficial role of nitrate/nitrite in human health has indeed been
extensively confirmed (Sindelar & Milkowski, 2012; Parthasarathy & Bryan, 2012). In this respect
it may be significant to mention that in a large cohort study involving 491,841 participants, nitrite
intake from processed red meats and other animal sources was associated with increased renal
adenocarcinoma risk whereas no association was found for nitrite intake from plant sources or
nitrate intake overall (DellaValle et al, 2013). Nevertheless, it has also been shown that although
low concentrations of nitrite inhibit cancer cell progression at early stage it promotes cancer cell
progression at higher concentrations in cells representing stage 4 colon carcinomas (Jiang et al,
2012). These findings may be related to the reported increased risk of CRC with nitrate in
drinking water (van Grinsven et al, 2010).
A likely hypothesis involves the presence of a minor specific carcinogenic component in the
colonic/fecal ATNCs induced by red and processed red meat other than those induced by nitrite.
Such component is probably a NOC and not an iron nitrosyl or S-nitrosothiol. In this respect, it
should be noted that rats lack an enterosalivary recycing of nitrate. Addition of nitrite to the
drinking water of rats however did not interact with the effect of heme compounds on biochemical
markers linked to colon carcinogenesis (lipid peroxidation, cytotoxicity of fecal contents).
However, according to Chenni et al (2013), addition of nitrite to the drinking water increased the
level of fecal nitroso-compounds but their concentration and their nature (iron-nitrosyl) would
probably not be associated with an increased risk of cancer. Obviously more precision is required
for identification of such compound in colon/fecal contents and recently over 30 putative NOCS
have been identified in fecal material (Clarke et al, 2011).
The recent Danish study involving 185 archival CRC samples collected from participants of the
European Prospective Investigation into Cancer (EPIC)-Norfolk study supports the hypothesis
that heme and nitrite present in processed red meat products may act together to induce higher
levels of NOCs. Indeed, CRC cases harbouring GC-to-AT transition mutations were associated
with processed red meat consumption, suggesting a dietary link with alkylating agents such as
NOCs (Gay et al., 2012). The hypothesis was further supported by the observation that the
promoting effect of nitrite treatment on preneoplastic lesion in the rat colon was linked with an
increased fecal ATNC content (Santarelli, 2010).
The same work however also provides support for a role of preformed (lipid) oxidation products
as suggested by Baradat et al (2011) and Leuratti et al (2002) : the nitrite-treated and oxidized
cured meat model similar to ham stored aerobically and fed to 1,2-dimethylhydrazine sensitized
rats specifically increased the number of colon pre-neoplastic lesions compared with a similar non
nitrite-treated and a similar nonoxidized meat (Table 15). No clear differences could however be
observed in biomarkers for lipid oxidation in the animal, suggesting that the effect is probably
brought about by the lipid oxidation products present in the oxidized product.
In very recent work (Santarelli et al, 2013) nine different cured meat products were fed to rats and
hot dogs and dry fermented sausage significantly and marginally increased mucin depleted foci
respectively. These indicators of carcinogenesis however were not related to levels of lipid
oxidation markers whereas dry fermented sausage contained eight times more TBARS than hot
dogs. The authors suggest that the carcinogenic effects are more probably related to the
formation of ATNC in the gut and/or the products induced by nitrosylated heme. A more
outspoken effect of hot dogs could then relate to the liberation of nitrosyl heme from globin by
cooking in hot dogs and the decreased availability of heme caused by fermentation in dry cured
sausage.
− 60−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 15. Effect of an oxidized processed red meat on pre-carcinogenic changes and biomarkers in
rats (adapted from Santarelli et al, 2010)
Diets
mg MDA eq/100 g meat
Histology
Aberrant crypt foci
Mucin depleted foci (MDF)
Crypts/MDF
Mucin depleted crypts/colon
Fecal water
Heme (µmol/l/24h)
TBARS (μmol/l MDAa equivalent)
Cytotoxicity (% dead cells)
ATNCb (μmol/l as NNO)
Urine
DHN-MAc (μg/24 h)
a
DCNAd
DCNOd
0.5
1.8
81
2.9
3.9
11
100
2.1
2.7
8.0
102*
4.1*
4.2
18.0*
0
58
0
47
137
102*
25
88
324
88*
11
424*#
0.5
5.3*
control
b
3.4
c
MDA = malondialdehyde
ATNC = apparent total N-nitroso compounds
DHN-MA = 1,4d
dihydroxynonane mercapturic acid
Diets fed contained DCNO = dark meat cooked with nitrite and
oxidized; DCNA = dark meat cooked with nitrite and kept anaerobic; Dry matter of diets contained identical
proportions of fat (15 g / 100 g) and protein (40 g /100 g). The control diet 40 g of casein/100 g and
experimental diets 55 g of processed red meat dry matter. Dark meat (supraspinatus and infraspinatus pig
muscles) was cured using salt (NaCl) containing 0.6 g sodium nitrite/100 g salt at 2 g/100 g meat and
cooked at 70°C for 1 hour in vacuum sealed plastic bags in a water bath. DCNA anaerobic meat was
packaged under vacuum immediately after processing in plastic bags with low oxygen permeability and
*
DCNO oxidized meat kept in the dark without any packaging for 5 days after cooking. different from control
#
different from DNA.
An effect of NaCl ?
A major effect of meat processing {nitrite (and/or nitrate) curing} is of course the increased salt
(NaCl) content reaching values ranging from 1 to 10%. The presence of Cl- leads to the
production of nitrosyl chloride following HNO2 + H+ + Cl- → NOCl + H2O. NOCl is more reactive
than N2O3 and chlorine may contribute with nitrite and ascorbate to the Fenton reaction producing
hydroxyl radicals from ROS formed in biological tissues (Skibsted, 2011). Salty diets and salted
foods have consistently been related to stomach cancer, mainly in Japan. Furthermore, NaCl
enhances experimental gastrocarcinogenesis by N-methyl-N’-nitro-N-nitrosoguanidine in rats
(Takahashi et al, 1994). Until now, no link has been published between salt intake and CRC
(Santarelli et al., 2008). However, the experimental evidence discussed above indicates that lipid
(per)oxidation during processing or digestion is very probably an underlying cause of the
increased risk for CRC associated with consumption of red and processed red meat. It was
pointed out (Demeyer & De Smet, 2011) that this may involve free radical damage possibly linked
to myeloperoxidase (MP) catalyzed generation of reactive chlorinating intermediates in the gut.
Indeed, MP activity is part of the regulation of the antioxidant defense and redox status of
tissues. It was shown to be involved in enhanced oxidative stress in neoplastic tissue of the colon
(Rainis et al, 2007) and was found to be strongly dependent on extracellular chloride
concentration in peripheral blood neutrophils (Painter et al, 2008). Also, DNA damage as the
result of HOCl-mediated chlorination by myeloperoxidase has been suggested as a contribution
to lung carcinogenesis (Masuda et al, 2001). The possibility that salt in consumed processed red
meats increases plasma chloride levels that, possibly in combination with heme compounds,
stimulate myeloperoxidase catalyze generation of reactive chlorinated intermediates in the gut is
therefore a hypothesis deserving further consideration and research.
− 61−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.6.7 Summary
Red meat consumption is clearly associated with an increased intake of polycyclic aromatic
hydrocarbons as well as heterocyclic amines, two groups of compounds recognized as
carcinogenic. PAH and HCA may be present as contaminants in the fresh meat and/or are
formed during cooking by contact with the open flame (PAH) or by high temperature treatments to
the “well done” state (HCA). However, both types of compounds are probably not the major
carcinogenic constituents of red meat. Indeed, they are present in similar or greater levels in
chicken and fish cooked in the same manner, foods not found to increase or even lower (fish) the
risk of CRC.
Both
- volatile nitrosamines and non-volatile nitrogen nitrosocompounds
as well as
- lipid oxidation products
are probably the most important compounds responsible for the increased risk for colorectal
carcinogenesis associated with the consumption of both fresh and processed (nitrite cured) red
meats.
They are formed
- during nitrite (and/or nitrate) curing and conservation of processed red meats
and/or
- during intestinal digestion of red meats and processed red meats.
The production of both types of compounds during digestion is intensified by the presence of
heme. Furthermore, due to the presence of nitrite heme mediated formation of lipid oxidation
products as well as volatile nitrosamines and non-volatile nitrogen nitrosocompounds (yet to be
identified) also occurs during processing and conservation of processed red meats. The ingestion
of these compounds and their interaction with the colon epithelium probably explains the greater
risk of processed red meats than of fresh red meats. The presence and formation of NOCs and
lipid peroxidation products in processed (nitrite cured) meats deserves extensive additional
research in relation to the justification of nitrite use in meat processing (Mirvish et al, 2008). A
summarizing scheme presented by Corpet (2011) may not accurately nor completely cover all
points discussed but also illustrates some mediating effects on heme induced carcinogenesis to
be discussed hereafter (Fig.17). It should also be realized that considering all the different
hazardous compounds present in red and processed red meat, the increased risk for CRC may
not be associated with one unique causative agent, but with the presence of the different
compounds, acting on multiple stages of CRC.
− 62−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Fig.17. Catalytic effect of heme iron on fat peroxidation and N-nitrosation, and their inhibition by
dietary means. Consequences for the development of colorectal cancer. Heme iron catalyzes
nitrosation and fat peroxidation. End products are N-nitroso compounds (NOCs), malondialdehyde
(MDA) and 4-hydroxy-nonenal (4-HNE). These pathways explain, at least in part, the promoting
effect of red and cured meat on colorectal cancer. The catalytic effects of heme iron can be
inhibited by trapping heme with calcium carbonate or chlorophyll. The endogenous formation of
NOCs is inhibited by vitamin C and E. Ongoing studies suggest that specific polyphenols can
inhibit fat peroxidation and/or nitrosation (From Corpet, 2011).
− 63−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.7 Possibilities for mitigation
Possibilities to mitigate
-
the carcinogenic effect of red meat and processed red meat,
the established toxicity of heme and nitrosyl heme in relation to the production of nitrogen
nitroso compounds and lipid oxidation products during processing {nitrite (and/or nitrate)
curing}, preparation (cooking) and conservation of processed red meats as well as during
intestinal digestion (nitrosation) of red meat and processed red meats
are apparent from:
Observed effects of dietary changes
The only foods reported by WCRF/AICR (2011) to decrease the risk of colorectal cancer are
dietary fiber (convincingly) as well as garlic and cow’s milk (probably). A risk decreasing effect of
fish intake is strongly supported by the European Prospective Investigation into Cancer and
Nutrition (2012) and other extensive work (Hall et al, 2008) (Wu et al, 2012). These facts should
support the concept of “healthy eating” as elaborated in relation to overweight and obesity (see
e.g. Vanhauwaert, 2012) also for the prevention of CRC. A nearly significant protective
association of a higher intake of vegetables and fruits, an index of “healthy eating”, with the
overall risk of colorectal cancer has also been identified (Kurotani et al, 2010) and is generally
accepted although the relation to folate supply requires some clarification (Lee & Chan, 2011). A
large cohort study from the Italian EPIC study (Pala et al, 2011) involving 45,241 subjects clearly
demonstrated an inverse association of yogurt intake with CRC risk, adjusted for energy, simple
sugar, calcium, fiber, animal fat, alcohol and red meat intake, as well as body mass index,
smoking, education and physical activity. The relative risk was 0.66 for the highest compared to
the lowest yogurt intake. This finding confirms protective effects of dairy foods and calcium
supplements reported earlier (Park et al, 2009). In a more general approach, Holtrop et al (2012)
recently demonstrated the complexity of dietary factors determining the formation of carcinogenic
NOC in humans.
Consumption of meat-based weight-loss diets increased fecal NOC excretion in obese subjects,
and this effect was increased mainly by dietary meat and nitrate contents.
Other dietary components namely vitamin C, total energy, and non-starch polysaccharides
however attenuated the effect in a complex manner involving e.g. the ratio of dietary components
present. In other large scale observational work, it was recently confirmed that non-red meat
sources of animal protein, often derived from low-fat dairy products, fish and poultry sources are
associated with lower risks of CRC (Sun et al, 2012; Miller et al, 2013).
Experimental work with animals or volunteers
Major effects apparent from observational studies have been at least partially confirmed in
experimental work. Joosen et al (2010) showed that although replacement of red meat with fatty
fish had no effect on endogenous nitrosation, inflammation and genotoxicity of faecal water in
apparently healthy human volunteers, it does reduce the formation of mutagenic and potentially
carcinogenic NOC and may as such beneficially affect colorectal risk. The feeding of cruciferous
vegetables (cauliflower, cabbage, broccoli, …), yogurt, and chlorophyllin tablets to fried meat
consuming volunteers clearly resulted in enhanced urinary voidance of diet induced mutagens
associated with a significant decrease of fecal mutagenicity and a nearly twofold decrease of the
DNA damage in colorectal cells (Shaughnessy et al, 2011). A suppressive effect of calcium
carbonate on promotion of carcinogenesis by beef meat was demonstrated in rats and was more
efficient than that of calcium phosphate (Allam et al, 2011). The recent work of Santarelli et al
(2013) shows that a high-calcium diet suppresses the carcinogenic effect of hot dogs in rats and
the authors suggest “an alternative protective strategy against colorectal cancer: processed red
meat meals should also include a calcium-rich food to counteract toxicity of cured meat”. Calcium
supplements or α-tocopherol addition fully normalizes fecal TBARS in volunteers given cured
− 64−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
meats (Santarelli, in preparation cited in Corpet, 2011a) and levels of postprandial plasma MDA
showed up to 80 % reduction by consumption of red wine polyphenols (Kanner et al, 2012;
Gorelik et al, 2013) or coffee (Sirota et al, 2013) polyphenols during a meat meal in humans.
Widely accepted former knowledge for the protective effect of resistant starch for colorectal
cancer in relation to a butyrate hind gut fermentation (Higgins & Brown, 2013) (Fung et al., 2013)
was confirmed for red meat carcinogenesis in rats (Toden et al, 2007; Toden et al, 2010; Winter
et al, 2011; Conlon et al, 2012). It was shown for the first time in humans that addition of
resistant starch to high red meat diets reduced formation of a meat induced promutagenic adduct
(Winter et al, 2012) as well as of mi-RNAs over expressed in CRC (Le Leu et al, 2012). Although
primarily fermented in the caecum, wheat fiber arabinoxylans protected colonocytes from DNA
damage and changed colonic microbial composition when fed to pigs, in conjunction with lower
phenol concentrations and altered microbial populations (Belobrajdic et al, 2012). Tumor
suppressive effects of dietary spinach were demonstrated in the rat colon and were linked to the
lowered formation of altered micro RNAs specific for heterocyclic amine-induced colon cancers
(Parasramka et al, 2012).
Demonstrated possibilities for optimization of meat processing and meat preparation
Adding antioxidant spices (rosmarinic acid) during cooking of hamburgers lowered
malondialdehyde levels in meat as well as in plasma and urine after ingestion by volunteers (Li et
al, 2010; Li et al, 2013). It is not clear whether an effect on malondialdehyde in vivo is involved
besides the effect in the product. Smoking conditions can be optimized to minimize the PAH
content of Frankfurter-type sausages (Pöhlmann et al, 2012). In relation to domestic meat
preparation, the effects of grilling and over-grilling on benzo[a]pyrene formation in meat and
chicken samples were investigated (Ince & Yaman, 2012) and well as the effects of pan-frying
and microwave heating on N-nitrosamines in dry-cured sausage (Li et al, 2012). Addition of plant
polyphenols in production of the latter was reported to lower levels of both TBARS and Nnitrosamines (Li et al, 2013). The use of spices lowers HCA production during cooking of beef as
illustrated for PhIP in Table 16 and inhibitory effects were observed with other plant compounds
for pork (Zhang et al., 2013). Similar reductions were found after treating beef with marinades
containing polyphenolic antioxidant spices 1 h prior to grilling (Smith et al, 2008) but the use of
alcohol in marinades may have the opposite effect (Wu et al, 2011)(Viegas et al, 2012a). Plant
extracts inhibit both E.Coli O157:H7 and heterocyclic amine production in heated ground beef
(Rounds et al, 2013). The work of Santarelli et al (2010) shows that pork meat cured without
nitrite or packaged to prevent oxidation does not promote carcinogenesis in rats. α-Tocopherol
added to the curing solution suppresses cured meat promotion of CRC in rats and associated
biomarkers in volunteers (Corpet, unpublished results cited in Corpet, 2011a). It should be
realized that the Mediterranean processing of raw and cured ham (e.g. Parma ham) is often
characterized by the absence of nitrite and the presence in the products of Zn-Protoporphyrin, a
compound known to inhibit hemin-induced DNA damage and cell hyperproliferation. It is formed
by both enzymatic and non-enzymatic pathways involving an iron-removal reaction catalyzed by
ferrochelatase, and its formation is inhibited by nitrite (Becker et al, 2012)(Fig. 18). The use of
exogenously added recombinant yeast ferrochelatase is investigated and can open approaches
to lower heme contents of cured meats (Chau et al, 2011).
Other possibilities to mitigate the CRC promoting effect of processed red meats include use of
less nitrite or use of promising natural nitrite alternatives (see e.g. Rodriguez-Sanchez et al.,
2013) as aimed at e.g. in a recently initiated European Research Project: “Phytochemicals to
Reduce Nitrite In Meat Products: Phytome”
(http://www.fenavian.be/goto.php?id=74c407e263578d03d02c1123aa730b52&type=docs) and
analogous research projects running in Flanders.
Other targets involve the development of “functional meat products” introducing e.g. fructooligosaccharides (a “functional probiotic” ?!) in fermented cooked sausages (dos Santos et al,
2012); up to 50 % substitution of pork fat by canola oil in pate or liver sausage (Morales-Irigoyen
et al, 2012) and red meat products enriched with fermentable dietary fiber shown to improve
colonic health in rats (Paturi et al, 2012).
− 65−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Processed meats can be enriched in plant antioxidants, calcium and (long chain) omega-3
unsaturated fatty acids through processing and/or animal feeding (Raes et al., 2004; Demeyer et
al., 2008; Doolaege et al., 2012; Vossen et al., 2012; de Ciriano et al., 2013). The latter have
indeed been shown to be associated with a decreased risk of CRC (Shen et al., 2012) (Zhong et
al., 2013).
Mediation of iron levels in pork by genetic selection has been proposed (Hermesh & Jones, 2012)
and a special mention deserves the promoting effect of chloride salts on lipid oxidation in
processed red meats (Gheisari & Motamedi, 2010). Substitution of “salt” in processed red meats
by other chlorides should therefore be avoided (Selgas et al, 2009). Possibilities to improve the
health properties of red meat and processed red meat products were comprehensively reviewed
by Olmedilla-Alonso et al. (2013) stressing the requirement for dietary intervention studies to
evaluate health effects.
Table 16. Effect of spices on PhIP production in cooked beef
Spices added
Minced Garlic (g/100g)
0
5
10
15
Rosemary
0
0.2 %
1
2
PhIP (ng/g)
Reference
Jung et al (2010)1
264
222
57
40
Puangsombat et al (2011)2
6.53
4.15
ground beef patties fried at 220°C for 10 min
beef patties cooked at 204°C (400 ◦F) for 10 min
Fig. 18. Scheme for the interaction of nitrite with the production of zinc protoporphyrin (From
Becker et al, 2012).
− 66−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
2.2.8 The types of processed red meats involved
Although the WCRF/AICR (2007) recommendation clearly defines “processed red meats” as
“meats preserved by smoking, curing or salting or by the addition of chemical preservatives”, a
lack of the precise definition of processed red meats is often pointed out (Demeyer et al, 2008).
Indeed, contrasting with dairy products, the processed red meats are a very diverse group of
foods, characterized by the use of very heterogeneous raw materials (different muscle and fat
tissues, organs, blood, …) as e.g. recognized in a recent FAO publication (Heinz &Hautzinger,
2007) (Fig. 19).
Fig. 19. Meat products grouped according to the processing technology applied (Heinz
a
&Hautzinger, 2007)
a
Fotographs of typical examples available at http://www.fao.org/docrep/010/ai407e/AI407E09.htm
In Western meat technology, processed red meats are predominantly prepared from pig meat. In
fact, it can be estimated that in Belgium, pig meat provides about 80 % of processed red meats
and that at least about 50 % of pig meat is processed (Anonymous, 2010), suggesting that pig
meat consumption reflects to a considerable extent processed (cured) meat consumption.
Perhaps contrasting with a general perception, it can be estimated that pig carcasses mainly
provide more than twice the amount of fat than protein, even when lean breeds are considered
(Table 17). Efficient meat technology however recovers most of the fat in a diversity of products
widely differing in fat content as shown e.g. in a product classification recently used by
Vandendriessche (2008) (Table 18). As apparent from Fig. 19 however the latter classification
does not sufficiently cover differences in fat content as well as in the use of nitrite. In view of the
large differences in fat content and the established relation of lipid oxidation as well as the use of
nitrite to the promotion of CRC by processed red meats, a different effect between high fat
(minced products) and lower fat (whole muscle products) might be expected, even in the absence
of nitrite. In the context of specific recommendations for Belgium, a variety of ground red meat
products with added fat and salt but no nitrite should perhaps be considered separate from fresh
as well as from processed red meats. In fact, such ground “mixed meats”
(vleesmengelingen/viandes hachées) covering hamburger, fricadel, meat balls, brochettes,
pita/gyros and similar products made up over 30 % of fresh meat home purchases between 2002
and 2012
(http://www.vlam.be/marketinformationdocument/files/GfKvleesinclusiefgevogeltewildenkonijn201
2-AP.pdf).They are often heated and may contain added poultry.
− 67−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 17. Estimated protein and fat yield from pigs and cattle (% of live weight)
muscle
adipose tissue
Tissue
Protein
Tissue
Fat
Lean Pig
44 (20)a
8.8
24 (80)b
19.2
Double muscled beef
44 (20)
8.8
12 (80)
9.6
a
b
between brackets estimate for % protein in muscle
estimate for % fat in adipose tissue
Table 18. Mean fat contents of different processed red meat types in Belgium (Vandendriessche,
2008)
Product
Whole muscle products
Minced (ground) products
Type
% fat
Type
% fat
Heated
Cooked ham
0.5 - 5
Luncheon meat
20 - 30
Raw
Dry cured ham
(e.g. Parma, Iberico)
2.5 - 10
Fermented dry
sausage (e.g.
chorizo)
30 – 40
In Swedish research (Larsson et al., 2006) similar hazard risk ratio estimates of 1.55, 1.50 and
1.48 were found for bacon, hot dogs and salami, respectively but to our knowledge however no
systematic studies have compared different processed red meats in epidemiology.
Although data are affected by possible differences in effectiveness of registration rate, it is
generally recognized that colorectal cancer death rates differ between Northern Europe and
Mediterranean countries (Parnaud &Corpet, 1997). We have therefore attempted to gain insight
in this problem by comparison of the consumption of specific processed red meats between
Northern and Southern European countries as observed in the EPIC study and described by
Linseisen et al (2006). Using the data for women (slightly different only from data for men), Table
19 illustrates striking differences: women in Northern Europe consume about twice the amount of
processed red meats (38 g/d) than in Southern Europe (20 g/d). The proportion of raw and cured
products (e.g. raw ham and salami type) is about twice as important in Southern Europe (32 %)
compared to Northern Europe (14 %). In Northern Europe a much higher proportion of cooked
and cured sausages (46 vs. 34 %) and “minced” hamburger type products (13 vs. 4 %) is
consumed.
It can be calculated that the average consumption of the latter product classes known to be high
in fat content amounts to 22.6 g/d and 7.6 g/d in Northern and Southern Europe respectively.
Considering the absence of added nitrite in the production technology of Mediterranean dry-cured
ham containing Zn-Protoporphyrin as discussed above, these results are in line with the
hypothesis that the higher incidence of processed red meat induced colorectal cancer in Northern
compared to Southern Europe mainly relates to a higher consumption of fatty meat products and
Fe-nitrosyl-heme provoked lipid peroxidation in the product and/or the gut.
− 68−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Table 19. Adjusted mean (± SE) daily intake of processed (cured) meat product classes in women
calculated from EPIC study data (Demeyer & De Smet, 2011).
Total (g/day)
Southern Europe
(n=4) a
Northern Europe
(n=5) b
UK
20 ± 3.7
38.4 ± 3.6
24.3
14.4
4.5
% of total
Raw cured
Ham
Salami type
32.8
Cooked cured
Ham
Sausages
52.2
Main other
Bacon
Minced1
Cuts2
Raw spreadable
15.0
15.5 ± 4.7
17.3 ± 7.9
7.8 ± 1.7
6.6 ± 1.8
58.9
19.4 ± 6.0
33.9 ± 5.8
0.8
3.7
30.9
12.7 ± 1.6
46.2 ± 3.4
26.7
3.6 ± 0.1
4.0 ± 2.1
5.0 ± 2.3
0.6 ± 0.4
21.4
9.5
64.6
3.6 ± 1.0
12.7 ± 4.0
9.6 ± 2.9
0.7 ± 0.3
a
Greece, Spain, Italy, Southern France;
Germany, The Netherlands, Denmark, Norway, Sweden
1
Hamburger, fricadel, meat balls; liver pâté
2
Roasted meat in aspic, schnitzel, ..
b
− 69−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
24.8
12.4
1.7
25.7
3
CONCLUSIONS AND RECOMMENDATIONS
For the benefit of the Spanish Governments, Bejar et al (2010) stated that “a minimal time span
of ten-fifteen years is necessary for changes in exposure to risk factors” to be able to modify the
incidence of CRC. This report confirms their conclusion that implementation of “legislative and
educational measures in the field of Health Promotion regarding the diet can therefore be
considered urgent”. Such measures should inform the consumer how to make healthy food
choices based on scientific evidence in a clear and straightforward manner not drown in the
actual confusing information cloud (Perez-Cuero & Verbeke, 2012). Discussing guidelines for a
healthy diet from an ecological perspective, the Dutch Health Council (Health Council of the
Netherlands, 2011) concluded that “the average consumption of red meat at the population level
and the combined intake of red and processed red meat exceeded the norms set by the World
Cancer Research Fund and the British Scientific Advisory Committee on Nutrition”. Based on one
reference only (not covered by the ISI Web of Science nor by PubMed) it considers that “the
significance of this fact for questions of health is uncertain”. Nevertheless, its recommendations
for other reasons involve only “occasional consumption” of “mince, rolled beef and sausage”
(meat) and of “raw ham, smoked meat, frankfurter, shoulder of ham, sausage, bacon, pâté and
pork fricandeau” (meat products). Evaluating the “New Nordic diet”, Adamsson et al (2012) refer
to “ a primarily plant-based diet ... associated with decreased morbidity and mortality”. In analogy
with more evidence based and explicit French (Programme National Nutrition Santé, France,
2009) and UK (Scientific Advisory Committee on Nutrition, UK, 2010) guidelines this report
justifies a proposal to amend the existing recommendation at the federal Government level
(“Nationaal voedingsplan voor een betere gezondheid - Plan National Nutrition pour une meilleure
santé”
at
http://www.belgium.be/nl/gezondheid/gezond_leven/voeding/nationaal_plan/
or
http://www.belgium.be/fr/sante/vie_saine/alimentation/plan_national/).
The epidemiological evidence is less clear when higher upper levels of intake (up to about 200
g/d) are absent and is not apparent with populations of older and health conscious individuals
(see under 2.2.2.4). Also, it has been shown that moderate amounts of red meat (~ 100 g/d for
adults ) remain valuable sources for net protein synthesis for the elderly. It is therefore proposed
to maintain the actual recommended maximal intake of 100 g/d of the food group
meats/fish/eggs/legumes/meat substitutes and the adapted proposal reads : “It is recommended
to consume not more than 100 g per day (amount before preparation) of the food group
meats/fish/eggs/legumes/meat substitutes. A high consumption of red meat (mainly beef, pork,
sheep but also meats from other species except poultry), mixed meats (with added fat and salt)
and even more, of processed red meats (mainly cured using nitrite) slightly increases the risk of
colorectal cancer. Therefore, choose preferably poultry, limit red and mixed meats and avoid
processed red meats, in particular fatty meat products of the cooked sausage type, paté and
salami. When preparing red meat (baking, roasting and cooking) make full use of vegetable
spices, do not overheat the meat to a dark brown colour but, when present, remove such parts on
the plate before consumption. Eating fish, including fat fish, once or twice a week is
recommended as well as the occasional use of vegetable meat alternatives.”
It should be remembered that “red meat” and “mixed meats” refer to fresh red meat products that
have not been subjected to other treatments than cooling, freezing and or comminution for mixing
with other red meats and salt (e.g. ground meat and hamburger type products). Processed red
meat is defined as ”red meats preserved by salting (mainly with addition of nitrite and/or nitrate)
and one or more other treatments”. In quantitative terms and in accordance with the WCRF/AICR
(2007) this means that at the level of the individual who eats red meat, the recommendation is not
to exceed the consumption of 500 g/week, very little if any of which to be processed.. This should
be in accordance with a public health goal for a population average consumption of less than 300
g/week of red meat, very little if any of which to be processed, a goal aimed at effects
complementary to the screening effort planned in Flanders. In addition and in comparison to the
messages related to the abstention of smoking and excessive alcohol use, an
− 70−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
alternative/additional and more straightforward and simple message for the consumer as inspired
by Perez-Cuero & Verbeke (2012) might be:
“The best prevention of colorectal cancer is the combination of higher physical activity
with a fiber-rich diet, limiting red meat and minimizing processed meat products.”
− 71−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
4
REFERENCES
Adamsson V, Reumark A, Cederholm T, Vessby B, Rise´rus U, Johansson G. What is a
healthy Nordic diet? Foods and nutrients in the NORDIET study Food & Nutrition Research
2012;56:18189.
Alaejos MS, Gonzalez V, Afonso AM. Exposure to heterocyclic aromatic amines from the
consumption of cooked red meat and its effect on human cancer risk: A review Food additives
and contaminants. 2008;25:2-24.
Alexander DD, Cushing CA. Red meat and colorectal cancer: a critical summary of
prospective epidemiologic studies. Obesity reviews 2011;12:e472–e93.
Alexander DD, Cushing CA, Lowe KA, Sceurman B, Roberts MA. Meta-analysis of animal fat
or animal protein intake and colorectal cancer. American journal of clinical nutrition
2009;89:1402-09.
Alexander DD, Miller AJ, Cushing CA, Lowe KA. Processed meat and colorectal cancer: A
quantitative review of prospective epidemiologic studies. Eur J Cancer 2010;19:328–41.
Alexander DD, Weed DL, Cushing CA, Lowe KA. Meta-analysis of prospective studies of red
meat consumption and colorectal cancer. European Journal of Cancer Prevention
2011;20:293–307.
Alexander J, Benford D, Cockburn A, Cravedi J-P, Dogliotti E, Di Domenico et al. Polycyclic
Aromatic Hydrocarbons in Food - Scientific Opinion of the Panel on Contaminants in the Food
Chain (Question N° EFSA-Q-2007-136) The EFSA Journal 2008;724:1-114.
Allam O, Bahuaud D, Taché S, Naud N, Corpet DE, Pierre FH. Calcium carbonate suppresses
haem toxicity markers without calcium phosphate side effects on colon carcinogenesis. British
Journal of Nutrition 2011;105:384–92.
Al-Sohaily S, Biankin A, Leong R, Kohonen-Corish M, Warusavitarne J. Molecular pathways
in colorectal cancer. Journal of Gastroenterology and Hepatology 2012;27:1423-31.
Altorf-van der Kuil W, Brink EJ, Boetje M, Siebelink E, Bijlsma S, Engberink MF, van 't Veer P,
Tomee D, Bakker SJL, van Baak MA, Geleijnse JM. Identification of biomarkers for intake of
protein from meat, dairy products and grains: a controlled dietary intervention study British
Journal of Nutrition 2013;110:810-22.
Anand P, Kunnumakara AB, Sundaram C, Harikumar KB, Tharakan ST, Lai OS et al. Cancer
is a Preventable Disease that Requires Major Lifestyle Changes. Pharmaceutical research
2008;25:2097-116.
Andersen V, Ostergaard M, Christensen J, Overvad K, Tjonneland A, Vogel U.
Polymorphisms in the xenobiotic transporter Multidrug Resistance 1 (MDR1) and interaction
with meat intake in relation to risk of colorectal cancer in a Danish prospective case-cohort
study. BMC Cancer 2009;9:Art. No. 407.
Andersen V, Christensen J, Overvadd K, Tjønneland A,Vogel U. Heme oxygenase-1
polymorphism is not associated with risk of colorectal cancer: a Danish prospective study.
European journal of gastroenterology & hepatology 2011;123:282–85.
Andersen V, Holst R, Vogel U. Systematic review: diet-gene interactions and the risk of
colorectal cancer. Alimentary Pharmacology & Therapeutics 2013;37:383-91.
Anderson KE, Sinha R, Kulldorff M, Gross M, Lang NP, Barber C et al. Meat intake and
cooking techniques: associations with pancreatic cancer. Mutation Research 2002;506:225–
31.
Andrews NC. Molecular control of iron metabolism: Best Practice & Research. Clinical
haematology 2005;18:159-69.
Angeli JP, Garcia CC, Sena F, Freitas FP, Miyamoto S, Medeiros MH et al. Lipid
hydroperoxide-induced and hemoglobin-enhanced oxidative damage to colon cancer cells.
Free radical biology and medicine 2011;51:503-15.
Anonymous. Prijzen, kosten en rendabiliteit in de varkenskolom. Federale Overheidsdienst
Economie, K.M.O., Middenstand en Energie. Brussel: 2010. Available from:
URL:<http://economie.fgov.be/nl/binaries/study_porc_nl_tcm325-73348.pdf>
− 72−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Aston LM, Smith JN, Powles JW. Impact of a reduced red and processed meat dietary pattern
on disease risks and greenhouse gas emissions in the UK: a modelling study. BMJ OPEN
2012;2:Article Number:e001072.
Atkin W. Editorial: Implementing screening for colorectal cancer. BMJ 1999;319:1249.
Augustsson K, Skog K, Jägerstad M, Steineck G. Assessment of the human exposure to
heterocyclic amines. Carcinogenesis 1997;18:1931–35.
Aune D, Chan DS, Vieira AR, Rosenblatt DA, Vieira R, Greenwood DC et al. Red and
processed meat intake and risk of colorectal adenomas: a systematic review and metaanalysis of epidemiological studies. Cancer Causes & Control 2013;24:611-27.
Baghurst PA. Colorectal cancer. Nutrition & Dietetics 2007;64:S173-80.
Bajro MH, Josifovski T, Panovski M, Jankulovski N, Nestorovska AK, Matevska N et al.
Promoter length polymorphism in UGT1A1 and the risk of sporadic colorectal cancer. Cancer
Genetics 2012;205:163-67.
Bao Y, Nimptsch K, Chan AT, Ng K, Meyerhardt JA, Willett WC et al. Reported behavior of
eating anything at anytime and risk of colorectal cancer in women. International journal of
cancer 2012;130:1395-400.
Baradat M, Jouanin I, Dalleau S, Tache S, Gieules M, Debrauwer L et al. 4-Hydroxy-2(E)nonenal Metabolism Differs in Apc(+/+) Cells and in Apc(Min/+) Cells: It May Explain Colon
Cancer Promotion. Heme Iron Chemical research in toxicology 2011;24:1984-93.
Barbir A, Linseisen J, Hermann S, Kaaks R, Teucher B, Eichholzer M et al.
Effects of phenotypes in heterocyclic aromatic amine (HCA) metabolism-related genes on the
association of HCA intake with the risk of colorectal adenomas. Cancer Causes & Control
2012;23:1429-42.
Baron CP, Andersen HJ. Myoglobin-Induced Lipid Oxidation. A Review. J. Agric. Food Chem.
2002;50:3887-97.
Bartsch H, Nair J. Oxidative stress and lipid peroxidation-derived DNA lesions in inflammation
driven carcinogenesis. Cancer Detect. Prev. 2004;28, 385-91.
Bastide NM, Pierre FH, Corpet DE. Heme Iron from Meat and Risk of Colorectal Cancer: A
Meta-analysis and a Review of the Mechanisms Involved. Cancer Prev Res 2011;4:177-84.
Bax M-L, Buffière C, Hafnaoui N, Gaudichon C, Savary-Auzeloux C, Dardevet D et al. Effects
of Meat Cooking, and of Ingested Amount, on Protein Digestion Speed and Entry of Residual
Proteins into the Colon: A Study in Minipigs. Plos One 2013;8: 4-e61252.
Becker EM, Westermann S, Hansson M, Skibsted LH. Parallel enzymatic and non-enzymatic
formation of zinc protoporphyrin IX in pork. Food chemistry 2012;130:832-40.
Bejar L, Gili M, Ramirez G, Lopez J, Cabanillas JL. Dietary changes and colorectal cancer
trends in Spain during 1951-2007.
Revista Espanola de Enfermedades Digestivas
2010;102:159-64.
Bejar LM, Gili M, Infantes B, Marcott PF. Incidence of colorectal cancer and influence of
dietary habits in fifteen European countries from 1971 to 2002. Gaceta sanitaria 2012;26:6973.
Belobrajdic DP, Bird AR, Conlon MA, Williams BA, Kang S, McSweeney CS et al. An
arabinoxylan-rich fraction from wheat enhances caecal fermentation and protects colonocyte
DNA against diet-induced damage in pigs. British Journal of Nutrition 2012;107:1274-82.
Beresford SA, Johnson KC, Ritenbaugh C, Lasser NL, Snetselaar LG, Black HR, et al. Lowfat dietary pattern and risk of colorectal cancer - The Women's Health Initiative randomized
controlled dietary modification trial JAMA-Journal of the American Medical Association
2006;295:643-54.
Bhopal RS, Bansal N, Steiner M, Brewster DH. Does the 'Scottish effect' apply to all ethnic
groups? All-cancer, lung, colorectal, breast and prostate cancer in the Scottish Health and
Ethnicity Linkage. Cohort Study BMJ OPEN 2012;2: Article Number:e001957.
Biasi F, Chiarpotto E, Sottero B, Maina M, Mascia C, Guina T et al. Evidence of cell damage
induced by major components of a diet-compatible mixture of oxysterols in human colon
cancer CaCo-2 cell line. Biochimie 2012;95: 632-40.
− 73−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Bingham SA, Hughes R, Cross AJ. Effect of White Versus Red Meat on Endogenous NNitrosation in the Human Colon and Further Evidence of a Dose Response. J. Nutr.
2002;132:3522S–25S. Biochimica et Biophysica Acta 823:111-45.
Boland CR, Goel A. Microsatellite Instability in Colorectal Cancer.
Gastroenterology
2010;138:2073-U87.
Bos JL. RAS oncogenes in human cancer - a review. Cancer Research 1989;49:4682-89.
Botma A, Vasen HF, van Duijnhoven FJ, Kleibeuker JH, Nagengast FM, Kampman E. Dietary
Patterns and Colorectal Adenomas in Lynch Syndrome. The GEOLynch Cohort Study Cancer
2013;119:512-21.
Bourre JM. Nutritional value of beef. Bulletin de l’Académie Nationale de Médecine
2011;195:1787-99.
Boyle P, Boffetta P, Autier P. Editorial : Diet, nutrition and cancer: public, media and scientific
confusion. Annals of Oncology 2008;19:1665–67.
Butler LM, Wang R, Koh WP, Yu MC. Prospective study of dietary patterns and colorectal
cancer among Singapore Chinese. British Journal of Cancer 2008;99:1511–16.
Byres E, Paton AW, Paton JC, Lofling JC, Smith DF, Wilce MC et al. Incorporation of a nonhuman glycan mediates human susceptibility to a bacterial toxin. Nature 2008;456: 648-53.
Cai J, Zhao Y, Zhu CL, Li J, Huang ZH. The association of NAT1 polymorphisms and
colorectal carcinoma risk: evidence from 20,000 subjects. Molecular Biology Reports
2012;39:7497-503.
Camilleri GM, Verger EO, Huneau JF, Carpentier F,Dubuisson C, Mariotti F. Plant and Animal
Protein Intakes Are Differently Associated with Nutrient Adequacy of the Diet of French Adults.
Journal of Nutrition 2013;143:1466-73.
Carlsen CU, Møller JK, Skibsted LH. Review : Heme-iron in lipid oxidation. Coordination
Chemistry Reviews 2005;249: 485–98.
Chan DS, Lau R, Aune D, Vieira R, Greenwood DC, Kampman E et al. Red and Processed
Meat and Colorectal Cancer Incidence: Meta-Analysis of Prospective Studies. PLoS ONE
2011; 6: Art. No. e20456.
Chau TT, Ishigaki M, Kataoka T, Taketani S. Ferrochelatase Catalyzes the Formation of Znprotoporphyrin of Dry-Cured Ham via the Conversion Reaction from Heme in Meat. J. Agric.
Food Chem. 2011;59:12238–245.
Chenni FZ, Tache S, Naud N, Gueraud F, Hobbs DA, Kunhle GG et al. Heme-induced
biomarkers associated with red meat promotion of colon cancer are not modulated by the
intake of nitrite. Nutrition and Cancer. An International Journal 2013;65:227-33.
Chizzolini R, Zanardi E, Dorigoni V, Ghidini S. Calorific value and cholesterol content of
normal and low-fat meat and meat products. Trends Fd Sci & Technol 1999;10: 119-28.
Cho E, Smith-Warner SA. Meat and fat intake and colorectal cancer risk: a pooled analysis of
14 prospective studies In: Proceedings of the 95th Annual Meeting of the American
Association for Cancer Research. 2004;27-31 Orlando, Florida (FLA): AACR; abstract 491.
Available from:
URL:<http://www.aacrmeetingabstracts.org/cgi/content/abstract/2004/1/113?maxtoshow=&hits
=10>
Cirillo T, Montuori P, Mainardi P, Russo I, Fasano E, Triassi M et al. Assessment of the dietary
habits and polycyclic aromatic hydrocarbon exposure in primary school children. Food
Additives and Contaminants 2010;27:1025–39.
Clark EM, Mahoney AW, Carpenter CE. Heme and total iron in ready-to-eat chicken. Journal
of Agricultural and Food Chemistry 1997;45:124-6.
Clarke DB, Startin JR, Hasnip SK, Crews C , Lloyd AS, Dennis MJ. Progress towards the
characterisation of faecal N-nitroso compounds. Analytical methods 2011;3:544-51.
Clevers H. At the crossroads of inflammation and cancer. J Cell 2004;118: 671-4.
Collins D, Hogan AM, Winter DC. Microbial and viral pathogens in colorectal cancer. Lancet
Oncol 2011;12: 504–12.
Collins JF, Wessling-Resnick M, Knutson MD. Hepcidin Regulation of Iron.
− 74−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
J. Nutr. 2008;138:2284–8.
Colon Cancer Family Registry and the Genetics and Epidemiology of Colorectal Cancer
Consortium. Identification of Genetic Susceptibility Loci for Colorectal Tumors in a GenomeWide Meta-analysis. J Gastroenterology 2013;144:799- 807.
Conlon MA, Kerr CA, McSweeney CS, Dunne RA, Shaw JM, Kang S et al. Resistant Starches
Protect against Colonic DNA Damage and Alter Microbiota and Gene Expression in Rats Fed
a Western Diet. Journal of nutrition 2012;142:832-40.
Corpet D. Red meat and colon cancer: Should we become vegetarians, or can we make meat
safer? Meat science 2011;89:310-16.
Corpet D. Review of the mechanisms for the effects of red and processed meat on colorectal
cancer. In: WCRF/AICR 2011a;124-27.
Cortese S, Azoulay R, Castellanos FX, Chalard F, Lecendreux M, Chechin D et al. Brain iron
levels in attention-deficit/hyperactivity disorder: A pilot. MRI study. World Journal of Biological
Psychiatry 2012;13:223-231.
Cotterchio M, Boucher BA, Manno M, Gallinger S, Okey AB, Harper PA. Red Meat Intake,
Doneness, Polymorphisms in Genes that Encode Carcinogen-Metabolizing Enzymes, and
Colorectal Cancer Risk. Cancer epidemiology biomarkers and prevention 2008;17:3098-107.
Coussens LM, Werb Z. Inflammation and cancer. Nature 2002;420: 860–7.
Craig WJ, Mangels AR. Position of the American Dietetic Association: Vegetarian Diets.
Journal of the American Dietetic Association 2009;109: 1266-82.
Cross AJ, Sinha R. Meat-Related Mutagens/Carcinogens in the Etiology of Colorectal Cancer.
Environmental and Molecular Mutagenesis 2004;44:44–55.
Cross AJ, Ferrucci LM, Risch A, Graubard BI, Ward MH, Park Y et al. A Large Prospective
Study of Meat Consumption and Colorectal Cancer Risk: An Investigation of Potential
Mechanisms Underlying this Association. Cancer research 2010;70: 2406-14.
Cross AJ, Leitzmann MF, Gail MH, Hollenbeck AR, Schatzkin A, Sinha R. A prospective study
of red and processed meat intake in relation to cancer risk. PLoS medicine 2007;4:1973-84.
Cross AJ, Pollock JR, Bingham SA. Haem, not protein or inorganic iron is responsible for
endogenous intestinal n-nitrosation arising from red meat. Cancer Res 2003;63:2358-60.
CSS – Conseil Supérieur de la Santé. Recommandations nutritionnelles pour la Belgique.
Bruxelles: CSS; 2009. Avis n°8309.
Dannenberger D, Reichardt W, Danier J, Numberg K, Numberg G, Ender K. Investigations on
selected essential micronutrients in muscle of German pure and crossbred pigs.
Fleischwirtschaft 2007;87:90-3.
Davis ME, Lisowyj MP, Zhou L, Wisecarver JL, Gulizia JM, Shostrom VK et al. Induction of
Colonic Aberrant Crypts in Mice by Feeding Apparent N-Nitroso Compounds Derived From
Hot Dogs Nutrition and cancer. The international journal 2012;64:342-49.
de Abreu Silva EO, Marcadenti A. Higher Red Meat Intake May Be a Marker of Risk, Not a
Risk Factor Itself. Arch intern med 2009;169:1538-39.
de Boer J, Schosler H, Boersema JJ. Climate change and meat eating: An inconvenient
couple? Journal of Environmental Psychology 2013;33:1-8.
de Ciriano MG, Berasategi I, Navarro-Blasco I, Astiasaran I, Ansorena D. Reduction of sodium
and increment of calcium and omega-3 polyunsaturated fatty acids in dry fermented sausages:
effects on the mineral content, lipid profile and sensory quality. Journal of the Science of Food
and Agriculture 2013;93: 876-81.
De Geeter H. Vlees wordt ingedeeld in rood en wit vlees. Waarom? Nutrinews 2009;2:18-9.
De Henauw S, De Backer G. Nutrient and food intakes in selected subgroups of Belgian
adults. British Journal of Nutrition 1999;81:S37–S42.
de Kok TM, van Maanen JM. Evaluation of fecal mutagenicity and colorectal cancer risk.
Mutation Research 2000;463:53–101.
De Stefani E, Aune D, Boffetta P, Deneo-Pellegrini H, Ronco AL, Acosta G et al. Salted Meat
Consumption and the Risk of Cancer: a Multisite. Case-Control Study in Uruguay Asian
pacific. Journal of cancer prevention 2009;10 :853-7.
− 75−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
De Stefani E, Ronco AL, Boffetta P, Deneo-Pellegrini H, Correa P, Acosta G et al. Nutrientderived Dietary Patterns and Risk of Colorectal Cancer: a Factor Analysis in Uruguay Asian
pacific. Journal of cancer prevention 2012;13:231-5.
De Vriese S, Huybrechts I, Moreau M, Van Oyen H. De Belgische voedselconsumptiepeiling 1
– 2004. Wetenschappelijk Instituut Volksgezondheid: Afdeling Epidemiologie. Brussel: WIV;
2006.
Available from:
URL:<(http://www.iph.fgov.be/epidemio/epinl/foodnl/table04.htm)>
DellaValle CT, Daniel CR, Aschebrook-Kilfoy B, Hollenbeck AR, Cross AJ, Sinha R et al.
Dietary intake of nitrate and nitrite and risk of renal cell carcinoma in the NIH-AARP Diet and
Health Study. British Journal of Cancer 2013;108:205-12.
Demeyer D, De Smet S. Relative importance and profile of processed meat intake in relation
to colon cancer death rates in Europe Proc. 57th International Congress of Meat Science and
Technology Ghent-Belgium 2011;7-12.
Demeyer D. Positioning of foods in availability and consumption of dietary energy, in food
based dietary guidelines and in nutrient profiling: Belgium as a case study. 2008;21. Available
from:
URL:<http://www.fenavian.be/>
Demeyer D. Letter to the Editors: Balancing the risks and benefits of unprocessed and
processed red meat consumption for both consumers and the environment. Meat Science
2010;86:529-30.
Demeyer D, Honikel K, De Smet S. The World Cancer Research Fund report 2007: A
challenge for the meat processing industry. Meat science 2008;80:953-59.
Demeyer DI, De Smet S. The recommendation to limit or avoid consumption of processed
meat is justified because of the association with the incidence of colorectal cancer and justifies
the use of alternatives for nitrite in meat processing Nitric oxide. Biology and Chemistry
2010;23:150-1.
D'evoli L, Salvatore P, Lucarini M, Nicoli S, Aguzzi A, Gabrielli P et al. Nutritional value of
traditional Italian meat-based dishes: influence of cooking methods and recipe formulation.
International journal of food sciences and nutrition 2009;60:38-49.
Deziel NC, Buckley TJ, Sinha R, Abubaker S, Platz EA, Strickland PT. Comparability and
repeatability of methods for estimating the dietary intake of the heterocyclic amine contaminant
2-amino-1-methyl-6-phenylimidazo[4,5b]pyridine (PhIP). Food Additives and Contaminants
Part A. Chemistry Analysis Control Exposure & Risk Assessment 2012;29:1202-11.
Doolaege EH, Vossen E, Raes K, De Meulenaer B, Verhe R, Paelinck H et al. Effect of
rosemary extract dose on lipid oxidation, colour stability and antioxidant concentrations, in
reduced nitrite liver pates. Meat science 2012; 90:925-31.
dos Santos BA, Campagnol PC, Pacheco MT, Pollonio MA. Fructooligo-saccharides as a fat
replacer in fermented cooked sausages. International Journal of Food Science and
Technology 2012;047:1183-92.
Drabik-Markiewicz G, Van den Maagdenberg K, De Mey E, Deprez S, Kowalska T, Paelinck
H. Role of proline and hydroxyproline in N-nitrosamine formation during heating in cured meat.
Meat Science 2009;81:479–86.
Dundar A, Sarıçoban C, Yılmaz MT. Response surface optimization of effects of some
processing variables on carcinogenic/mutagenic heterocyclic aromatic amine (HAA) content in
cooked patties. Meat Science 2012;91: 325–33.
EFSA - European Food Safety Agency. Polycyclic Aromatic Hydrocarbons in Food [1] Scientific Opinion of the Panel on Contaminants in the Food Chain. The EFSA Journal
2008;724: 1-114.
Egeberg R, Olsen A, Christensen J, Halkjaer J, Jakobsen MU, Overvad K. Associations
between Red Meat and Risks for Colon and Rectal Cancer Depend on the Type of Red Meat
Consumed. Journal of Nutrition 2013;143: 464-72.
− 76−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Engemann A, Focke C, Humpf HU. Intestinal formation of N-nitroso compounds in the pig
cecum model. J Agric Food Chem. 2013;61:998-1005.
EC - European Commission. European Guidelines for Quality Assurance in Colorectal Cancer
Screening and Diagnosis - First Edition - Segnan N, Patnick J, von Karsa L. editors.
Luxembourg: Publications Office of the European Union. 2010.
EPIC - European Prospective Investigation into Cancer and Nutrition. 2012. Availible from:
URL : <http://epic.iarc.fr/keyfindings.php>
EPIC - European Prospective Investigation into Cancer and Nutrition. Food content of potential
carcinogens. 2012a. Availible from:
URL:< http://www.epic-spain.com/libro.html >
Faustman C, Sun Q, Mancini R, Suman SP. Myoglobin and lipid oxidation interactions:
Mechanistic bases and control. Meat Science 2010;86:86–94.
Ferguson LR. Meat and cancer. Meat science, 2010;84: 308-13.
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden
of cancer in 2008: Globocan 2008. International journal of cancer 2010;127:2893-917.
Ferrucci LM, Cross AJ, Gunter MJ, Ahn J, Mayne ST, Ma X et al. Xenobiotic Metabolizing
Genes, Meat-Related Exposures, and Risk of Advanced Colorectal Adenoma. J Nutrigenet
Nutrigenomics 2011;3:170–81.
Ferrucci LM, Sinha R, Huang WY, Berndt SI, Katki HA, Schoen RE et al. Meat consumption
and the risk of incident distal colon and rectal adenoma. British journal of cancer
2012;106:608-16.
Cox B, Debacker N, De Vriese S, Drieskens S, Huybrechts I, Moreau M et al. Food
Consumption Survey Interactive Analysis (NUTRIA), Unit of Epidemiology, Scientific Institute
of Public Health, Brussels, Belgium. 2004. Availible from:
URL: <(http://www.iph.fgov.be/epidemio/epien/PROG5.HTM) >
Frew E, Wolstenholme JL, Atkin W, Whynes DK. Estimating time and travel costs incurred in
clinic based screening: flexible sigmoidoscopy screening for colorectal cancer. J Med Screen
1999;6:119–23.
Freybler LA, Gray JI, Asghar A, Booren AM, Pearson AM, Buckley DJ. Nitrite Stabilization of
Lipids In Cured Pork Meat Science 1993;33:85-96.
Fu ZM, Shrubsole MJ, Smalley WE, Wu HY, Chen Z, Shyr Y et al. Association of Meat Intake
and Meat-Derived Mutagen Exposure with the Risk of Colorectal Polyps by Histologic Type.
Cancer prevention research 2011;4:1686-97.
Fung KYC, Ooi CC, Zucker MH, Lockett T, Williams DB, Cosgrove LJ, Topping DL.
Colorectal Carcinogenesis: A Cellular Response to Sustained Risk Environment . International
Journal of Molecular Sciences 2013;14:13525-41.
Fung TT, Hu FB, Schulze M, Pollak M, Wu TY, Fuchs CS et al. A dietary pattern that is
associated with C-peptide and risk of colorectal cancer in women. Cancer causes and control
2012;23: 959-65.
Fung TT, Hu FB, Wu KN, Chiuve SE, Fuchs CS, Giovannucci E. The Mediterranean and
Dietary Approaches to Stop Hypertension (DASH) diets and colorectal cancer. American
journal of clinical nutrition 2010;92:1429-35.
Gaard M, Tretli S, Loken EB. Dietary factors and risk of colon cancer: A prospective study of
50,535 young Norwegian men and women. European Journal of Cancer Prevention 1996; 5:
445-454.
Garnett T. Food sustainability: problems, perspectives and solutions. Proceedings of the
Nutrition Society 2013;72:29-39.
Gay LJ, Mitrou PN, Keen J, Bowman R, Naguib A, Cooke J et al. Dietary, lifestyle and
clinicopathological factors associated with APC mutations and promoter methylation in
colorectal cancers from the EPIC-Norfolk study. Journal of Pathology 2012;228: 405-15.
Geissler C, Singh M. Iron, Meat and Health Nutrients 2011;3: 283-316.
− 77−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Gerber N, Brogioli R, Hattendorf B, Scheeder MR, Wenk C, Gunther D. Variability of selected
trace elements of different meat cuts determined by ICP-MS and DRC-ICPMS.
Animal 2009;3:166-72.
Gheisari HR, Motamedi H. Chloride salt type/ionic strength and refrigeration effects on
antioxidant enzymes and lipid oxidation in cattle, camel and chicken meat. Meat Science
2010;86:377-83.
Gilsing AM, Berndt SI, Ruder EH, Graubard BI, Ferrucci LM, Burdett L et al. Meat-related
mutagen exposure, xenobiotic metabolizing gene polymorphisms and the risk of advanced
colorectal adenoma and cancer. Carcinogenesis 2012;33:1332-39.
Gilsing AM, Weijenberg MP, Hughes LA, Ambergen T, Dagnelie PC, Goldbohm RA et al.
Longitudinal Changes in BMI in Older Adults Are Associated with Meat Consumption
Differentially, by Type of Meat Consumed. Journal of nutrition 2012a;142:340-9 .
Girard H, Butler LM, Villeneuvea L, Millikan RC, Sinha R, Sandler RS et al.
UGT1A1 and UGT1A9 functional variants, meat intake, and colon cancer,among Caucasians
and African-Americans Mutation. Research 2008;644:56–63.
Goldman R, Shields PG. Food Mutagens. J. Nutr. 2003;133:965S–73S.
Gonzalez-Gross M, Valtuena J, Moreno LA, Ferrari M, Kersting M, De Henauw S et al. Vitamin
D status among adolescents in Europe: the Healthy Lifestyle in Europe by Nutrition in
Adolescence study. British journal of nutrition 2012;107:755-64.
Gorelik S, Kanner J, Schurr D, Kohen R. A rational approach to prevent postprandial
modification of LDL by dietary polyphenols. Journal of Functional Foods 2013;5:163-9.
Gottschalg E, Scott GB, Burns PA, Shuker DE. Potassium diazoacetate-induced p53
mutations in vitro in relation to formation of O6-carboxymethyl- and O6-methyl-20deoxyguanosine DNA adducts: relevance for gastrointestinal cancer. Carcinogenesis
2007;28:356–62.
Goutefongea R, Cassens RG, Woolford G. Distribution of sodium nitrite in adipose tissue
during curing. Journal of Food Science 1977;42:1637–41.
Gratz SW, Wallace RJ, El-Nezami HS. Recent perspectives on the relations between fecal
mutagenicity, genotoxicity, and diet Front. Pharmacol. 2011;2:1-9.
Greenfield H, Arcot J, Barnes JA., Cunningham J, Adorno P, Stobaus T et al. Nutrient
composition of Australian retail pork cuts 2005/2006. Food Chemistry 2009;117:721–30.
Grivennikov SI, Greten FR, Karin M. Immunity, Inflammation, and Cancer : the good, the bad
and the ugly. Cell 2010;140:883-99.
Gunter MJ, Probst-Hensch NM, Cortessis VK, Kulldorff M, Haile RW, Sinha R. Meat intake,
cooking-related mutagens and risk of colorectal adenoma in a sigmoidoscopy-based casecontrol study. Carcinogenesis 2005;26:637-42.
Halkjaer J, Olsen A, Overvad K, Jakobsen MU, Boeing H, Buijsse B et al. Intake of total animal
and plant protein and subsequent changes in weight or waist circumference in European men
and women: the Diogenes project International. Journal of obesity 2011;35:1104-13.
Hall MN, Chavarro JE, Lee IM, Willett WC, Ma J. A 22-year prospective study of fish, n-3 fatty
acid intake, and colorectal cancer risk in men. Cancer epidemiology biomarkers & prevention
2008;17:1136-43.
Halliwell B, Gutteridge JM. Review article : Oxygen toxicity, oxygen radicals, transition metals
and disease. J Biochem 1984;219:1-14.
Haorah J, Zhou L, Wang XJ, Xu GP, Mirvish SS. Determination of total N-nitroso compounds
and their precursors in frankfurters, fresh meat, dried salted fish, sauces, tobacco, and
tobacco smoke particulates. Journal of agricultural and food chemistry 2001;49:6068-78.
Hara A , Sasazuki S, Inoue M, Iwasaki M, Shimazu T, Sawada N et al. Zinc and heme iron
intakes and risk of colorectal cancer: a population-based prospective cohort study in Japan.
American Journal of Clinical Nutrition 2012;96:864-73.
Hartnett L, Egan LJ. Inflammation, DNA methylation and colitis-associated cancer.
Carcinogenesis 2012;33:723-31.
− 78−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Hasan N, Pollack A, Cho I. Infectious Causes of Colorectal Cancer. Infect Dis Clin N Am
2010;24:1019–39.
GR - Health Council of the Netherlands. Guidelines for a Healthy Diet: the Ecological
Perspective. The Hague: GR; 2011.
Hebels DG, Sveje KM, de Kok MC, van Herwijnen MH, Kuhnle GG, Engels LG et al. Red
meat intake-induced increases in fecal water genotoxicity correlate with pro-carcinogenic gene
expression changes in the human colon. Food and Chemical Toxicology 2012;50:95-103.
Hebels DG, Brauers KJ, van Herwijnen MH, Georgiadis PA, Kyrtopoulos SA, Kleinjans JC.
Time-series analysis of gene expression profiles induced by nitrosamides and nitrosamines
elucidates modes of action underlying their genotoxicity in human colon cells. Toxicology
letters 2011;207:232-41.
Hedlund M, Padler-Karavani V, Varki NM, Varki A. Evidence for a human-specific mechanism
for diet and antibody-mediated inflammation in carcinoma progression. Proceedings of the
national academy of sciences of the United States of America 2008;105:18936-41.
Heinz G, Hautzinger. Meat processing technology for small-to medium-scale producers. Food
and Agriculture Organization of the United Nations - Regional office for Asia and the pacific
Bangkok
FAO
2010
ISBN:
978-974-7946-99-4.
Available
from:
URL:<http://www.fao.org/docrep/010/ai407e/AI407E00.htm>
Hentze MW, Muckenthaler MU, Galy B, Camaschella C. Two to Tango: Regulation of
Mammalian Iron. Metabolism Cell 2010;142:24-38.
Hermesch S, Jones RM. Genetic parameters for haemoglobin levels in pigs and iron content in
pork. Animal 2012;6:1904-12.
Higgins JA, Brown IL. Resistant starch: a promising dietary agent for the prevention/treatment
of inflammatory bowel disease and bowel cancer. Current Opinion in Gastroenterology
2013;29:190-4.
HGR - Hoge Gezondheidsraad. Voedingsaanbevelingen voor België.
Brussel: HGR; 2009. Advies nr. 8309.
Hofmann JN, Liao LM, Strickland P, Shu XO, Yang G, Ji BT, Li HL,Rothman N, Kamangar,
Gao YT, Zheng W, Chow WH.Polycyclic aromatic hydrocarbons: determinants of urinary 1hydroxypyrene glucuronide concentration and risk of colorectal cancer in the Shanghai
Women's Health Study BMC Cancer 2013; 13: 282.
Hogg N. Red meat and colon cancer: Heme proteins and nitrite in the gut. A commentary on
“Diet-induced endogenous formation of nitroso compounds in the GI tract”. Free Radical
Biology and Medicine 2007;43:1037-39.
Holtrop G, Johnstone AM, Fyfe C, Gratz SW. Diet Composition is Associated with
Endogenous Formation of N-Nitroso Compounds in Obese Men. Journal of Nutrition
2012;142:1652-58.
Honikel KO. The use and control of nitrate and nitrite for the processing of meat products.
Meat Science 2008;78:68-76.
Hord NG, Tang YP, Bryan NS. Food sources of nitrates and nitrites: the physiologic context for
potential health benefits. American journal of clinical nutrition 2009;90:1-10.
Hu JF, La Vecchia C, DesMeules M, Negri E, Mery L. Meat and fish consumption and cancer
in Canada. Nutrition and cancer - International Journal 2008;60:313-24.
Hu JF, La Vecchia C, Morrison H, Negri E, Mery L. Salt, processed meat and the risk of
cancer. European Journal of cancer prevention 2011;20:132-39.
Huang T, Yang B, Zheng JS, Li GP, Wahlqvist ML, Li D. Cardiovascular Disease Mortality
and Cancer Incidence in Vegetarians: A Meta-Analysis and Systematic Review. Annals of
nutrition and metabolism 2012;60: 233-40.
Hughes R , Cross AJ , Pollock JR, Bingham S. Dose-dependent effect of dietary meat on
endogenous colonic N-nitrosation. Carcinogenesis 2001; 22:199-202.
Hunt JR. Bioavailability of iron, zinc, and other trace minerals from vegetarian diets. Am J Clin
Nutr 2003;78:633S–9S.
− 79−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Hurrell R, Egli I. Iron bioavailability and dietary reference values. Am J of clinical nutrition
2010;91:1461S-67S.
Hutter CM, Chang-Claude J, Slattery ML, Pflugeisen BM, Lin Y, Duggan D et al.
Characterization of Gene-Environment Interactions for Colorectal Cancer Susceptibility Loci.
Cancer research 2012;72:2036-44.
Huxley RR, Ansary-Moghaddam A, Clifton P, Czernichow S, Parr CL, Woodward M. The
impact of dietary and lifestyle risk factors on risk of colorectal cancer: A quantitative overview
of the epidemiological evidence. Int J Cancer 2009;125:171-80.
Huybrechts I, Lin Y, De Keyzer W, Matthys C, Harvey L, Meirhaeghe A et al. Intake and
dietary sources of haem and non-haem iron in Flemish preschoolers. European Journal of
Clinical Nutrition 2012;66:806-12.
IJssennagger N, de Wit N, Muller M, van der Meer R. Dietary Heme-Mediated PPAR alpha
Activation Does Not Affect the Heme-Induced Epithelial Hyperproliferation and Hyperplasia in
Mouse Colon. PLos One 2012;7:Article Number: e43260.
IJssennagger N, Derrien M, van Doorn GM, Rijnierse A, van den Bogert B, Müller M et al.
Dietary Heme Alters Microbiota and Mucosa of Mouse Colon without Functional Changes in
Host-Microbe Cross-Talk. PLoS One 2012b;7: e49868.
IJssennagger N, Rijnierse A, de Wit NJW, Boekschoten MV, Dekker J, Schonewille A,Müller
M, Van der Meer R. Dietary heme induces acute oxidative stress, but delayed cytotoxicity and
compensatory hyperproliferation in mouse colon. Carcinogenesis 2013 ;34 (7):1628-35.
Ince M, Yaman M. High Performance Liquid Chromatography-Mass Spectrometry for
Determination of Benzo[a]pyrene in Grilled Meat Foods. Asian J. of Chemistry 2012;24:339195.
IARC - International Agency for Research on Cancer. IARC monographs on the evaluation of
carcinogenic risk to humans. Some naturally occurring substances: Food items and
constituents. Heterocyclic aromatic amines and mycotoxins 1993;Vol. 56. Available from:
URL:<http://www.iarc.fr/en/publications/list/monographs/>
Itzkowitz SH, Yio XY. Inflammation and cancer - IV. Colorectal cancer in inflammatory bowel
disease: the role of inflammation. Am J of Physiology-Gastrointestinal and Liver Physiology
2004;287:G7-G17.
Izumi K, Cassens RG, Greaser MI. Reaction of nitrite with ascorbic-acid and its significant role
in nitrite-cured food. Meat Science 1989;26:141-53.
Jägerstad M, Skog K. Genotoxicity of heat-processed foods. Mutation Research
2005;574:156–72.
Jakszyn P, Agudo A, Ibáñez R, García-Closas R, Pera G, Amiano P et al. Development of a
Food Database of Nitrosamines, Heterocyclic Amines, and Polycyclic Aromatic Hydrocarbons.
J Nutr 2004;134:2011–14.
Jeffery IB, O'Toole PW. Diet-Microbiota Interactions and Their Implications for Healthy Living.
Nutrients 2013;5:234-52.
Jiang H, Tang YP, Garg HK, Parthasarathy DK, Torregrossa AC, Hord NG et al.
Concentration- and stage-specific effects of nitrite on colon cancer cell lines. Nitric OxideBiology and Chemistry 2012;26:SI267-73.
Johnson CM, Wei CM, Ensor JE, Smolenski DJ, Amos CI, Levin B, Berry DA. Meta-analyses
of colorectal cancer risk factors Cancer Causes & Control 2013;56:1207-1222.
Joosen AM, Kuhnle GG, Aspinall SM, Barrow TM, Lecommandeur E, Azqueta A et al. Effect
of processed and red meat on endogenous nitrosation and DNA damage. Carcinogenesis
2009;30:1402-07.
Joosen AM, Lecommandeur E, Kuhnle GG, Aspinall SM, Kap L, Rodwell SA. Effect of dietary
meat and fish on endogenous nitrosation, inflammation and genotoxicity of faecal water.
Mutagenesis 2010;25:243-47.
Jung K, Lee K, Park J, Dong A, Shin HS. Influence of Fructooligosaccharides and Garlic on
Formation of Heterocyclic Amines in Fried Ground Beef Patties. Food science and
biotechnology 2010;19:1159-64.
− 80−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Kabat GC, Miller AB, Jain M, Rohan TE. A cohort study of dietary iron and heme iron intake
and risk of colorectal cancer in women. British journal of cancer 2007;97:118-22.
Kanazawa K, Ashida H. Dietary hydroperoxides of linoleic acid decompose to aldehydes in
stomach before being absorbed into the body. Biochimica et Biophysica Acta-Lipids and lipid
metabolism 1998;1393:349-61.
Kanner J. Dietary advanced lipid oxidation endproducts are risk factors to human health. Mol
Nutr Food Res 2007; 51:1094-101.
Kanner J. Oxidative processes in meat and meat products: quality implications. Meat Sci
1994;6:169–89.
Kanner J, Gorelik S, Roman S, Kohen R. Protection by Polyphenols of Postprandial Human
Plasma and Low-Density Lipoprotein Modification: The Stomach as a Bioreactor. J of
Agricultural and Food Chemistry 2012;60: 8790-96.
Karin M. Nuclear factor-kappaB in cancer development and progression. Nature
2006;441:431–36.
Kato I, Boleij A, Kortman GA, Roelofs R, Djuric Z, Severson RK et al. Partial Associations of
Dietary Iron, Smoking and Intestinal Bacteria with Colorectal Cancer Risk. Nutrition and
Cancer- an International Journal 2013;65:169-77.
Kazerouni N, Sinha R, Hsu CH, Greenberg A, Rothman N. Analysis of 200 food items for
benzo[a]pyrene and estimation of its intake in an epidemiologic study. Food and chemical
toxicology 2001;39:423-36.
Key TJ, Appleby PN, Spencer EA, Travis RC, Allen NE, Thorogood M et al. Cancer incidence
in British vegetarians. British journal of cancer 2009;101:192-197.
Kirkegaard H, Johnsen NF, Christensen J, Frederiksen K, Overvad K, Tjonneland A.
Association of adherence to lifestyle recommendations and risk of colorectal cancer: a
prospective Danish cohort study. BMJ 2010;341:Art. No. c5504.
Knekt P, Järvinen R, Dich J, Hakulinen T. Risk of colorectal and other gastro-intestinal cancers
after exposure to nitrate, nitrite and n-nitroso compounds: a follow-up study. Int J Cancer
1999;80:852–56.
Krebs NF, Hambidge KM. Complementary feeding: clinically relevant factors affecting timing
and composition. American journal of clinical nutrition 2006;85:639S-45S.
Krebs NF, Mazariegos M, Chomba E, Sami N, Pasha O, Tshefu A et al. Randomized
controlled trial of meat compared with multimicronutrient-fortified cereal in infants and toddlers
with high stunting rates in diverse settings. American Journal of Clinical Nutrition
2012a;96:840-47.
Krebs NF, Mazariegos M, Tshefu A, Bose C, Sami N, Chomba E et al. Meat consumption is
associated with less stunting among toddlers in four diverse low-income settings. Food and
nutrition bulletin 2011;32:185-91.
Krebs NF, Westcott JE, Culbertson DL, Sian L, Miller LV, Hambidge KM. Comparison of
complementary feeding strategies to meet zinc requirements of older breastfed infants.
American Journal of Clinical Nutrition 2012;96:30-5.
Kuhnle GG, Story GW, Reda T, Mani AR, Moore KP, Lunn JC et al. Diet-induced endogenous
formation of nitroso compounds in the GI tract Free. Radical Biology & Medicine
2007;43:1040–47.
Kumar TV, Ramji S. Effect of Zinc Supplementation on Growth in Very Low Birth Weight
Infants. Journal of tropical pediatrics 2012;58:50-4.
Kunitsugu I, Okuda M, Sugiyama S, Yoshitake N, Tanizawa Y, Sasaki S et al. Meat intake
frequency and anemia in Japanese children and adolescents. Nursing & Health Sciences
2012;14:197-203.
Kurotani K, Budhathoki S, Joshi AM, Yin GA, Toyomura K, Kono S et al. Dietary patterns and
colorectal cancer in a Japanese population: The Fukuoka Colorectal Cancer Study. British
journal of nutrition 2010;104:1703-11.
− 81−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Küry S, Buecher B, Robiou-du-Pont S, Scoul C, Sébille V, Colman H et al. Combinations of
cytochrome P450 gene polymorphisms enhancing the risk for sporadic colorectal cancer
related to red meat consumption. Cancer Epidemiol Biomarkers 2007;Prev16:1460–67.
Lagiou P, Trichopoulou A, Henderickx HK, Kelleher C, Leonhauser IU, Moreiras O et al.
Household budget survey nutritional data in relation to mortality from coronary heart disease,
colorectal cancer and female breast cancer in European countries. European journal of clinical
nutrition 1999;53:328-32.
Lambrinoudaki I, Ceasu I, Depypere H, Erel T, Rees M, Schenck-Gustafsson K et al. EMAS
position statement: Diet and health in midlife and beyond. Maturitas 2013;4:99-104.
Landi D, Gemignani F, Naccarati A, Pardini B, Vodicka P, Vodickova L, et al. Polymorphisms
within micro-RNA-binding sites and risk of sporadic colorectal cancer. Carcinogenesis
2008;29:579–84.
Landi D, Moreno V, Guino E, Vodicka P, Pardini B, Naccarati A et al. Polymorphisms
affecting micro-RNA regulation and associated with the risk of dietary-related cancers: A
review from the literature and new evidence for a functional role of rs17281995 (CD86) and
rs1051690 (INSR), previously associated with colorectal cancer mutation researchfundamental and molecular mechanisms of mutagenesis 2011;717:109-15.
Lang T, Barling D. Nutrition and sustainability: an emerging food policy discourse Proceedings
of the Nutrition Society 2013;72:1-12.
Lanza E, Schatzkin A, Daston C, Corle D, Freedman L, Ballard-Barbash R et al.
Implementation of a 4-y, high-fiber, high-fruit-and-vegetable, low-fat dietary intervention:
results of dietary changes in the Polyp Prevention Trial. American J of Clinical Nutrition
2001;74:387-401.
Larsson SC, Wolk A. Meat consumption and risk of colorectal cancer: a meta- analysis of
prospective studies. International Journal of Cancer 2006;119:2657-64.
Larsson SC, Rafter J, Holmberg L, Bergkvist L, Wolk A. Red meat consumption and risk of
cancers of the proximal colon, distal colon and rectum: The Swedish Mammography Cohort.
Int J Cancer 2005;113:829–34.
Latvala T, Niva M, Makela J, Pouta E, Heikkila J, Kotro J et al. Diversifying meat consumption
patterns: Consumers' self-reported past behaviour and intentions for change. Meat Science
2012;92:71-7.
Le Leu R, Conlon M, Winter J, Humphreys K, Michael M, Hu Y et al. Effect of high red meat
intake and resistant starch in humans on risk factors for colorectal cancer. Journal of
Gastroenterology and Hepatology 2012;27: 24-5.
Le Marchand L, Hankin JH, Pierce LM, Sinha R, Nerurkar PV, Franke AA et al. Well-done red
meat, metabolic phenotypes and colorectal cancer in Hawaii. Mutation Research 2002;506–
07: 205–14.
Lecerf JM. Meat and human health: excess and errors. Bulletin de l’Academie Nationale de
Médecine 2011;195:1801-12.
Lecerf JM. Cooking and cancer: why not? Correspondances en Metabolismes Hormones.
Diabetes et Nutrition 2012;16 :155-60.
Lee DH, Anderson KE, Harnack LJ, Folsom AR, Jacobs DR. Heme iron, zinc, alcohol
consumption, and colon cancer: Iowa Women's Health Study. Journal of the national cancer
institute 2004;96:403-07.
Lee JE, Chan AT. Fruit, Vegetables, and Folate: Cultivating the Evidence for Cancer
Prevention. Gastroenterology 2011;41:16-20.
Lee SA, Shu XO, Yang G, Li HL, Gao YT, Zheng W. Animal Origin Foods and Colorectal
Cancer Risk: A Report From the Shanghai Women's Health Study Nutrition and cancer.
International journal 2009;61:194-205.
Lenoir-Wijnkoop I, Jones PJ, Uauy R, Segal L, Milner J. Nutrition economics - food as an ally
of public health. British journal of Nutrition 2013;109:777-84.
− 82−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Leuratti C, Watson MA, Deag EJ, Welch A, Singh R, Gottschalg E et al. Detection of
malondialdehyde DNA adducts in human colorectal mucosa: Relationship with diet and the
presence of adenomas. Cancer epidemiology biomarkers & prevention 2002;11:267-73.
Lewin MH, Bailey N, Bandaletova T, Bowman R, Cross AJ, Pollock J et al. Red meat
enhances the colonic formation of the DNA adduct O6-carboxymethyl guanine: implications for
colorectal cancer risk. Cancer Research 2006;66:1859-65.
Li FY, Lai MD. Colorectal cancer, one entity or three. Journal of Zhejiang university
2009;10:219-29.
Li L, Shao JH, Zhu XD, Zhou GH, Xu XL. Effect of plant polyphenols and ascorbic acid on lipid
oxidation residual nitrite and N-nitrosamines formation in dry-cured sausage International
Journal of Food Science And Technology 2013; 48: 1157-1164.
Li L, Wang P, Xu XL, Zhou, GH. Influence of Various Cooking Methods on the Concentrations
of Volatile N-Nitrosamines and Biogenic Amines in Dry-Cured Sausages. Journal of Food
Science 2012;77:C560-C65.
Li Z, Henning SM, Zhang Y, Rahnama N, Zerlin A, Thames G et al. Decrease of postprandial
endothelial dysfunction by spice mix added to high-fat hamburger meat in men with Type 2
diabetes mellitus. Diabet. Med. 2013;30:590–95.
Li ZP, Henning SM, Zhang YJ, Zerlin A, Li LY, Gao K et al. Antioxidant-rich spice added to
hamburger meat during cooking results in reduced meat, plasma, and urine malondialdehyde
concentrations. American journal of clinical nutrition 2010;91:1180-84.
Liang PS, Chen T-Y, Giovannucci E. Cigarette smoking and colorectal cancer incidence and
mortality: Systematic review and meta-analysis. Int. J. Cancer 2009;124:2406–15.
Lim DG, Sweeney S, Bloodsworth A, White CR, Chumley PH, Krishna NR et al. Nitrolinoleate,
a nitric oxide-derived mediator of cell function: Synthesis, characteri-zation, and vasomotor
activity. Proceedings of the national academy of sciences of the United States of America
2002;99:15941–46.
Lin Y, Bolca S, Vandevijvere S, De Vriese S, Mouratidou T, De Neve M et al. Plant and animal
protein intake and its association with overweight and obesity among the Belgian population.
British journal of nutrition 2011;105:1106-16.
Linseisen J, Kesse E, Slimani N, , Bueno-de-Mesquita HB, Ocke MC, Skeie G et al. Meat
consumption in the European Prospective Investigation into Cancer and Nutrition (EPIC)
cohorts: results 24-hour dietary recalls. Public Health Nutrition 2002;5:SI1243-58.
Linseisen J, Rohrmann S, Norat T, Gonzalez CA, Iraeta MD, Gomez PM et al. Dietary intake
of different types and characteristics of processed meat which might be associated with cancer
risk – results from the 24-hour diet recalls in the European Prospective Investigation into
Cancer and Nutrition (EPIC). Public Health Nutrition 2006; 9:449–64.
Liu F, Yuan D, Wei YG, Wang WT, Yan LN, Wen TF et al. Systematic Review and MetaAnalysis of the Relationship between EPHX1 Polymorphisms and Colorectal Cancer Risk.
PLos One 2012a;7: e43821.
Liu JX, Ding DP, Wang XX, Chen YZ, Li R, Zhang Y et al. N-Acetyltransferase Polymorphism
and Risk of Colorectal Adenoma and Cancer: A Pooled Analysis of Variations from 59 Studies.
PLos One 2012; 7:e42797.
Loh YH, Jakszyn P, Luben RN, Mulligan AA, Mitrou PN, Khaw KT. N-nitroso compounds and
cancer incidence: the European Prospective Investigation into Cancer and Nutrition (EPIC)–
Norfolk Study. Am J Clin Nutr 2011;93:1053–61.
Lombardi-Boccia G, Lanzi S, Aguzzi A. Aspects of meat quality: trace elements and B vitamins
in raw and cooked meats. Journal of Food Composition and Analysis 2005;18:39–46.
Lombardi-boccia G, Martinez-dominguez B, Aguzzi A. Total Heme and Non-heme Iron in Raw
and Cooked Meats. Journal of food science 2002;67:1738-41.
López-Alonso M, García-Vaquero M, Benedito JL, Castillo C, Miranda M. Trace mineral
status and toxic metal accumulation in extensive and intensive pigs in NW. Spain Livestock
Science 2012;146:47–53.
− 83−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
López-Alonso M, Miranda M, Castillo C, Hernández J, García-Vaquero M, Benedito JL. Toxic
and essential metals in liver, kidney and muscle of pigs at slaughter in Galicia. Food Additives
and Contaminants 2007;24:943-54.
Lorrain B, Dangles O, Genot C, Dufour C. Chemical Modeling of Heme-Induced Lipid
Oxidation in Gastric Conditions and Inhibition by Dietary Polyphenols. J Agric Food Chem
2010;58:676–83.
Lund EK, Belshaw NJ, Elliott GO, Johnson IT. Recent advances in understanding the role of
diet and obesity in the development of colorectal cancer. Proceedings of the nutrition society
2011;70:194-204.
Lunn JC, Kuhnle G, Mai V, Frankenfeld C, Shuker DE, Glen RC et al. The effect of haem in
red and processed meat on the endogenous formation of N-nitroso compounds in the upper
gastrointestinal tract. Carcinogenesis 2007;28:685-90.
Macdiarmid JI, Kyle J, Horgan GW, Loe J, Fyfe C, Johnstone A et al. Sustainable diets for the
future: can we contribute to reducing greenhouse gas emissions by eating a healthy diet?
American Journal of Clinical Nutrition 2012;96:632-9.
Magalhaes B, Peleteiro B, Lunet N. Dietary patterns and colorectal cancer: systematic review
and meta-analysis. European journal of cancer prevention 2012;21:15-23.
Major JM, Cross AJ, Doubeni CA, Park Y, Lian M, Hollenbeck AR et al. Socioeconomic
deprivation impact on meat intake and mortality: NIH-AARP Diet and Health Study. Cancer
causes and control 2011;22:1699-707.
Mann J. Evidence-based nutrition: Does it differ from evidence-based medicine? Annals of
Medicine 2010;42:475–86.
Markowitz SD, Bertagnolli MM. Molecular Origins of Cancer: Molecular Basis of Colorectal
Cancer. New England Journal of Medicine 2009;361:2449-60.
Marnett LJ, Plastaras JP. Review : Endogenous DNA damage and mutation. Trends in
Genetics 2001;17:214–21.
Marnett LJ. Inflammation and Cancer: Chemical Approaches to Mechanisms, Imaging.
Journal of Organic Chemistry 2012;77:5224-38.
Massey RC, Key PE, Mallett AK, Rowland IR. An investigation of the endogenous formation of
apparent total N-nitroso compounds in conventional microflora and germ-free rats. Food Chem
Toxicol. 1988;26: 595-600.
Masuda M, Suzuki T, Friesen MD, Ravanat JL, Cadet J, Pignatelli B et al. Chlorination of
guanosine and other nucleosides by hypochlorous acid and myeloperoxidase of activated
human neutrophils - Catalysis by nicotine and trimethylamine. Journal of biological chemistry
2001;276:40486-96.
McAfee AJ, McSorley EM, Cuskelly GJ, Moss BW, Wallace JM, Bonham MP et al. Red meat
consumption: An overview of the risks and benefits. Meat science 2010;84:1-13.
McEvoy CT, Temple N, Woodside JV. Vegetarian diets, low-meat diets and health: a review.
Public Health Nutrition 2012;15:2287-94.
McMichael AJ, Powles JW, Butler CD, Uauy R. Food, livestock production, energy, climate
change, and health. Lancet 2007;370:1253-63.
McNeill S, Van Elswyk ME. Red meat in global nutrition. Meat Sci 2012;92:166-73.
Mei Q, Zhou DJ, Han JL, Lu H, Tang B. CYP1B1 Asn453Ser polymorphism and colorectal
cancer risk: a meta-analysis. Metabolism-Clinical And Experimental 2012;61:1321-29.
Meyer KA, Sijtsma FP, Nettleton JA, Steffen LM, Van Horn L, Shikany JM et al. Dietary
patterns are associated with plasma F-2-isoprostanes in an observational cohort study of
adults. Free Radical Biology and Medicine 2013;57:201-09.
Mhurchu CN, Capelin C, Dunford EK, Webster JL, Neal BC, Jebb SA. Sodium content of
processed foods in the United Kingdom: analysis of 44,000 foods purchased by 21,000
households. American journal of clinical nutrition 2011;93:594-600.
Miller PE, Lazarus P, Lesko SM, Cross AJ, Sinha R, Laio J et al. Meat-Related Compounds
and Colorectal Cancer Risk by Anatomical Subsite Nutrition and Cancer. International Journal
2013;65:202-26.
− 84−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Mills EW, Seetharaman K, Maretzki AN. A Nutribusiness Strategy for Processing and
Marketing Animal-Source Foods for Children. J. Nutr. 2007;137:1115–8.
Millward DJ, Garnett T. Food and the planet: nutritional dilemmas of greenhouse gas emission
reductions through reduced intakes of meat and dairy foods. Proceedings of the nutrition
society 2010;69:103-18.
Mirvish SS, Davis ME, Lisowyj MP, Gaikwadt NW. Effect of Feeding Nitrite, Ascorbate, Hemin,
and Omeprazole on Excretion of Fecal Total Apparent N-Nitroso Compounds in Mice.
Chemical research in toxicology 2008;21:2344-51.
Mirvish SS, Haorah J, Zhou L, Hartman M, Morris CR, Clapper ML. N-Nitroso compounds in
the gastrointestinal tract of rats and in the feces of mice with induced colitis or fed hot dogs or
beef. Carcinogenesis 2003;24:595-6.
Mithril C, Dragsted LO, Meyer C, Blauert E, Holt MK, Astrup A. Guidelines for the New Nordic
Diet. Public Health Nutrition 2012;15:1941-47.
Moor HG. Colorectal Cancer: What Should Patients and Families Be Told to Lower the Risk of
Colorectal Cancer? Surgical oncology clinics of North America 2010;19:693- 710.
Morales-Irigoyen EE, Severiano-Perez P, Rodriguez-Huezo ME, Totosaus A. Textural,
physicochemical and sensory properties compensation of fat replacing in pork liver pate
incorporating emulsified canola oil. Food Science and Technology International 2012;8:41341.
Morita H, Yoshikawa H, Suzuki T, Hisamatsu S, Kato Y, Sakata R et al. Anti-microbial action
against verotoxigenic Escherichia coli O157 : H7 of nitric oxide derived from sodium nitrite.
Bioscience Biotechnology and Biochemistry 2004;68:1027-34.
Morita M, Le Marchand L, Kono S, Yin G, Toyomura K, Nagano J et al. Genetic
Polymorphisms of CYP2E1 and Risk of Colorectal Cancer: The Fukuoka. Colorectal Cancer
Study Cancer epidemiology biomarkers and prevention 2009;18:235-41.
Morrissey PA, Tichivangana JZ. The Antioxidant Activities of Nitrite and Nitrosylmyoglobin in
Cooked Meats. Meat Science 1985;14:175-90.
Mouloud M, Metro F, Goutefongea R, Dumont JP. Mass-spectrometric study of derivatives
formed by the reaction of oleic-acid with nitrite - some evidence for the formation of derivatives
nitrosubstituted on the alpha-position of the double-bond. Sciences Des Aliments
1992;12:371-82.
Mozaffarian D. Meat Intake and Mortality: Evidence for Harm, No Effect, or Benefit? Arch
intern med 2009;169:1537-38.
Mullie P, Godderis L, Clarys P. Determinants and nutritional implications associated with lowfat food consumption. Appetite 2012;58:34-8.
Murata M, Thanan R, Ma N, Kawanishi S. Role of nitrative and oxidative DNA damage in
inflammation-related carcinogenesis. J Biomed Biotechnol 2012:623019.
Murkovic M. Chemistry, formation and occurrence of genotoxic heterocyclic aromatic amines
in fried products. Eur J Lipid Sci Technol 2004;106:777–85.
Nakai H, Cassens RG, Greaser ML, Woolford G. Significance of the reaction of nitrite with
tryptophan. Journal of Food Science 1978;43:1857–60.
Navia JL, Byers T, Djordjevic D, Hentges E, King J, Klurfeld D et al. Integrating the Totality
of Food and Nutrition Evidence for Public Health Decision Making and Communication. Critical
reviews in food science and nutrition 2010;50:1:1-8.
Nebert DW, Ingelman-sundberg M, Daly AK. Genetic epidemiology of environmental toxicity
and cancer susceptibility: human allelic polymorphisms in drugmetabolizing enzyme genes,
their functional importance, and nomenclature issues. Drug metabolism reviews 1999;31:467–
87.
Nicolescu AC, Reynolds JN, Ross L, Barclay C, Thatcher GR. Organic Nitrites and NO:
Inhibition of Lipid Peroxidation and Radical Reactions. Chem Res Toxicol 2004;17:185-96.
Norat T, Bingham S, Ferrari P, Slimani N, Jenab M, Mazuir M et al. Meat, fish, and colorectal
cancer risk: The European prospective investigation into cancer and nutrition. Journal of the
national cancer institute 2005;97:906-16.
− 85−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Norat T, Lukanova A, Ferrari P, Riboli E. Meat consumption and colorectal cancer risk: Doseresponse meta-analysis of epidemiological studies. International Journal of Cancer
2002;98:241-56.
Nordgren A. Ethical Issues in Mitigation of Climate Change: The Option of Reduced Meat
Production and Consumption. Journal of Agricultural and Environmental ethics 2012;25:56384.
Ollberding NJ, Nomura AM, Wilkens LR, Henderson BE, Kolonel LN. Racial/ethnic differences
in colorectal cancer risk: the multiethnic cohort study. Int. J. Cancer 2011;129:1899–1906.
Ollberding NJ, Wilkens LR, Henderson BE, Kolonel LN, le Marchand L. Meat consumption,
heterocyclic amines and colorectal cancer risk: The Multiethnic. Cohort Study International
Journal of Cancer Early View 2012. Available from:
URL:<http://onlinelibrary.wiley.com/doi/10.1002/ijc.27546/pdf>
Olmedilla-Alonso B, Jimenez-Colmenero F, Sanchez-Muniz FJ. Development and assessment
of healthy properties of meat and meat products designed as functional foods. Meat Science
2013;95:919-30.
Ozden TA, Gokcay G, Issever H, Durmaz O, Sokucu S, Saner G. Serum and hair zinc levels
of infants and their mothers. Clinical Biochemistry 2012;45:753-57.
Pacolet J, De Coninck A, Hedebouw G, Cabus S, Spruytte N. De medische en niet-medische
kosten van kankerpatiënten - Studie in opdracht van de Vlaamse Liga tegen Kanker
gerealiseerd met de medewerking van de Christelijke Mutualiteit, het Universitair Ziekenhuis
Leuven en het Ziekenhuis Netwerk Antwerpen. Gepubliceerd door HIVA – Onderzoeksinstituut
voor Arbeid en Samenleving (K.U.Leuven). 2011. Availible from:
URL:<http://www.hiva.be>
Padidar S, Farquharson AJ, Williams LM, Kearney R, Arthur JR, Drew JE. High-Fat Diet Alters
Gene Expression in the Liver and Colon: Links to Increased Development of Aberrant Crypt
Foci. Digestive Diseases and Sciences 2012;57:1866-74.
Painter RG, Bonvillain RW, Valentine VG, Lombard GA, LaPlace SG, Nauseef WM et al. The
role of chloride anion and CFTR in killing of Pseudomonas aeruginosa by normal and CF
neutrophils. Journal of Leukocyte Biology 2008;83:1345-53.
Pala V, Sieri S, Berrino F, Vineis P, Sacerdote C, Palli D et al. Yogurt consumption and risk of
colorectal cancer in the Italian European Prospective Investigation into Cancer and Nutrition
cohort. International Journal of Cancer 2011;129:2712-19.
Pan A, Sun Q, Bernstein AM, Schulze MB, Manson JE, Stampfer MJ et al. Red Meat
Consumption and Mortality - Results From 2 Prospective Cohort Studies. Archives of Internal
Medicine 2012;172:555-63.
Parasramka MA, Dashwood WM, Wang R, Abdelli A, Bailey GS, Williams DE, et al. MicroRNA
profiling of carcinogen-induced rat colon tumors and the influence of dietary spinach.
Molecular Nutrition and Food Research 2012; 56:1259-69.
Park SY, Murphy SP, Wilkens LR, Yamamoto JF, Sharma S, Hankin JH et al. Dietary patterns
using the food guide pyramid groups are associated with sociodemographic and lifestyle
factors: The multiethnic cohort study. Journal of Nutrition 2005;135:843-49.
Park Y, Leitzmann MF, Subar AF, Hollenbeck A, Schatzkin A. Dairy Food, Calcium, and Risk
of Cancer in the NIH-AARP. Diet and Health Study. Archives of Internal Medicine
2009;169:391-401.
Parkin DM. International Variation Oncogene 2004;23:6329- 40.
Parkin DM, Olsen AH, Sasieni P. The potential for prevention of colorectal cancer in the UK.
European Journal of Cancer Prevention 2009;18: 179-90.
Parnaud G, Corpet DE. Colorectal cancer - controversial role of meat consumption. Bulletin du
Cancer 1997;84:899-911.
Parnaud G, Pignatelli B, Peiffer G, Tache S, Corpet DE. Endogenous N-nitroso compounds,
and their precursors, present in bacon, do not initiate or promote aberrant crypt foci in the
colon of rats. Nutrition and Cancer-An International Journal 2000;38:74-80.
− 86−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Parr CL, Hjartaker A, Lund E, Veierod MB. Meat intake cooking methods and risk of proximal
colon distal colon and rectal cancer: The Norwegian Women and Cancer (NOWAC) cohort
study. International Journal of Cancer 2013; 133: 1153-1163.
Parthasarathy DK, Bryan NS. Sodium nitrite: The "cure" for nitric oxide insufficiency. Meat
Science 2012;92:SI274-79.
Paturi G, Nyanhanda T, Butts CA, Herath TD, Monro JA, Ansell J. Effects of Potato Fiber and
Potato-Resistant Starch on Biomarkers of Colonic Health in Rats Fed Diets Containing Red
Meat. Journal of Food Science 2012; 277:H216-23.
Pedersen M, Halldorsson TI, Autrup H, Brouwer A, Besselink H, Loft S et al. Maternal diet and
dioxin-like activity, bulky DNA adducts and micronuclei in mother-newborns. Mutation
research-fundamental and molecular mechanisms of mutagenesis 2012;734:12-1.
Pegg RB, Shahidi F, Fox Jr JB. Unraveling the chemical identity of meat pigments. Critical
Reviews in Food Science and Nutrition 1997;37: 561– 589
Peng H, Xie SK, Huang MJ, Ren DL. Associations of CYP2E1 rs2031920 and rs3813867
polymorphisms with colorectal cancer risk: a systemic review and meta-analysis. Tumor
Biology 2013; 34:2389-95.
Pennings B, Groen BBL, van Dijk JW, de Lange A, Kiskini A, Kuklinski M, Senden JMG, van
Loon LJC. Minced beef is more rapidly digested and absorbed than beef steak, resulting in
greater postprandial protein retention in older Men. American Journal of Clinical Nutrition
2013; 98:121-28.
Pérez-Cueto FJ, Verbeke W. Consumer implications of the WCRF's permanent update on
colorectal cancer. Meat Science 2012;90:977–8.
Phillips SM. Nutrient-rich meat proteins in offsetting age-related muscle loss. Meat Science
2012;92:SI174-8.
Pierre F, Freeman A, Tache S, Van der Meer R, Corpet DE. Beef meat and blood sausage
promote the formation of azoxymethane-induced mucin-depleted foci and aberrant crypt foci in
rat colons. Journal of Nutrition 2004;134:2711-16.
Pierre F, Peiro G, Tache S, Cross AJ, Gasc N, Gottardi G et al. New marker of colon cancer
risk associated with heme intake: 1,4-dihydroxynonane mercapturic acid. Cancer epidemiology
biomarkers and prevention 2006;15:2274-79.
Pierre FH, Santarelli RL, Allam O, Tache S, Naud N, Gueraud F et al. Freeze-dried ham
promotes azoxymethane-induced mucin-depleted foci and aberrant crypt foci in rat colon. Nutr
Cancer 2010;62:567-73.
Pöhlmann M, Hitzel A, Schwägele F, Speer K, Jira W. Contents of polycyclic aromatic
hydrocarbons (PAH) and phenolic substances in Frankfurter-type sausages depending on
smoking conditions using glow smoke. Meat Sci. 2012;90:176-84.
Pomerleau J, McKee M, Lobstein T, Knai C. The burden of disease attributable to nutrition in
Europe Public. Health Nutrition 2003;6:453–61.
Pou SA, Diaz MD, Osella AR. Applying multilevel model to the relationship of dietary patterns
and colorectal cancer: an ongoing case-control study in Cordoba, Argentina. European
Journal of Nutrition 2012;51: 755-64.
Powell TW, Lenton TM. Future carbon dioxide removal via biomass energy constrained by
agricultural efficiency and dietary trends Energy and Environmental Science 2012;5:8116-33.
Programme National Nutrition Santé. Nutrition & Prévention des cancers :des connaissances
scientifiques aux recommandations. France;2009. Available from :
URL :< http://www.hnpcc-lynch.com/INCa_brochure_pnns_nutrition160209.pdf>
Prynne CJ, Wagemakers JJ, Stephen AM, Wadsworth ME. Meat consumption after
disaggregation of meat dishes in a cohort of British adults in 1989 and 1999 in relation to diet
quality. European Journal of Clinical Nutrition 2009;63:660–66.
Puangsombat K, Gadgil P, Houser TA, Hunt MC, Scott SJ. Occurrence of heterocyclic amines
in cooked meat products. Meat science 2012;90:739-46.
− 87−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Purchas RW, Rutherfurd SM, Pearce PD, Vather R, Wilkinson BH. Cooking temperature
effects on the forms of iron and levels of several other compounds in beef semitendinosus
muscle. Meat Science 2004;68:201–7.
Qian J, Song ZF, Lv YX, Huang XF. CYP2E1 T7632A and 9-bp insertion polymorphisms and
colorectal cancer risk: a meta-analysis based on 4,592 cases and 5,918 controls. Tumor
Biology 2013; 34:2225-31
Qian SY, Buettner GR. Iron and dioxygen chemistry is an important route to initiation of
biological free radical oxidations: An electron paramagnetic resonance spin trapping study.
Free radical biology and medicine 1999; 26(11-12):1447-56.
Qiao L,Feng Y. Intakes of heme iron and zinc and colorectal cancer incidence: a metaanalysis of prospective studies. Cancer Causes & Control 2013; 24:1175-83.
Raes K, De Smet S & Demeyer D. Effect of dietary fatty acids on incorporation of long chain
polyunsaturated fatty acids and conjugated linoleic acid in lamb, beef and pork meat: a review.
Animal feed science and technology 2004;113:199-221.
Rainis T, Maor I, Lanir A, Shnizer S, Lavy A. Enhanced Oxidative Stress and Leucocyte
Activation in Neoplastic Tissues of the Colon. Dig Dis Sci 2007; 52:526–30.
Rakoff-Nahoum S, Medzhitov R. Innate immune recognition of the indigenous microbial flora.
Mucosal Immunol 2008;S10–S4.
Ramos A, Cabrera MC, Saadoun A. Bioaccessibility of Se, Cu, Zn, Mn and Fe, and heme iron
content in unaged and aged meat of Hereford and Braford steers fed pasture. Meat science
2012;91:116-24.
Randi G, Edefonti V, Ferraroni M, La Vecchia C, Decarli A. Dietary patterns and the risk of
colorectal cancer and adenomas. Nutrition reviews 2010;68:389-408.
Reedy J, Wirfalt E, Flood A, Mitrou PN, Krebs-Smith SM, Kipnis V et al. Comparing 3 Dietary
Pattern Methods-Cluster Analysis, Factor Analysis, and Index Analysis-With Colorectal Cancer
Risk. American Journal of Epidemiology 2010;171:479-87.
Rémond D, Machebeuf M, Yven C, Buffière C, Mioche L, Mosoni L et al. Postprandial wholebody protein metabolism after a meat meal is influenced by chewing efficiency in elderly
subjects. Am J Clin Nutr 2007;85:1286-92.
Rodriguez-Sanchez DG, Pacheco A,Garcia-Cruz MI,Gutierrez-Uribe JA ,Benavides-Lozano
JA, Hernandez-Brenes C . Isolation and Structure Elucidation of Avocado Seed (Persea
americana) Lipid Derivatives That Inhibit Clostridium sporogenes Endospore Germination.
Journal of Agricultural and Food Chemistry 2013;61:7403-11.
Rohrmann S, Overvad K, Bueno-de-Mesquita HB, Jakobsen MU, Egeberg R, Tjønneland A
et al. Meat consumption and mortality - results from the European Prospective Investigation
into Cancer and Nutrition. BMC Medicine 2013;11:63.
Rohrmann S, Hermann S, Linseisen J. Heterocyclic aromatic amine intake increases
colorectal adenoma risk: findings from a prospective European cohort study. American Journal
of Clinical Nutrition 2009;89:1418-24.
Rohr-Udilova NV, Stolze K, Sagmeister S, Nohl H, Schulte-Hermann R, Grasl-Kraupp B. Lipid
hydroperoxides from processed dietary oils enhance growth of hepatocarcinoma cells. Mol
Nutr Food Res 2008;52:352-59.
Romaguera D, Angquist L, Du HD, Jakobsen MU, Forouhi NG, Halkjaer J et al. Food
Composition of the Diet in Relation to Changes in Waist Circumference Adjusted for Body
Mass Index. PLoS ONE 2011;6:Article No e23384.
Rooke JA, Flockhart JF, Sparks NH. The potential for increasing the concentrations of
micronutrients relevant to human nutrition in meat, milk and eggs.The Journal of Agricultural
Science 2010;148:pp 603-14.
Rosato V, Bosetti C, Levi F, Polesel J, Zucchetto A, Negri E et al. Risk factors for young-onset
colorectal cancer. Cancer Causes and Control 2013;24:335-41.
Ross HD, Henion J, Babish J, Hotchkiss JH. Nitrosating Agents from the Reaction Between
Methyl Oleate and Dinitrogen Trioxide: Identification and Mutagenicity. Food Chemistry
1987;23:207-22.
− 88−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Rounds L, Havens CM, Feinstein Y, Friedman M, Ravishankar S.Concentration-dependent
inhibition of Escherichia coli O157:H7 and heterocyclic amines in heated ground beef patties
by apple and olive extracts, onion powder and clove bud oil. Meat Science 2013; 94: 461-467.
Ruder EH, Thiebaut AC, Thompson FE, Potischman N, Subar AF, Park Y et al. Adolescent
and mid-life diet: risk of colorectal cancer in the NIH-AARP Diet and Health Study. American
Journal of Clinical Nutrition 2011;94:1607-19.
Rywotycki R. Meat nitrosamine contamination level depending on animal breeding factors.
Meat Science 2003;65:669-75.
Rywotycki R. The effect of baking of various kinds of raw meat from different animal species
and meat with functional additives on nitrosamine contamination level. Food Chemistry
2007;101:540–48.
Saebo M, Skjelbred CF, Li KB, Lothe IM, Hagen PC, Johnsen E et al. CYP1A2 164 A -> C
polymorphism, cigarette smoking, consumption of well-done red meat and risk of developing
colorectal adenomas and carcinomas. Anticancer research 2008;28:2289-95.
Saffhill R, Margison GP, Oconnor PJ. Mechanisms of carcinogenesis induced by alkylatingagents 1985.
Sainani K. The Limitations of Statistical Adjustment. PM and R 2011;3:868-72.
Sanford KW, McPherson RA. Fecal Occult Blood Testing. Clin Lab Med 2009;29:523–41.
Santarelli RL, Naud N, Taché S, Guéraud F, Vendeuvre J-L, Zhou L et al. Calcium Inhibits
Promotion by Hot Dog of 1,2-Dimethylhydrazine-Induced Mucin-Depleted Foci in Rat Colon.
International Journal of Cancer 2013.
Santarelli RL ,Pierre F, Corpet DE. Processed meat and colorectal cancer: A review of
epidemiologic and experimental evidence. Nutrition and Cancer International Journal
2008;60:131-44.
Santarelli RL, Vendeuvre JL, Naud N, Tache S, Gueraud F, Viau M et al. Meat Processing and
Colon Carcinogenesis: Cooked, Nitrite-Treated, and Oxidized High-Heme Cured Meat
Promotes Mucin-Depleted Foci in Rats. Cancer Prevention Research 2010;3:852-64.
Satia JA, Tseng M, Galanko JA, Martin C & Sandler RS (2009) Dietary Patterns and Colon
Cancer Risk in Whites and African Americans in the North Carolina Colon Cancer Study
Nutrition and cancer-an international journal 61 (2) 179-193
Sato Y, Nakaya N, Kuriyama S, Nishino Y, Tsubono Y, Tsuji I. Meat consumption and risk of
colorectal cancer in Japan: The Miyagi cohort study. European Journal of Cancer Prevention
2006;15:211-18.
Scarborough P, Allender S, Clarke D, Wickramasinghe K, Rayner M. Modelling the health
impact of environmentally sustainable dietary scenarios in the UK European. Journal of
Clinical Nutrition 2012;66:710-15.
Schipper HM. Neurodegeneration with brain iron accumulation Clinical syndromes and
neuroimaging.
Biochimica
et
Biophysica
Acta-Molecular
Basis
of
Disease
2012;1822:SIPages:350-60.
Schmid A, Badertscher R, Scherrer D, Portmann R, Dubois S, Spahni M et al. Nutrient
composition of Swiss cured cooked meat. Fleischwirtschaft 2011;91:97-100.
Schönfeldt HC, Hall NG. Determining iron bio-availability with a constant heme iron value.
Journal of Food Composition and Analysis 2011;24:738–40.
Schönfeldt HC, Hall NG. Consumer education on the health benefits of red meat - A
multidisciplinary approach. Food Research International 2012;47:SI152-5.
Scientific Advisory Committee on Nutrition. Iron and Health Report UK;2010. Available from:
URL:<http://www.sacn.gov.uk/pdfs/sacn_iron and_health_report_web.pdf >
Selgas MD, Salazar P, Garcia ML. Usefulness of calcium lactate, citrate and gluconate for
calcium enrichment of dry fermented sausages. Meat science 2009;82:478-80.
Sesink AL, Termont DS, Kleibeuker JH, Van der Meer R. Red meat and colon cancer: The
cytotoxic and hyperproliferative effects of dietary heme. Cancer Research 1999;59:5704-09.
− 89−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Sesink AL, Termont DS, Kleibeuker JH, Van der Meer R. Red meat and colon cancer: dietary
haem-induced colonic cytotoxicity and epithelial hyperproliferation are inhibited by calcium.
Carcinogenesis 2001;22:1653-59.
Shahidi F, Rubin LJ, Wood DF. Control of lipid oxidation in cooked ground pork with
antioxidants and dinitrosyl ferrohemochrome. Journal of Food Science 1987;52:564-67.
Shaughnessy DT, Gangarosa LM, Schliebe B, Umbach DM, Xu ZL, MacIntosh B et al.
Inhibition of Fried Meat-Induced Colorectal DNA Damage and Altered Systemic Genotoxicity in
Humans by Crucifera, Chlorophyllin, and Yogurt. PLOS ONE 2011;6:Art.No.e18707.
Shena X, Zhoua J, Donga J, Dinga W, Wu J. Systematic Review with Meta-Analysis Dietary
intake of n-3 fatty acids and colorectal cancer risk: a meta-analysis of data from 489 000
individuals. British Journal of Nutrition 2012;108:1550-56.
Shin A, Joo J, Bak J, Yang HR, Kim J, Park S et al. Site-Specific Risk Factors for Colorectal
Cancer in a Korean Population. PLoS ONE 2011;8:Art.No.e23196.
Sindelar JJ, Milkowski AL. Human safety controversies surrounding nitrate and nitrite in the
diet Nitric Oxide. Biology and Chemistry 2012;26: SI259-66.
Sinha R, Graubard BI, Cross AJ, Leitzmann MF, Schatzkin A. In reply. Arch intern med
2009;169:1539.
Sinha R, Kulldorff M, Gunter MJ, Strickland P, Rothman N. Dietary Benzo[a]Pyrene Intake and
Risk of Colorectal Adenoma Cancer. Epidemiol Biomarkers Prev 2005;14:2030-4.
Sirota R, Gorelik S, Harris R, Kohen R, Kanner J. Coffee polyphenols protect human plasma
from postprandial carbonyl modifications Molecular Nutrition & Food Research 2013; 57: 916919.
Skibsted LH. Nitric oxide and quality and safety of muscle based foods. Nitric Oxide
2011;24:176–83.
Smith JS, Ameri F, Gadgil P. Effect of marinades on the formation of heterocyclic amines in
grilled beef steaks. Journal of Food Science 2008;73 :T100-T05.
Smolinska K & Paluszkiewicz P. Risk of colorectal cancer in relation to frequency and total
amount of red meat consumption. Systematic review and meta-analysis. Archives of Medical
Science 2010;6:605-10.
Spencer EA, Key TJ, Appleby PN, Dahm CC, Keogh RH, Fentiman IS et al. Meat, poultry and
fish and risk of colorectal cancer: pooled analysis of data from the UK dietary cohort
consortium. Cancer Causes and Control 2010;21:1417-25.
Squires J, Roebothan B, Buehler S, Sun ZY, Cotterchio M, Younghusband B et al. Pickled
meat consumption and colorectal cancer (CRC): a case-control study in Newfoundland and
Labrador. Cancer Causes and Control 2010;21:1513-21.
Steinberg P. Endogenously formed N-nitroso compounds: A new group of colon carcinogens
relevant to man? Ernahrungs-Umschau 2009;56:332-37.
Stoltzfus RJ. Defining Iron-Deficiency Anemia in Public Health Terms: A Time for Reflection. J.
Nutr. 2001;131: 565S–7S.
Stuff JR, Goh ET, Barrera SL, Bondy ML, Forman MR. Construction of an N-nitroso database
for assessing dietary intake. Journal of Food Composition and Analysis 2009;22S:S42–S47.
Sugimura T. Overview of carcinogenic heterocyclic amines. Mutation Research 1997;376:211–
19.
Sun WQ, Zhou GH, Xu XL, Peng ZQ. Studies on the structure and oxidation properties of
extracted cooked cured meat pigment by four spectra. Food Chemistry 2009;115:596–601.
Sun ZY, Liu L, Wang PP, Roebothan B, Zhao J, Dicks E et al. Association of total energy
intake and macronutrient consumption with colorectal cancer risk: results from a large
population-based case-control. Study in Newfoundland and Labrador and Ontario, Canada.
Nutrition Journal 2012;11:Art. No.18.
SHC – Superior Health Council & SciCom FASFC – Scientific Committee of the Federal
Agency for the Safety of the Food Chain. Joint advisory report. Reformulation of foodstuffs –
salt reduction. Brussels: SHC; 2012. Advisory report n°8663.
− 90−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Symons TB, Sheffield-Moore M, Wolfe RR, Paddon-jones D. A Moderate Serving of HighQuality Protein Maximally Stimulates Skeletal Muscle Protein Synthesis in Young and Elderly
Subjects. J Am Diet Assoc 2009;109:1582-86.
Szterk A, Roszko M, Malek K, Kurek M, Zbiec M, Waszkiewicz-Robak B. Profiles and
concentrations of heterocyclic aromatic amines formed in beef during various heat treatments
depend on the time of ripening and muscle type. Meat Science 2012;92:587-95.
Tabatabaei SM, Fritschi L, Knuiman MW, Boyle T, Iacopetta BJ, Platell C et al. Meat
consumption and cooking practices and the risk of colorectal cancer. European Journal of
clinical nutrition 2011;65:668-75.
Tabatabaei SM, Heyworth JS, Knuiman MW, Fritschi L. (2010) Dietary Benzo[a]pyrene Intake
from Meat and the Risk of Colorectal Cancer. Cancer Epidemiol Biomarkers Prev
2010;19:3182-84.
Takachi R, Tsubono Y, Baba K, Inoue M, Sasazuki S, Iwasaki M et al. Red meat intake may
increase the risk of colon cancer in Japanese, a population with relatively low red meat
consumption. Asia pacific journal of clinical nutrition 2011;20:603-12.
Takahashi M, Nishikawa A, Furukawa F, Hasegawa T, Hayashi Y. Dose-dependent promoting
effects of sodium chloride (NaCI) on rat glandular stomach carcinogenesis initiated with
Nmethyl-N'-nitro-N-nitrosoguanidine. Carcinogenesis 1994;15:1429-32.
Temme EH, van der Voet H, Roodenburg AJ, Bulder A, van Donkersgoed G, van Klaveren J.
Impact of foods with health logo on saturated fat, sodium and sugar intake of young Dutch
adults. Public health nutrition 2011;14:635-44.
Terzic J, Grivennikov S, Karin E, Karin M. Inflammation and Colon Cancer Gastroenterology
2010;138:2101-U119.
Thiebaud HP, Knize MG, Kuzmicky PA, Hsieh DP, Felton JS. Airborne mutagens produced by
frying beef, pork and a soy-based food. Food and chemical toxicology 1995;33:821-28.
Toden S, Belobrajdic DP, Bird AR, Topping DL, Conlon MA. Effects of Dietary Beef and
Chicken With and Without High Amylose Maize Starch on Blood Malondialdehyde,
Interleukins, IGF-I, Insulin, Leptin, MMP-2, and TIMP-2 Concentrations in Rats Nutrition and
cancer. International journal 2010; 62:454-65.
Toden S, Bird AR, Topping DL, Conlon MA. High red meat diets induce greater numbers of
colonic DNA double-strand breaks than white meat in rats: attenuation by high-amylose maize
starch. Carcinogenesis 2007;28:2355-62.
Tomovic VM, Petrovic LS, Tomovic MS, Kevresan ZS, Dzinic NR. Determination of mineral
contents of semimembranosus muscle and liver from pure and crossbred pigs in Vojvodina.
Food Chemistry 2011;124:342-48.
Tricker AR, Preussmann R. Carcinogenic n-nitrosamines in the diet - occurrence, formation,
mechanisms and carcinogenic potential. Mutation research 1991;259:277-89.
Tricker AR. N-nitroso compounds and man: sources of exposure, endogenous formation and
occurrence in body fluids. European Journal of Cancer prevention 1997;6:226-68.
Tudek B, Speina E. Oxidatively damaged DNA and its repair in colon. Carcinogenesis
Mutation Research-Fundamental and Molecular Mechanisms of Mutagenesis 2012;736:SI8292.
Tussing-Humphreys L, Pustacioglu C, Nemeth E, Braunschweig C. Rethinking Iron Regulation
and Assessment in Iron Deficiency, Anemia of Chronic Disease, and Obesity: Introducing
Hepcidin. Journal of the academy of nutrition and dietetics 2012;112:391-400.
Valencia-Martin JL, Galan I, Rodriguez-Artalejo F. The Association Between Alcohol
Consumption Patterns and Adherence to Food Consumption. Guidelines Alcoholism-Clinical
and experimental research 2011;35:2075-81.
van den Brandt PA, Goldbohm RA. Nutrition in the prevention of gastrointestinal cancer. Best
practice & research in clinical gastroenterology 2006;20:589-603.
van Grinsven HJM, Rabl A, de Kok TM. Estimation of incidence and social cost of colon
cancer due to nitrate in drinking water in the EU: a tentative cost-benefit assessment.
Environmental health 2010;9:Article Nr. 58.
− 91−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
van Leeuwen FX. Health impact of chemicals in food. WHO Consultation on Global Burden of
Foodborne Diseases. Geneva; 2006.
Van Lieshout EM, Van Doesburg W, Van der Meer R. Real-time PCR of host DNA in feces to
study differential exfoliation of colonocytes between rats and humans. Scand J Gastroenterol
2004;39:852-7.
Van Winckel M, Van de Velde SV, De Bruyne R, Van Biervliet S. Clinical practice: Vegetarian
infant and child nutrition. European Journal of Pediatrics 2011;170:1489-94.
Vandendriessche F. Meat products in the past, today and in the future. Meat Science
2008;78:104-13.
Vandevijvere S, Van Oyen H. Sodium intake in the Belgian population - Research limitations
and policy implications. Arch Public Health 2008;66:187-95.
Vandevijvere S, De Keyzer W, Chapelle JP, Jeanne D, Mouillet G, Huybrechts I et al. Estimate
of total salt intake in two regions of Belgium through analysis of sodium in 24-h urine samples.
Eur J Clin Nutr 2010;64:1260-5.
Vandevijvere S, De Vriese S, Huybrechts I, Moreau M, Temme E, De Henauw S et al. The
gap between food-based dietary guidelines and usual food consumption in Belgium 2004.
Public Health Nutrition 2009;12:423-31.
Vanhaecke L, Derycke L, Le Curieux F, Lust S, Marzin D, Verstraete W et al. The microbial
PhIP metabolite 7-hydroxy-5-methyl-3-phenyl-6,7,8,9-tetrahydropyrido [3_,2_:4,5]imidazo[1,2a]pyrimidin-5-ium chloride (PhIP-M1) induces DNA damage, apoptosis and cell cycle arrest
towards Caco-2 cells. Toxicology Letters 2008;178:61-9.
Vanham D, Mekonnen MM, Hoekstra AY. The water footprint of the EU for different diets
Ecological Indicators 2013; 32: 1-8.
Vanhauwaert E. De actieve Voedingsdriehoek. Uitgeverij Acco, Leuven. 2012. Available from:
URL:<http://issuu.com/vigez/docs/de_actieve_voedingsdriehoek>
van Meer S, Leufkens AM, Bueno-de-Mesquita HB, van Duijnhoven FJB, van Oijen MGH,
Siersema PD. Role of dietary factors in survival and mortality in colorectal cancer: a
systematic review. Nutrition Reviews 2013 ;71 :631-41.
Vaucher P, Druais PL, Waldvogel S, Favrat B. Effect of iron supplementation on fatigue in
nonanemic menstruating women with low ferritin: a randomized controlled trial. CMAJ 2012.
Ventanas S, Ventanas J, Jurado A, Estévez M. Quality traits in muscle biceps femoris and
back-fat from purebred Iberian and reciprocal Iberian x Duroc crossbred pigs. Meat Science
2006;73:651-59.
Verginelli F, Bishehsari F, Napolitano F, Mahdavinia M, Cama A, Malekzadeh R et al.
Transitions at CpG Dinucleotides, Geographic Clustering of TP53 Mutations and Food
Availability Patterns in Colorectal Cancer. Plos One 2009; 4: Art.No.e6824.
Viegas O, Amaro LF, Ferreira IM, Pinho O. Inhibitory Effect of Antioxidant-Rich Marinades on
the Formation of Heterocyclic Aromatic Amines in Pan-Fried Beef. Journal of Agricultural and
Food Chemistry 2012a;60:6235-40.
Viegas O, Novo P, Pinto E, Pinho O, Ferreira IM. Effect of charcoal types and grilling
conditions on formation of heterocyclic aromatic amines (HAs) and polycyclic aromatic
hydrocarbons (PAH) in grilled muscle foods. Food and Chemical Toxicology 2012;50:2128-34.
Vinnari M, Montonen J, Harkanen T, Mannisto S. Identifying vegetarians and their food
consumption according to self-identification and operationalized definition in Finland. Public
Health Nutrition 2009;12:481-88.
VLAM - Vlaams Centrum voor Agro- en Visserijmarketing. Marktinfo: vlees. Belgische
vleessector in cijfers.
Available from:
URL: <http://www.vlam.be/facts/info nl.phtml?id=7>
Vossen E, Doolaege EH, Moges HD, De Meulenaer B, Szczepaniak S, Raes K et al. Effect of
sodium ascorbate dose on the shelf life stability of reduced nitrite liver pates. Meat science
2012;91:29-35.
− 92−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Voutsinas J, Wilkens LR, Franke A, Vogt TM, Yokochi LA, Decker R et al. Heterocyclic amine
intake, smoking, cytochrome P450 1A2 and N-acetylation phenotypes, and risk of colorectal
adenoma in a multiethnic population. Gut 2013;62:416-22.
Wadge A, Pennington H, Usborne WR. Perspectives food safety challenges. Journal of the
Science of Food And Agriculture 2004;84:1079-82.
Waegeneers N, Thiry C, De Temmerman L, Ruttens A. Predicted dietary intake of selenium by
the general adult population in Belgium. Food Additives and Contaminants Part A. Chemistry
Analysis Control Exposure and Risk Assessment 2013;30:278-85.
Wang J, Joshi AD, Corral R, Siegmund KD, Le Marchand L, Martinez ME et al. Carcinogen
metabolism genes, red meat and poultry intake, and colorectal cancer risk. Int J Cancer
2012;130:1898–1907.
Wang Y, Beydoun MA. Meat consumption is associated with obesity and central obesity
among US adults. International Journal of Obesity 2009;33:621-28.
Watson AJM, Collins PD. Colon Cancer: A Civilization Disorder. Digestive diseases
2011;29:222-8.
WCRF - World Cancer Research Fund. WCRF global network's diet and cancer report. 2012.
Available from:
URL<http://www.dietandcancerreport.org/index.php>
WCRF/AICR - World Cancer Research Fund / American Institute for Cancer Research.
Second expert report- Food, Nutrition, Physical Activity and the Prevention of Cancer: a Global
perspective.
Research
Methodology
2007a.
Available
from:
URL:<http://www.dietandcancerreport.org/expert_report/scientific_process/methodology.php>
WCRF/AICR - World Cancer Research Fund / American Institute for Cancer Research.
WCRF/AICR Systematic Literature Review Continuous Update Project Report. 2011. Available
from:
URL:< http://www.wcrf.org/PDFs/Colorectal-cancer-CUP-report-2010.pdf>
WCRF/AICR - World Cancer Research Fund/American Institute for Cancer Research. Food,
Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective. 2007.
Available from: URL:<http://www.dietandcancerreport.org/cancer_resource_center/downloads/
Second_Expert_Report_full.pdf>
Weiss G. Iron metabolism in the anemia of chronic disease. Biochimica et Biophysica Acta
2009;1790:682–93.
Westbrook A.M, Szakmary A, Schiestl RH. Mechanisms of intestinal inflammation and
development of associated cancers: lessons learned from mouse models. Mutat Res
2010;705:40–59.
WHO – World Health Organisation. Diet, nutrition and the prevention of chronic diseases.
Report of a joint WHO/FAO expert consultation. WHO 2003;919:148.
WHO – World Health Organisation. Vitamin B12, Vitamin and mineral requirements in human
nutrition. WHO 2004;279-88. Available from:
URL:<(http://whqlibdoc.who.int/publications/2004/9241546123.pdf>
Wicki A, Hagmann J. Diet and cancer. Swiss Med Wkly 2011;141:w13250.
Williams CD, Satia JA, Adair LS, Stevens J, Galanko J, Keku TO et al.
Associations of Red Meat, Fat, and Protein Intake With Distal Colorectal Cancer. Risk Nutr
Cancer 2010;62:701-9.
Windey K, De Preter V, Verbeke K. Relevance of protein fermentation to gut health. Molecular
nutrition and food research 2012;6:184-96.
Windey K, De Preter V, Louat T, Schuit F, Herman J. Modulation of protein fermentation does
not affect fecal water toxicity: a randomized cross-over study in healthy subjects. PLoS ONE
2012a;7:e52387.
Winter J, Nyskohus L, Young GP, Hu Y, Conlon M, Bird A et al. High Red Meat-Induced
Promutagenic Adducts in the Mouse and Human Colon and Their Inhibition by Resistant
Starch. Environmental and Molecular Mutagenesis 2012;53: S1-S26.
− 93−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Winter J, Nyskohus L, Young GP, Hu Y, Conlon MA, Bird AR et al. Inhibition by Resistant
Starch of Red Meat-Induced Promutagenic Adducts in Mouse Colon. Cancer Pevention
Research 2011;4:1920-28.
Woolford G, Cassens RG. The fate of sodium nitrite in bacon. Journal of Food Science
1977;42:586-9.
Wu MC, Ma CY, Yang CC, Kao WC, Shen SC. The formation of IQ type mutagens from
Maillard reaction in ethanolic solution. Food chemistry 2011;125:582-7.
Wu SJ, Feng B, Li K, Zhu X, Liang SH, Liu XF et al. Fish Consumption and Colorectal Cancer
Risk in Humans: A Systematic Review and Meta-analysis. American Journal of Medicine
2012;125:551-69.
Xu XD, Yu ED, Gao XH, Song N, Liu LJ, Wei XB et al. Red and processed meat intake and
risk of colorectal adenomas: A meta-analysis of observational studies. International Journal of
Cancer 2013;132:437-48.
Yarnall JM, Crouch DJM, Lewis CM. Incorporating non-genetic risk factors and behavioural
modifications into risk prediction models for colorectal cancer Cancer Epidemiology 2013; 37:
324-329.
Yoshida K, Osawa K, Kasahara M, Miyaishi A, Nakanishi K, Hayamizu S et al. Association of
CYP1A1, CYP1A2, GSTM1 and NAT2 gene polymorphisms with colorectal cancer risk and
smoking. Asian Pacific Journal of Cancer Prevention 2008;8:438-44.
Yu H, Pardoll D, Jove R. STATs in cancer inflammation and immunity: a leading role for
STAT3. Nat Rev Cancer 2009;9:798–809.
Yurchenko S, Mölder U. Volatile N-nitrosamines in various fish products. Food Chem
2006;96:325-33.
Yurchenko S, Mölder U. The occurrence of volatile N-nitrosamines in Estonian meat products.
Food Chemistry 2007;100:1713-21.
Zanardi E, Ghidini S, Battaglia A, Chizzolini R. Lipolysis and lipid oxidation in fermented
sausages depending on different processing conditions and different antioxidants. Meat Sci
2004;66:415-23.
Zhang JJ, Dhakal IB, Zhao ZJ, Li L. Trends in mortality from cancers of the breast, colon,
prostate, esophagus, and stomach in East Asia: role of nutrition transition. European Journal
of Cancer Prevention 2012;21:480-9.
Zhang LQ, Zhou JN, Wang J, Liang GD, Li JY, Zhu YD et al. Absence of Association between
N-Acetyltransferase 2 Acetylator Status and Colorectal Cancer Susceptibility: Based on
Evidence from 40 Studies. PLoS ONE 2012a;7: e32425.
Zhang XH, Giovannucci EL, Smith-Warner SA, Wu K, Fuchs CS, Pollak M et al. A prospective
study of intakes of zinc and heme iron and colorectal cancer risk in men and women. Cancer
Causes and Control 2011;22:1627-37.
Zhang Y, Yu CD, Mei JB, Wang S. Formation and mitigation of heterocyclic aromatic amines
in fried pork. Food Additives and Contaminants Part A-Chemistry Analysis Control Exposure &
Risk Assessment 2013;30:1501-07.
Zhao Y, Han YS, Zhang L, Wang YC,Ma YS, Zhang F, Fu D, Wang XF. Quantitative
Assessment of the Effect of Cytochrome P450 2C9 Gene Polymorphism and Colorectal
Cancer. PLOS ONE 2013;8:Article Number:e60607.
Zhao ZQ, Guan QK, Yang FY, Zhao P, Zhou B, Chen ZJ. System review and meta-analysis of
the relationships between five metabolic gene polymorphisms and colorectal adenoma risk.
Tumor biology 2012;33:SI - 523-35.
Zheng W, Lee SA. Well-Done Meat Intake, Heterocyclic Amine Exposure, and Cancer Risk
Nutrition and cancer. International Journal 2009;61:437-46.
Zhong X, Fang YJ, Pan ZZ, Li B, Wang L,Zheng MC, Chen YM, Zhang CX. Dietary fat, fatty
acid intakes and colorectal cancer risk in Chinese adults: a case-control study .European
Journal of Cancer Prevention 2013;22:438-47.
− 94−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
Zhu Y, Peng ZQ, Wang M, Wang RR, Rui LM. Optimization of extraction procedure for
formaldehyde assay in smoked meat Products. Journal of Food Composition and Analysis
2012;28:1-7.
Zhu Y, Wu H, Wang PP, Savas S, Woodrow J, Wish T et al. Dietary patterns and colorectal
cancer recurrence and survival: a cohort study. BMJ Open 2013;3:e002270.
zur Hausen H. Red meat consumption and cancer: Reasons to suspect involvement of bovine
infectious factors in colorectal cancer. International Journal of Cancer 2012;130:2475-83.
− 95−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
5
RECOMMENDATIONS FOR FURTHER RESEARCH
Short of inconceivable randomized controlled clinical trials with colo-rectal cancer incidence as
outcome, the colorectal carcinogenic effect of red meat and processed red meats has been
demonstrated beyond doubt, both in epidemiology as well as in experimental work with both
animals and humans. It seems clear that the major carcinogen involved is heme although
considerable evidence points to the negative effect of heterocyclic amines formed by over-heating
red meat and apparent from an extreme brown/charred appearance. It is not clear however why
the carcinogenic effect of fresh red meats is only about half that of processed (cured) meats. In
Belgium, cured meats are almost exclusively derived from pig meat and both the higher fat and
salt content compared to fresh meat may be involved. Further research on the issue is clearly
required.
Also, in view of the newer insights:
-
contrasting health effects of individual foods vs. those of a dietary pattern both in intervention
trials with animals or, preferably, humans using CRC markers and using in vitro digestive
systems
-
the possibilities for animal production, meat processing and domestic food preparation to
incorporate cancer mitigating components and /or processes
(applied) research in these areas should be promoted.
Work should preferably involve:
-
the development of « functional meat products » incorporating components mitigating
carcinogenesis through animal (pig) feeding (e.g. plant derived antioxidants) and/or meat
processing (e.g. Calcium salts, fibrous components, minor plant components, ..).
-
experiments testing such diets/products fed to animals (e.g. rodents, pigs) or to in vitro
digestive systems evaluating colon epithelial changes and/or oxidative status of digestive
contents.
-
intervention experiments with humans involving testing of processed red meats, analogous to
e.g. the recent work described in Windey et al (2012a)
Also in Belgium, research along these lines has recently been initiated by the Federal Public
Service (FPS) Health, Food Chain Safety and Environment: RF 11/6250 MEATNOX “Vorming en
(geno)toxische activiteit van nitros(yl)atie- en oxidatieproducten in het gastrointestinaal stelsel: rol
van nitrietgepekelde vleesproducten en preventie.”
− 96−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
6
COMPOSITION OF THE WORKING GROUP
All experts joined the working group in a private capacity. The names of the members and
experts of the Superior Health Council are indicated with an asterisk*.
The following experts were involved in drawing up the advice :
DE BACKER Guy*
DE HENAUW Stefaan*
DELZENNE Nathalie*
DEMEYER Daniel
DE SMET Stefaan
HERMAN Lieve
MAGHUIN-ROGISTER Guy*
MERTENS Birgit
PAQUOT Nicolas*
PEETERS Marc
VANCAMP John*
Preventive medicine, public health, epidemiology
Public health nutrition
Nutrition, toxicology
Nutrition, animal production&meat technology
Animal nutrition and animal product quality
Technology and food
Food analysis
Toxicology, genotoxicity
Nutrition, metabolic and endocrine systems
Oncology
Nutritional value of food, nutrition and health
UGent
UGent
UCL
UGent
UGent
ILVO
ULg
WIV
ULg
UZA
UGent
The working group was chaired by Guy MAGHUIN-ROGISTER, the scientific secretary was
Michèle ULENS.
− 97−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be
About the Superior Health Council (SHC)
The Superior Health Council is a federal body that is part of the Federal Public Service Health,
Food Chain Safety and Environment. It was founded in 1849 and provides scientific advisory
reports on public health issues to the Ministers of Public Health and the Environment, their
administration, and a few agencies. These advisory reports are drawn up on request or on the
SHC's own initiative. The SHC takes no decisions on the policies to follow, nor does it implement
them. It does, however, aim at giving guidance to political decision-makers on public health
matters. It does this on the basis of the most recent scientific knowledge
Apart from its 25-member internal secretariat, the Council draws upon a vast network of over 500
experts (university professors, members of scientific institutions), 200 of whom are appointed
experts of the Council. These experts meet in multidisciplinary working groups in order to write
the advisory reports.
As an official body, the Superior Health Council takes the view that it is of key importance to
guarantee that the scientific advisory reports it issues are neutral and impartial. In order to do so,
it has provided itself with a structure, rules and procedures with which these requirements can be
met efficiently at each stage of the coming into being of the advisory reports. The key stages in
the latter process are: 1) the preliminary analysis of the request, 2) the appointing of the experts
within the working groups, 3) the implementation of the procedures for managing potential
conflicts of interest (based on the declaration of interest, the analysis of possible conflicts of
interest, and a referring committee) and 4) the final endorsement of the advisory reports by the
Board (ultimate decision-making body). This coherent set of procedures aims at allowing the SHC
to issue advisory reports based on the highest level of scientific expertise available whilst
maintaining all possible impartiality.
The advisory reports drawn up by the working groups are submitted to the Board. Once they have
been endorsed, they are sent to those who requested them as well as to the Minister of Public
Health and are subsequently published on the SHC website (www.shc-belgium.be), except as
regards confidential advisory reports. Some of them are also communicated to the press and to
target groups among healthcare professionals.
The SHC is also an active partner in developing the EuSANH network (European Science
Advisory Network for Health), which aims at drawing up advisory reports at the European level.
In order to receive notification about the activities and publications of the SHC, you can send a
mail to [email protected]
− 98−
Superior Health Council
rue de l’Autonomie 4 ● 1070 Brussels ● www.shc-belgium.be